Allergies are typically diagnosed based on detailed history elicited from a patient. Confirmation of the diagnosis by allergy skin or in vitro testing is sometimes also helpful. The authors discuss several physical examination features, specifically in the head and neck region, that are often suggestive of allergy presence.
Nearly one-third of the population in the United States reports nasal and ocular symptoms of allergy. As ear, nose, and throat physicians, we have a unique role in helping these patients. Many allergic symptoms manifest in the head and neck. The term allergic rhinitis is used as a diagnosis for patients with nose and eye symptoms secondary to IgE-mediated, or type 1 hypersensitivity reactions to various antigens. Atopic IgE-mediated allergic reactions can occur throughout the body; however, inhalant allergy is usually limited to the nose, eyes, and lungs.
A thorough history of a patient’s symptoms will often include symptoms both localized in areas such as the eyes or throat as well as systemic symptoms. History alone is often sufficient to make the diagnosis of allergic rhinitis. Confirmation can be obtained in the form of skin or in vitro testing for better-guided avoidance measures as well as appropriate institution of immunotherapy. Though arguably not as important as history, the physical examination can also be a helpful adjunct in diagnosing allergy. The authors present several head and neck physical examination findings the otolaryngologist will likely encounter in the examination of the allergic patient.
Nasal examination
Optimal nasal examination for an allergic evaluation includes the use of a nasal speculum and headlight as well as inspection of the nasal skin and the patient’s behavior. Nose blowing, wiping, sneezing, and sniffing are commonly seen in the allergic patient with acute symptom exacerbation.
Nasal Drip and Nasal Crease
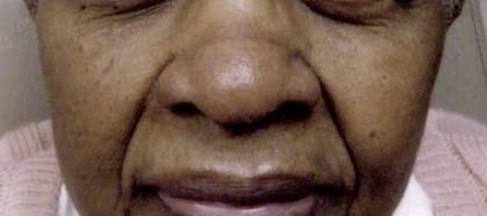
Clear nasal secretions can be copious in allergic rhinitis ( Figs. 1 and 2 ). Some patients develop a pattern of wiping the nose with the palm of their hand leading to the term the “allergic salute.” These patients may also develop a horizontal crease in the nasal supratip area called an allergic nasal crease.

Pale and Boggy Inferior Turbinates
The nasal mucosa of the inferior turbinates often becomes edematous without erythema after inhalant allergen exposure leading to a pale or blue appearing surface ( Fig. 3 ). The turbinates can become significantly swollen and obstruct the nasal airway and are typically surrounded by copious clear mucus.

Red Inferior Turbinate
Reddened nasal mucosa is less frequently associated with inhalant allergy ( Fig. 4 ). The differential diagnosis for red turbinates includes exposure to cigarette smoke (either active or second hand), overuse of topical decongestants, or (in the senior author’s experience) food allergy.
Nasal Polyposis
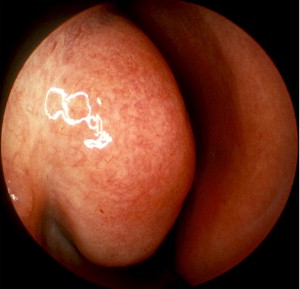
Whereas atopy alone as the cause of nasal polyp development is controversial, the presence of IgE to various antigens has certainly been identified in nasal polyp specimens ( Fig. 5 ). Many patients with nasal polyps also exhibit positive skin testing or in vitro IgE to inhalant allergens. Wise and colleagues discussed a population of patients with high nasal-IgE levels and nasal polyps and negative skin or in vitro allergy testing. The higher sensitivity of detecting local IgE production in the nose may allow better treatment of truly allergic nasal polyp patients with negative conventional testing.

Adenoid Hypertrophy
Inflammatory mediators in nasal secretions of the allergic patient can lead to enlargement of the lymphoid tissue within the nasopharynx also known as adenoid tissue ( Fig. 6 ). This is more common in the pediatric patient and can be a significant source of nasal obstruction, sleep disordered breathing, and bacterial rhinosinusitis in untreated allergic children.




