Photodynamic Therapy of Early Laryngeal Cancers
Merrill A. Biel
INTRODUCTION
Cancer of the larynx accounts for 25% to 30% of all cancers of the head and neck. Early cancers of the larynx (Tis, T1, T2) and severe dysplasia are presently treated with either radiation therapy or surgery alone. Five-year cure rates achieved with this therapy, including surgical salvage, are 75% to 90%. Radiation therapy has the advantage of preserving the physical integrity of the larynx, thereby preserving the voice. Radiation therapy, however, has significant disadvantages even when small laryngeal fields of radiation are used. These disadvantages include discomfort and mucositis during and for potential prolonged periods after therapy, permanently altered quality of the voice, dysphagia, chondroradionecrosis of the larynx and trachea, and the extensive length of therapy (6 to 7 weeks). Surgical therapy for early cancers of the larynx, T1 and T2, includes performing a partial cordectomy or hemilaryngectomy. Although cure rates are high, surgical removal of portions of the vocal cord or hemilarynx results in significant alteration of the quality of the voice.
Severe dysplasia and Tis may also be treated with either radiation or limited surgery with either microsurgical techniques or laser excision. Le reported on 82 patients with Cis Tis of which 15 were treated with vocal cord stripping with a 56% local control rate, 13 were treated with extensive laser resection/hemilaryngectomy with a 71% local control rate, and 54 were treated with radiotherapy with a 79% local control rate. Involvement of the anterior commissure was a significant negative prognostic factor. Subjective quality of the voice was good to excellent in 73% of patients who underwent vocal cord stripping, 40% of those who underwent extensive resection, and 68% who underwent radiation therapy. Zeitels reported on seven patients with Tis undergoing microsurgical resection. Two patients developed subsequent microinvasive cancer requiring more aggressive treatment. Smith reported on 25 patients with Tis treated with surgical resection with an 88% cure rate. Sittel reported on laser excision of vocal cord cancers and noted significant effect on the quality of the voice with anterior commissure resections even when done in a staged fashion. Chone reported on 48 patients with early cancer of the glottis treated with laser microsurgical resection. He noted a 79% local control rate and a 96% laryngeal preservation rate. Rucci presented the results of 81 patients treated with CO2 laser therapy for Cis Tis and T1 glottic cancers and noted a 35% recurrence rate.
Garcia-Serra reported on 30 patients with Tis treated with radiotherapy with an 88% local control rate. Review of the literature for radiotherapy of Tis demonstrated an 87.4% weighted local control rate at 5 years on 705 patients in 22 published reports.
Review of 10 reports of laser excision treatments of Tis demonstrated an 82.5% control rate in 177 patients. Many patients required multiple laser excisions.
Damm reported on 29 patients with Tis treated with laser excision. Seventy-six percent (22/29) required more than one laser excision for persistence of disease, 9 of which were in the anterior commissure. Two-year disease-free survival was 86%. Dysphonia was reported in all patients, and none had improved quality of the voice over the pretreatment state. A review of the literature of control rates of various treatments for Tis were as follows: laser excision (104 patients) 20% initial failure rate, 1% loss of the larynx; vocal cord stripping (235 patients) 34% failure rate, 12% loss of the larynx; and radiotherapy (481 patients) 16% failure rate, 7% loss of
the larynx. The literature therefore demonstrates that surgical techniques to treat Tis are best limited to those patients in whom the Tis does not involve the anterior commissure or both vocal cords.
the larynx. The literature therefore demonstrates that surgical techniques to treat Tis are best limited to those patients in whom the Tis does not involve the anterior commissure or both vocal cords.
Hafidh presented the results of 150 patients treated with radiotherapy for T1/T2 glottic cancers. Seventy-one percent of T1 and 63.3% of T2 cancers were controlled with radiotherapy with an average follow-up of 37 months. Hartl presented a review of treatment options for cancer of the glottis and using primary radiotherapy noted a 43% to 91% control rate for T1 cancers and a 50% to 85% control rate for T2 cancers.
Batalla performed a study of the quality of the voice in patients who underwent endoscopic laser surgery and radiotherapy for T1 glottic cancer and noted that the quality of the voice was affected both by surgery and radiotherapy, although there was a reduced impact on the patient’s perception of the quality of the voice after radiotherapy.
The optimal treatment for severe dysplasia and early cancer of the larynx would be one that is effective, safe, repeatable, minimally invasive, nonsurgical, and a less time-consuming therapy than radiotherapy. Photodynamic therapy (PDT) is potentially such a treatment for severe dysplasia and early cancers of the larynx.
Photodynamic Therapy
PDT is a minimally invasive treatment involving the use of a photosensitizing drug and laser light for the treatment of a variety of cancers. When administered, these compounds are accumulated and retained to a greater degree in malignant tissues than normal tissues. The drugs remain inactive until exposed to a specific wavelength of light. The light, usually from a laser, is transmitted through specially modified fiber optics and activates the drug. The resulting photochemical reaction results in the production of oxygen radicals, thereby destroying diseased cells with little effect on normal tissues.
To date, PDT has been used to treat cancers in many organs, and Photofrin-based PDT has been approved by the U.S. FDA to treat early- and end-stage endobronchial and esophageal squamous cell cancers and Barrett dysplasia. Photofrin (porfimer sodium) concentrates in malignant tissue, is activated by penetrating light (630 nm + 3 nm), produces fluorescence, and is photochemically efficient. Photofrin has produced only one major adverse reaction as a result of its use: light sensitivity. Importantly, the use of Photofrin PDT to treat early cancer of the head and neck has been promising.
The generally accepted mechanism of action of PDT is that there is an energy transfer process from the light activated or excited triplet state of the photosensitizer to oxygen producing singlet oxygen, which in turn causes irreversible oxidation of some essential cellular component. It has also been shown that the vasculature changes within the tumor necrosis subsequent to PDT result in ischemia that is responsible for tumor necrosis. Either or both are sufficient to explain the remarkable necrosis of tumors within 2 to 5 days following PDT with Photofrin.
PDT has been demonstrated to be effective in the treatment of early cancers of the head and neck. The advantage of PDT therapy for early cancers of the larynx is the ability to preserve normal endolaryngeal tissue while effectively treating the cancers. This results in improved function of the larynx and the quality of the voice. Furthermore, PDT requires a short duration of therapy as compared to radiation therapy, is repeatable, carries less risk than surgical therapy, and is performed as an outpatient noninvasive treatment. Importantly, the use of PDT does not preclude the use of radiotherapy or surgery in the future for new primary or recurrent disease.
CLINICAL EXAMPLE
HISTORY
A 71-year-old male presents with a history of recurrent hoarseness. Two years prior he noted hoarseness and on medical workup was noted to have a hyperkeratosis of the right vocal cord. He underwent microlaryngoscopy and CO2 laser excision of the right vocal cord lesion that on pathology demonstrated right vocal cord severe dysplasia. He then presented 2 years later with onset of hoarseness. There was no sore throat, dysphagia, hemoptysis, or shortness of breath.
PHYSICAL EXAMINATION
On laryngoscopy, he was noted to have a hyperkeratotic lesion along the right anterior vocal cord with surrounding induration. The lesion extended up to the anterior commissure and there was a slight area of hyperkeratosis along the free edge of the left anterior vocal cord, just opposite from the right vocal cord lesion. There was no cervical lymphadenopathy. Biopsies were obtained under microlaryngoscopy. The right vocal cord lesion histologically was a microinvasive squamous cell carcinoma, and the left anterior vocal cord lesion histologically demonstrated hyperkeratosis with moderate premalignant dysplasia. He was therefore staged as a recurrent T1aN0 squamous cell cancer of the right vocal cord with premalignant dysplasia on the anterior left vocal cord.
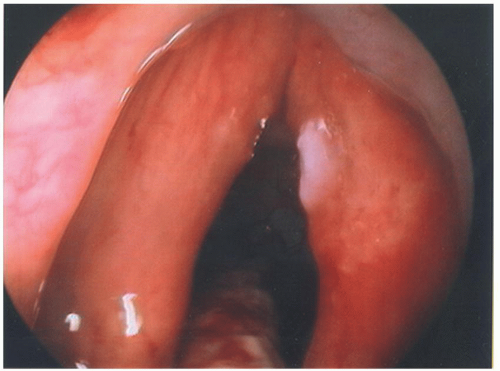 FIGURE 35.1 Recurrent squamous cell carcinoma of the right vocal cord T1a and dysplasia of the left anterior vocal cord. |
PREOPERATIVE MANAGEMENT
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


