CHAPTER 19 Phaco complications
Local anesthesia
Peribulbar hemorrhage
This can occur with any type of infiltrative anesthesia and is usually fairly immediate but can occasionally be delayed until later during surgery. The orbit becomes tense and incompressible but will usually soften fairly quickly over 10–20 minutes if it is due to the far more common venous bleed. The lids can become tight and difficult to open but again will usually settle down given a little time and some direct orbital pressure. An oculopressive balloon can help limit bleeding and lower the orbital tension. Occasionally the orbit will remain tense, in which case surgery should be abandoned because the risk of chamber collapse, iris prolapse, posterior capsule rupture, and vitreous loss is high. Most patients are relieved that you are putting safety first, once they have understood the risks of continuing. In practice only a small minority (around 5%) of patients with peri- or retrobulbar hemorrhage will need to have their surgery rescheduled1.
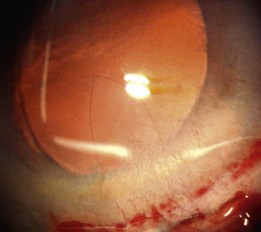
Very rarely an orbital arterial bleed may occur. This has happened to the author only once in 20 years of eye surgery. In this case there is rapid and dramatic proptosis accompanied by a rock hard orbit and infiltrative staining of skin and conjunctiva by pressurized blood (Fig. 19.1). Despite intravenous acetazolamide and mannitol plus lateral canthotomy/cantholysis the visual prognosis following arterial orbital hemorrhage is often poor.

Needle injury
Any needle can damage an extraocular muscle, perforate the globe or, if it is long enough, enter the optic nerve via the intraconal space. High risk orbital apex injections have now largely been abandoned and superceded by safer topical, peribulbar, and subTenon’s anesthesia. Consequently subarachnoid infiltration and brainstem anesthesia are almost unheard of today. The incidence of single penetration or double perforation with peribulbar anesthesia is less than 1 in 20002 but increases to around 1 in 150 with larger myopic eyes3. If a short disposable sharp 25 mm needle is used and the surgeon is familiar with the anatomy of the orbit then it is difficult to inadvertently enter a normally sized eye without adequate warning signs. First, you will meet with a significant increase in resistance to the passage of the needle as you tangentially catch the sclera. This is often associated with some pain. However the key sign is that the impaled eye rotates with advancement of the needle. If any of these three things happen then stop, withdraw, and enter more peripherally with the needle directed parallel with the orbital wall.
Incisions
A small dehiscence of Descemet’s membrane related to the internal front edge of the main wound is fairly common. This produces a hinged flap which spontaneously falls back into place and is of no consequence. A larger flap can, on most occasions, be persuaded to lie flat again. If not then an air bubble, SF6 gas, viscoelastic, or rarely suturing have all been used to successfully re-attach hanging flaps. The problem arises when a sizeable flap is stripped off and then completely detaches, never to be seen again. This is rare. The defect is usually triangular in shape with its base the width of the incision and its apex towards the center of the cornea (Fig. 19.2). Nothing to do here except wait and see how well the remaining endothelial cells respond to the greater demand on them. If over one fifth of the endothelium is gone then grafting is likely to be needed. Wait at least 3 months before considering endothelial grafting since slow recovery is the usual course with smaller defects.