Photography and Documentation of Pathologic Findings
Steven D. Rauch
Jeffrey H. Spiegel
Continuing advances in imaging technology enable the physician to supplement medical record narratives and sketches with conventional and digital photographs, slides, and video recordings of physical findings. This chapter will present and discuss the rationale, principles, and techniques of photo documentation as they apply to otology. For a more detailed tutorial on many topics in standard medical photography, the reader is referred to general texts on the subject, such as that by Hansell (1).
REASONS FOR PHOTODOCUMENTATION
Photo documentation provides a visual record of physical findings at the time of patient examination. Regardless of the medium—still photograph, slide, or video—it is an eloquent record rarely equaled by narrative description. Patient care is undeniably improved by such objective documentation. Issues of interval assessment of change, as well as communication between doctor and patient or between physicians are facilitated. Furthermore, this record is available for research and teaching purposes even when the patient is not. There are also obvious medicolegal benefits that accrue from careful record keeping in general and from photographic records specifically, because once the physical appearance of the patient is altered by time, pathology, or surgical intervention, there is no other means of demonstrating interval change. These three uses of photodocumentation—patient care, education and research, and medicolegal—are compelling reasons to include patient imaging as one of the standards of care.
GENERAL PRINCIPLES OF MEDICAL PHOTOGRAPHY
Patient Consent
There are certain general principles of photodocumentation in the medical record that apply regardless of specialty or subject matter. As part of the medical record, the patient’s photograph is subject to the same considerations of confidentiality as any other personal medical document. This includes accuracy of labeling (patient’s name, medical record number, and date) and restriction of access to only those individuals with a legitimate need to review the data to provide patient care. Any other use of the photographic record, such as for teaching or publication, requires the patient’s consent. Obviously, if there are any features of the clinical photograph permitting identification of the patient, written consent is mandatory and masking of identifying features is appropriate prior to presentation or publication. Adoption of a simple, standardized photographic consent form for office use is an excellent idea. These forms are readily available from any hospital audiovisual department, as are general guidelines regarding issues of consent as they relate to photographic records. The clinician can consider incorporating an imaging consent form into the standard paperwork completed by each patient.
Standardization of Composition
Because one of the major applications of photodocumentation is for interval assessment of physical findings, it is imperative that variables of lighting, magnification, and angle of view be consistent between images. This is accomplished simply by adoption of office standards for photographic equipment, setting, and conditions. Standards should include a designated format (standard, digital, or both), choice of film or camera settings, light source, lenses, and distance from subject for each common subject photographed. For instance, all external ear (pinna) photographs should be taken using a macro lens at a 1:4 view ratio (as read from the lens barrel or a film-based camera), direct flash lighting, and automatic shutter speed and f-stop exposure settings for the particular film type chosen. Similarly, endoscopic photographs of the ear canal and tympanic membrane should be obtained at a standard zoom setting of 90 to 120 mm (depending on physician preference [Fig. 2.1]) using an automatic
exposure setting coupled to stroboscopic flash illumination generated by the light source. For digital imaging, a standard composition and focal length, along with uniform settings and resolution, are necessary. The key here is internal consistency among photographs within the office. It is not strictly necessary to adopt the same routine as that used in another setting. It is advisable to record camera equipment and setting information, however, to permit duplication of results by others if necessary. Exposure settings and equipment information should also be recorded in those cases in which photographs are taken of unusual subject matter. For example, in a patient with a genetic syndrome, photographs of associated skeletal or ophthalmic anomalies might be desirable but have not been standardized in an otology office.
exposure setting coupled to stroboscopic flash illumination generated by the light source. For digital imaging, a standard composition and focal length, along with uniform settings and resolution, are necessary. The key here is internal consistency among photographs within the office. It is not strictly necessary to adopt the same routine as that used in another setting. It is advisable to record camera equipment and setting information, however, to permit duplication of results by others if necessary. Exposure settings and equipment information should also be recorded in those cases in which photographs are taken of unusual subject matter. For example, in a patient with a genetic syndrome, photographs of associated skeletal or ophthalmic anomalies might be desirable but have not been standardized in an otology office.
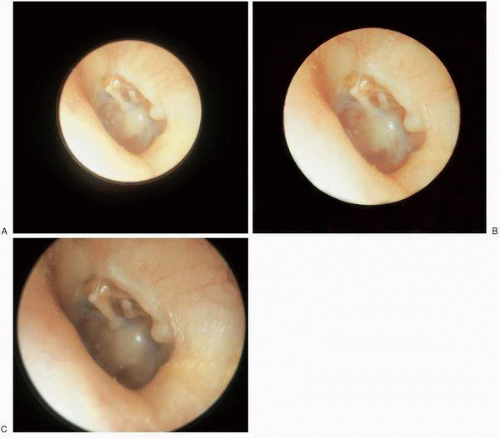 FIG. 2.1 Effect of different focal length on ratio of image size to negative size. Longer focal length increases relative image size but clips top and bottom of field. Chronic otitis media with effusion and “nature’s” type III tympanoplasty. A: 90-mm focal length. B: 100-mm focal length. C: 120-mm focal length. |
PHOTOGRAPHIC STUDIO
Although a room dedicated to photography may not be feasible, it is advantageous to have some dedicated space (even in the form of a locking, rolling cabinet) for picture taking and for equipment storage. Equipment maintenance is critical for protecting the investment in hardware and for sustaining optimum picture quality. Dedicated space ensures minimum wear and tear on equipment from setup and breakdown time, transportation, and rough handling. An office
studio space also facilitates standardization of patient positioning and lighting. In many cases an adequate “studio” can consist of a blue backdrop against a wall in an area of the office with appropriate lighting. A smooth, organized, and efficient photography routine lends an air of professionalism that is reassuring to patients.
studio space also facilitates standardization of patient positioning and lighting. In many cases an adequate “studio” can consist of a blue backdrop against a wall in an area of the office with appropriate lighting. A smooth, organized, and efficient photography routine lends an air of professionalism that is reassuring to patients.
PRINCIPLES OF PHOTOGRAPHIC COMPOSITION
Appreciation of the general effects of lighting, film, color, and composition on the photographic record is essential. Lighting may be provided by ambient room light, an assortment of camera-mounted or freestanding flash devices, fiber-optic cable (in the case of endoscopic photography), or studio lights. Most film is color-balanced for daylight, a true white light compared with the yellow of incandescent (tungsten) light or green of fluorescent lights. Ambient light rarely provides adequate illumination and often introduces unpleasant color distortion because of mismatch between the color temperature of the light and the color balance of the film. Aside from the obvious need for adequate illumination for the subject, the major consideration in choice of lighting is shadow. The nearer the light source to the axis of view from subject to camera lens, the less shadow is thrown across the field of view. The more oblique the incident light upon the subject, the longer the shadow (Fig. 2.2). In a two-dimensional photograph, the major source of depth cuing is shadow. A long shadow from oblique lighting tends to enhance surface textural detail while obscuring or distorting color. Coaxial illumination (as provided by a “ring flash” or through an endoscope) results in a uniformly lighted subject and elimination of shadows, which provides excellent color detail but “flattens” all surface texture. Coaxial illumination is best used for objects within an orifice, such as the mouth or ear canal. Oblique lighting is excellent for demonstrating surface detail, as in rashes or other skin lesions. General surface photography of surgical fields, body parts, or portraiture is best achieved by a compromise using diffused lighting located 30 to 60 degrees above the subject and slightly to one side (so-called ¾ lighting), simulating midmorning sunlight.
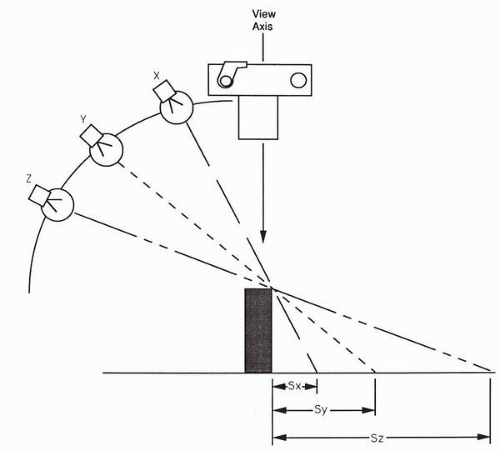 FIG. 2.2 Effect of angle of incidence of illumination on shadow length. As the angle of incidence of illumination becomes progressively more oblique, the shadow length (S) becomes progressively longer. Longer shadows enhance surface textural detail, whereas shorter shadows provide more even illumination. |
Photo composition has both aesthetic and practical aspects. The inclusion of some object or structure to provide a sense of scale or relative size and to provide anatomic orientation for the viewer is particularly important when photographing a surgical field (Fig. 2.3). Much of the region is beneath the drapes and the viewer may literally not know which end is up. The simple inclusion of a chin, nose, or ear lobe may be all that is necessary to orient the viewer. Another practical objective of photographic composition is to lead the viewer’s eye to the important aspects of the subject. Aside from including the subject of interest and features for scale
and orientation, all other extraneous items are distracting and should be excluded. Surgical instruments, sponges, and surgeon’s fingers should be excluded from photographs of surgical fields or specimens. Panoramic views are inappropriate when the area of interest is small, such as showing the entire side of the head if the pinna is the subject of interest.
and orientation, all other extraneous items are distracting and should be excluded. Surgical instruments, sponges, and surgeon’s fingers should be excluded from photographs of surgical fields or specimens. Panoramic views are inappropriate when the area of interest is small, such as showing the entire side of the head if the pinna is the subject of interest.
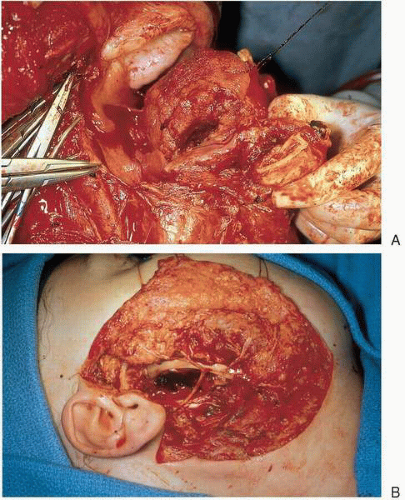 FIG. 2.3 Composition greatly influences the effectiveness with which the photograph communicates information. A: Poor composition. Composite resection of right mandible and neck. Note lack of landmarks to orient viewer to relevant anatomy, as well as distracting instruments and bloody glove. B: Picture is visually simple, provides landmarks for orientation and scale, and avoids distracting objects or panoramic view. |
Aesthetic aspects of photographic composition are harder to define. In portrait views, one should try to capture a pleasant facial expression with a slight smile and both eyes open. Intraoperative photographs should avoid depiction of excessively bloody surgical fields by covering the perioperative site with clean towels, cleaning any visible surgical instruments, and putting clean gloves on hands that will remain in the picture. Gratuitously grotesque photographs of injuries, lesions, or intraoperative defects are to be discouraged unless they specifically make a point or document an important feature of the case, such as tumor margins or anatomic variation. Adherence to a general effort to obtain visual simplicity with the minimum subject size that clearly portrays the field of interest and adequately orients the viewer will usually result in good photodocumentation.
Choice of Film
Many options for choice of film are available. Film for color prints or slides are available in a variety of speeds (ASA rating). The “faster” the film, the more light sensitive it is and therefore the less light or exposure time necessary to obtain the picture. However, faster film tends to be slightly lower resolution or “grainier” and also have less color saturation. Film in the ASA 100 or 200 range is a good compromise between the features of speed, resolution, and color saturation. Different films also have different color balance. In other words, the apparent color saturation will vary in different parts of the color spectrum. Generally, Kodachrome (Eastman Kodak Co., Rochester, NY) tends to have very rich reds, whereas Ektachrome (Eastman Kodak Co., Rochester, NY) has a bluish cast and Fujichrome (Fuji Photo Film Co., Ltd., Tokyo) emphasizes greens and yellows. If there is a lot of red color in the subject, a film rich in red (such as Kodachrome) may fail to show good differentiation of subtle color differences, whereas a “cooler” bluish Ektachrome film may resolve subtle red shadings better. Kodachrome is the gold standard for archival storage of photographic records. It is known to be color stable for decades. Ektachrome is less stable and, even under ideal storage conditions, will fade over many years. Kodachrome and Ektachrome have different processing requirements as well. Kodachrome uses a chemical sequence known as C41 that is time-consuming and available only at larger processing laboratories. Ektachrome uses E6 processing, which is rapid and widely available in many small photofinishing operations and often on site in hospital audiovisual departments. As a result, Ektachrome slides are usually available within 24 hours or less, whereas Kodachrome slides typically have a 5- to 10-day turnaround time from shooting to viewing. Choosing among the different films is ultimately a personal choice based on these considerations of color balance, longevity, and rapidity of processing.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


