Purpose
To compare a theoretical pharmacokinetic model of triamcinolone acetonide after posterior sub-Tenon’s injection with experimental serum and undiluted vitreous triamcinolone acetonide concentrations obtained during pars plana vitrectomy.
Design
Clinical-practice, prospective, interventional case series study.
Methods
This study compared computer-modeled triamcinolone acetonide diffusion after posterior sub-Tenon’s injection with triamcinolone acetonide levels in experimental undiluted vitreous and serum samples from 57 patients undergoing vitrectomy assessed via mass spectrometry and high-pressure liquid chromatography. At least 5 pairs of samples were collected at each of 7 time points (1 day, 3 days, and 1, 2, 3, 4, and 8 weeks) after triamcinolone acetonide injection, with 6 controls without injection. Cortisol levels were measured in 31 sets of samples.
Results
The theoretical model predicted that triamcinolone acetonide levels in systemic blood, vitreous, and choroidal extracellular matrix would plateau after 3 days at 15 ng/mL, 227 ng/mL and 2230 ng/mL, respectively. Experimental vitreous levels of triamcinolone peaked at 111 ng/mL at day 1, then reached a plateau in the range 15 to 25 ng/mL, while serum triamcinolone levels peaked at day 3 near 35 ng/mL and plateaued near 2 to 8 ng/mL. Serum triamcinolone and cortisol levels were inversely correlated (Spearman −0.42, P = .02).
Conclusions
The theoretical model predicts efficient delivery of triamcinolone acetonide from the posterior sub-Tenon’s space to the extracellular choroidal matrix. The experimental findings demonstrate low levels of serum triamcinolone that alter systemic cortisol levels and higher vitreous levels lasting at least 1 month. Both assessments support trans-scleral delivery of posterior sub-Tenon’s triamcinolone.
Triamcinolone acetonide is a long-acting corticosteroid depot that has been used extensively in ophthalmology. Traditionally, it has been delivered by periocular injection into the subconjunctival or posterior sub-Tenon’s space to treat a variety of conditions ranging from uveitis to cystoid macular edema. More recently, triamcinolone has been injected directly into the vitreous in the treatment of such conditions as diabetic macular edema, retinal vein occlusions, neovascular age-related macular degeneration (AMD), and reducing refractory cystoid macular edema in the short term, particularly in patients with uveitis. However, intravitreal-delivered steroid carries significant complication risks such as the elevation of intraocular pressure (IOP) and progression of cataract. Thirty percent of patients experienced elevated IOP requiring antiglaucoma medications and reported cataract progression in 13% to 30% of cases that often required surgery within 1 year of triamcinolone acetonide injection. In disease processes that primarily involve the choroid, such as macular degeneration, posterior sub-Tenon’s injection of triamcinolone may be a lower-risk method for long-acting steroid delivery compared to intravitreal injection. Therefore, a better understanding of the ocular and systemic pharmacodynamics of posterior sub-Tenon’s triamcinolone may be useful in devising novel treatment strategies for inflammatory, oxidative, and ischemic choroidal diseases such as AMD.
Recent clinical investigations of the relative therapeutic merits of intravitreal and sub-Tenon’s triamcinolone acetonide in patients with uveitic macular edema have shown inconclusive results, with Choudhry and Ghosh finding no significant difference in final visual acuity outcomes. Understanding the mechanism at work in both modes of delivery might help to evaluate their clinical relevance. In general, vitreous steroid concentrations have been lower and more variable following sub-Tenon’s delivery. However, the heterogeneity of triamcinolone pharmacokinetic studies has made these comparative assessments tenuous. Studies have varied greatly in follow-up duration, study size, study design, the amount of corticosteroid initially delivered, and the differing methods of steroid concentration analysis. Similarly designed studies by Mason and associates and Beer and associates have differed by numerous orders of magnitude in their findings. Furthermore, the systemic absorption of the steroid following sub-Tenon’s injection has also become a major concern because of its possible influence on patients with metabolic diseases such as diabetes. Recent studies have indicated that systemic absorption of triamcinolone following sub-Tenon’s injection occurs at levels sufficient to affect metabolic control in some patients, which would pose a significant risk factor in their use. Degenring and associates warn of the systemic effects of triamcinolone acetonide following their intravitreal injections, despite finding less systemic triamcinolone absorption compared with sub-Tenon’s assessments.
In this study, we sought to answer the following questions: 1) What are the pharmacokinetics of posterior sub-Tenon’s triamcinolone acetonide in the serum and vitreous? 2) What is the route of entry of posterior sub-Tenon’s triamcinolone acetonide into the eye? 3) Are there systemic side effects of posterior sub-Tenon’s triamcinolone acetonide delivery? To answer these questions, we developed an ocular simulation model that could be used to predict the serum, choroidal, and vitreous concentrations of triamcinolone acetonide after sub-Tenon’s injection. We then compared these predictions with the triamcinolone acetonide levels in both serum and undiluted vitreous samples obtained at the time of vitrectomy in patients who had previously received sub-Tenon’s steroid injection. In order to study the effects of systemic triamcinolone on the pituitary adrenal axis we also measured serum cortisol levels. To the best of our knowledge this study is the most comprehensive study to date on the serum and vitreous pharmacokinetics after posterior sub-Tenon’s injection for the time points 1 day to 56 days. In addition, this is the first study to assess the effects of systemic triamcinolone acetonide on cortisol levels. We anticipate that this study will to help clarify much of the debate surrounding the mechanism of action and the pervasive variability of the literature.
Methods
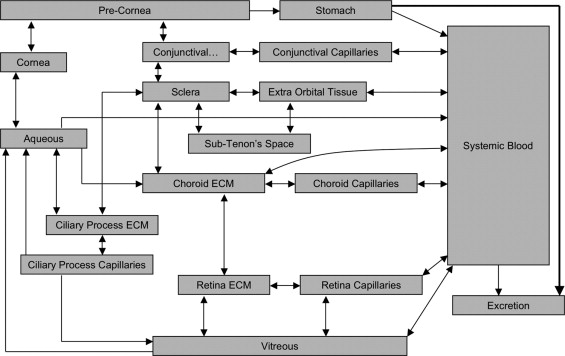
In silico modeling of posterior sub-Tenon’s triamcinolone acetonide was carried out using an ocular simulation (OCUSIM; Bend Research, Inc, Bend, Oregon, USA) computer program. The governing principles and assumptions used were: 1) ocular bioavailability determines overall systemic absorption and bioactivity; 2) site of deposition and physicochemical properties of triamcinolone acetonide may dictate rates of dissolution, absorption, metabolism, and elimination; 3) posterior sub-Tenon’s triamcinolone acetonide has high hepatic first-pass inactivation, whereas there is no first-pass metabolism via ocular route; and 4) no standardized methods exist for testing dissolution rates from sub-Tenon’s injection. The multiple compartments used in this model are shown in Figure 1 . Physiological and anatomic parameters for the ocular simulation were customized to model the human eye by entering appropriate volumes of distribution and surface areas of posterior compartment tissues. The physicochemical and physiological parameters of triamcinolone acetonide used in the ocular simulation were its logP (estimated partition coefficient in an n-octanol/water system: value 2.53), ocular pigment binding (estimated, following the method by Koeberle and associates, to be very low from equilibrium sepia melanin association: values with capacity of 7 × 10 4 (ng/g)(mL), K on of 3 × 10 −6 (mL/ng)(s), and K a of 7 × 10 −9 mL/ng), and systemic clearance (37 L/hr and t½ of 2 hr) following intravenous administration. Formulation characteristics were adapted from Kenalog-40 (Bristol-Myers Squibb, Princeton, New Jersey, USA): 1) saturation concentration of 1.3 × 10 4 ng/mL, 2) spherical suspension particles with an average radius of 1 × 10 4 nm, 3) total dose potency of 40 mg/mL, 4) particle density of 1.2 g/mL, and 5) estimated dissolution rate of 1 × 10 −6 cm 2 /s. Based on these parameters, theoretical calculations were carried out for a 40-mg posterior sub-Tenon’s triamcinolone acetonide injection.
To reduce postoperative inflammation and cellular reproliferation, patients are routinely given preoperative sub-Tenon’s triamcinolone acetonide between 1 and 56 days prior to vitrectomy surgery for epiretinal membrane or macular hole. In our study, this procedure was performed as described by Nozik. Briefly, a cotton tip soaked in proparacaine 0.5% is placed under the lid in the superotemporal quadrant of the eye for approximately 5 minutes. One drop of a fourth-generation floroquinolone is given topically every minute times 3. A ¾-inch 25-gauge needle on a 1-cc syringe is placed in the fornix superotemporally with the bevel towards the globe. The tip of the needle is moved side to side as it is moved posteriorly along the sclera, ending in a position immediately behind the macula. During the introduction of the needle, the limbal vessels are carefully observed for synchronous lateral movements that would indicate engagement of the needle with the sclera. Forty milligrams of triamcinolone acetonide (Kenalog-40; Bristol-Myers Squibb), in 1 cc, are then injected slowly into the posterior sub-Tenon’s space.
Undiluted vitreous and serum samples were collected based on a previously established technique. Prior to turning on the infusion to start the vitrectomy, the vitreous cutter was used to obtain 0.5 to 1 cc of undiluted vitreous specimen. A 3-cc syringe on a 3-way stopcock was used to provide manual aspiration of the specimen. Once a sufficient volume of vitreous was obtained, the infusion was turned on and the stopcock was rotated and the vitrectomy was continued. Patients were monitored for complications, specifically severe increases in IOP between posterior sub-Tenon’s administration and immediately postoperatively. The number of patients requiring pharmacologic intervention for elevated IOP was recorded.
At least 5 pairs of samples (serum and undiluted vitreous) were collected as close as possible to each of 7 intended time points after injection: 1 day, 3 days, 1 week, 2 weeks, 3 weeks, 4 weeks, and 8 weeks. Six additional pairs of samples from patients who did not receive a steroid injection were obtained and served as controls, yielding a total of 57 samples in all. Following collection, serum samples were immediately spun in a centrifuge at 1600 G for 10 minutes. The supernatant was then extracted and frozen at −80 C along with the collected vitreous samples. The frozen samples were later shipped overnight on dry ice to the Endocrine Medical Laboratory of the Mayo Clinic in Rochester, Minnesota. There the samples were analyzed for triamcinolone acetonide levels using liquid chromatography – tandem mass spectrometry. Briefly, the stable isotope of triamcinolone-d1 acetonide-d6 228 pmol (100 ng) was added to 50 μL of the fluid. Acetonitrile was added to each sample to precipitate proteins. The supernatants were then extracted with 4.0 mL of methylene chloride, washed, and finally dried. Fifteen microliters of the reconstituted extract was then injected onto a reversed-phase column and analyzed using a tandem mass spectrometer operating in the positive mode (API 3000 Sciex triple-quadripole mass spectrometer, ABI-Sciex, Toronto, Ontario, Canada). The minimum level of detection for this system was 0.05 ng/mL. Cortisol levels were also assessed using liquid chromatography – tandem mass spectrometry for the 31 samples sent in the final shipment to the Endocrine Medical Laboratory in Minnesota.
Preliminary statistical analyses were performed using StatView 5 for Macintosh and Windows (SAS Institute, Inc, Cary, North Carolina, USA), and final analyses were run on SPSS software version 12.0 for Windows (SPSS Inc, Chicago, Illinois, USA). Spearman correlation tests were used to assess possible relationships between serum triamcinolone concentrations, vitreous triamcinolone concentrations, serum cortisol concentrations, and vitreous cortisol concentrations. A t test was used to see if cortisol levels were significantly depressed from physiological levels.
Results
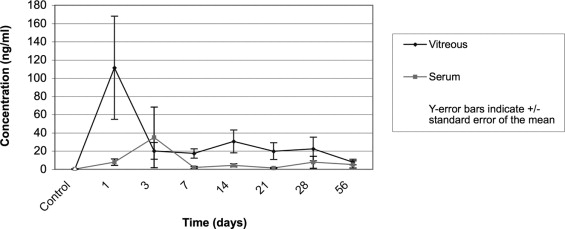
The experimental results for the serum and vitreous samples are shown in the Table . Vitreous and serum samples were collected during vitrectomies at the following time intervals: 1, 3, 7, 14, 21, 28, and 56 days after injection. The mean observed time intervals between injection and sample collection for each group were 1 ± 0 days (1-day group), 3.88 ± 0.64 days (3-day group), 6.44 ± 1.01 days (7-day group), 12.83 ± 0.98 days (14-day group), 19.29 ± 2.21 days (21-day group), 32 ± 4.38 days (28-day group), and 61 ± 3.74 days (56-day group). Vitreous concentrations of triamcinolone peaked 1 day following injection at 111.43 ± 138.93 ng/mL. Vitreous triamcinolone concentration then plateaued at around 15 to 25 ng/mL, reaching a minimum of 7.99 ± 7.0 ng/mL at 56 days. Serum concentrations reached a maximum of 35 ng/mL at day 3, with a large standard deviation of 88.21 ng/mL caused by 1 sample at 235 ng/mL. Serum concentrations plateaued around 5 ng/mL from day 3 onwards. Experimental results are plotted in Figure 2 , with the standard error of the mean highlighting the large data variability.
| Time (Days) | Vitreous Triamcinolone Acetonide (ng/mL) | Serum Triamcinolone Acetonide (ng/mL) | Vitreous Cortisol (μg/dL) | Serum Cortisol (μg/dL) |
|---|---|---|---|---|
| (Control) | 0 | 0 | 0.31 ± 0.15 | 15.54 ± 8.35 |
| n = 6 | n = 6 | n = 5 | n = 6 | |
| 1 | 111.43 ± 138.93 | 7.90 ± 8.82 | 0.20 ± 0.04 | 10.15 ± 1.94 |
| n = 6 | n = 6 | n = 3 | n = 3 | |
| 3 | 20.20 ± 27.45 | 35.00 ± 88.21 | 0.19 ± 0.22 | 8.61 ± 2.65 |
| n = 8 | n = 7 | n = 5 | n = 5 | |
| 7 | 17.38 ± 12.43 | 2.17 ± 2.51 | 0.24 ± 0.16 | 8.33 ± 4.59 |
| n = 9 | n = 7 | n = 4 | n = 5 | |
| 14 | 30.62 ± 32.98 | 4.43 ± 4.50 | 0.41 | 13.79 ± 2.02 |
| n = 6 | n = 6 | n = 1 | n = 2 | |
| 21 | 19.97 ± 24.17 | 1.48 ± 1.84 | 0.27 ± 0.26 | 11.18 ± 3.50 |
| n = 7 | n = 7 | n = 4 | n = 5 | |
| 28 | 22.42 ± 36.63 | 7.76 ± 19.83 | 0.47 ± 0.50 | 12.59 ± 4.24 |
| n = 8 | n = 9 | n = 3 | n = 3 | |
| 56 | 7.99 ± 7.01 | 5.32 ± 8.84 | 1.11 | 31.60 |
| n = 5 | n = 5 | n = 1 | n = 1 |
a There are fewer cortisol values since cortisol concentrations were only assessed in the final shipment of 31 samples.
Thirty-one sets of samples were also analyzed for their cortisol levels. Vitreous concentrations were found to dip from their initial mean of 0.31 ± 0.15 μg/dL to the 0.18 to 0.25 μg/dL range over the first week following sub-Tenon’s injection, before gradually rising over time ( Table ). Physiologic serum cortisol concentrations, indicated by preinjection controls, were recorded at 15.54 ± 8.35 μg/dL. On postinjection day 1, serum cortisol concentration was 10.15 ± 1.94 μg/dL, with concentrations dipping to 8.33 ± 4.59 μg/dL on day 7.
Serum concentrations of triamcinolone were also found to be significantly correlated with vitreous concentrations of triamcinolone (Spearman coefficient = 0.65, P < .0001). Cortisol levels in serum samples were found to decrease with an increase in systemic corticosteroid levels, with a Spearman correlation coefficient of −0.42 ( P = .02). When systemic levels of triamcinolone were highest at day 3, levels of cortisol were found to have varied significantly from their physiologic baseline as measured in the control samples ( P = .01).
Two cases were found in which patients required pharmacologic intervention for elevated IOP following both posterior sub-Tenon’s triamcinolone injection and pars plana vitrectomy. In both cases the IOP was controlled with drops alone. Although there were a few other cases with slightly elevated IOP on postoperative day 1, these were thought to be surgically induced since they resolved without medical intervention and were mild in severity.
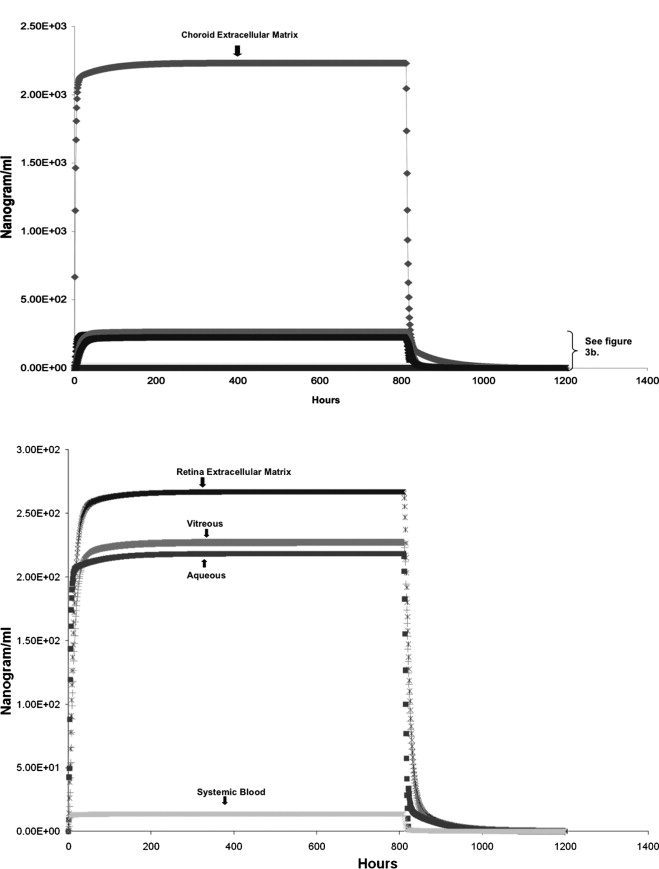
The theoretical model developed through the ocular simulation program predicted that triamcinolone levels in the serum and eye would reach their maximum level within 36 hours after posterior sub-Tenon’s injection and remain at that level for 1 month. The highest levels of triamcinolone were predicted in the choroidal extracellular matrix (ECM) with a plateau at 2230 ng/mL ( Figure 3 , Top). The vitreous levels were predicted to reach 227 ng/mL while the systemic blood levels were predicted to reach 15 ng/mL ( Figure 3 , Bottom).