Purpose
To compare the outcomes for patients with rhegmatogenous retinal detachment (RRD) and patients with retinal detachment (RD) following penetrating injury after combined 360 degree retinotomy, anterior flap retinectomy, and radial retinotomy for the management of advanced proliferative vitreoretinopathy (PVR).
Design
Retrospective, comparative, interventional case series.
Methods
Twenty-four eyes (60%) of 24 patients diagnosed with RRD and 16 eyes (40%) of 16 patients diagnosed with RD after penetrating injury whose surgery involved 360 degree retinotomy, anterior flap retinectomy, and radial retinotomy for the management of advanced PVR (grade D) were included in the analysis. The primary outcome was anatomic surgical success. Secondary outcomes were change in visual acuity (VA) and postoperative complications.
Results
The mean number of previous interventions in the RRD and trauma groups were 1.04 and 1.31, respectively ( P = .13). After 51.5 (± 52.7) months of mean follow-up, the complete retinal reattachment rates for the RRD and trauma groups were 79% (19/24) and 75% (12/16), respectively ( P > .99). The final mean VA was 2.2 logMAR (20/2000) in both groups, with improvement in the RRD group ( P = .04). The most common postoperative complications in the RRD and trauma groups, respectively, were persistent hypotony in 6 eyes (25%) and 5 eyes (31%) ( P = .73), corneal damage in 8 eyes (29%) and 6 eyes (38%) ( P = .34), and epiretinal membrane in 5 eyes (20.8%) and 4 eyes (25%) ( P > .99).
Conclusions
Only 25% of the eyes (10/40) had VA of 20/200 or better. The aim of peripheral 360 degree retinotomy, anterior flap retinectomy, and radial retinotomy is to obtain retinal reattachment, which is otherwise unachievable.
Intraretinal proliferation of all non-neuronal cell types in the retina after retinal detachment (RD) has been shown in experimental trials. Retinal pigment epithelium (RPE) and Müller cells are the principal cell types responsible for the formation of abnormal cellular accumulations in the vitreous cavity and subretinal space. Clinically, this condition is known as proliferative vitreoretinopathy (PVR). The PVR process is characterized by formation of periretinal fibrocellular membranes, intraretinal fibrosis, and subretinal bands.
Treatment of RD in eyes with PVR is challenging and requires complex vitreoretinal surgery. This may involve scleral buckling, pars plana vitrectomy (PPV) with membrane peeling, retinotomy, retinectomy, and intraocular tamponade injection. Despite extensive peeling and removal of membranes, in some cases intraoperative retinal reattachment cannot be achieved. In these cases, there seems to be some intraretinal fibrosis causing shortening of the chronically detached retina. In severe cases, relaxing retinotomy is often needed.
Since being described by Machemer in 1979, retinotomy has been used for the management of cases with severe PVR. In 1985, 360 degree retinotomy was introduced by Haut and associates. Such circumferential relaxing retinotomy is helpful in the management of anteroposterior retinal shortening in eyes with intraretinal fibrosis secondary to chronic RD. However, it has been proposed that it is not effective in the management of circumferential shortening commonly found in more advanced stages of PVR.
High anatomic success rates in patients with advanced PVR were achieved by Lim and associates, who reported performing combined circumferential retinectomy and large radial retinotomy in 2009. A PubMed search revealed no further information on the anatomic and functional outcomes since the introduction of this surgical technique.
In this retrospective study, we compared the anatomic and functional outcomes of patients diagnosed with rhegmatogenous retinal detachment (RRD) and patients with RD after penetrating injury whose surgery involved 360 degree retinotomy, anterior flap retinectomy, and radial retinotomy for the management of complex RD.
Methods
The medical records of all patients who underwent 360 degree retinotomy, anterior flap retinectomy, and radial retinotomy for complex RD at the Istanbul Retina Institute between May 1, 2000 and April 1, 2015 were reviewed. Sixty-six eyes of 63 patients were identified. Patients of all ages and grades of PVR (grade D1-3) were included. Patients with previous retinotomy, inadequate follow-up (less than 6 months), and incomplete data were excluded. Therefore, 24 eyes of 24 patients with RRD and 16 eyes of 16 patients with RD after penetrating injury were included in the analysis. Informed consent was obtained from all participants prior to every surgical procedure. The study protocol was approved by the Institutional Review Board of Sisli Memorial Hospital, Istanbul. The study was in accordance with the principles of the Declaration of Helsinki.
All patients underwent a comprehensive ophthalmologic examination including best-corrected visual acuity (BCVA), tonometry, slit-lamp biomicroscopy, and dilated funduscopic examination. Preoperative data included sex, laterality, refraction, Early Treatment Diabetic Retinopathy Study (ETDRS) visual acuity (VA), lens status, pathology, duration of symptoms, number and details of previous operations, and coexisting diseases. The PVR was graded intraoperatively using the Retina Society Classification System. Postoperative BCVA, intraocular pressure (IOP), retinal reattachment, number and details of reoperations, time of removal of silicone oil, and complications were recorded. Hypotony was defined as a persistent IOP of 5 mm Hg or less. An IOP 25 mm Hg or higher was considered elevated.
All operations were performed by the same surgeon (M.K.) and all patients from both groups had macula-off RDs. Scleral buckling (silicone tire, style 286) was performed during the same surgical procedure, prior to 360 degree retinotomy and radial retinotomy in cases presenting with significant chronic disease. Although the surgical technique varied, in all cases it included 3-port 20 gauge or 23 gauge PPV using the Associate 2500 vitrectomy system (DORC, Zuidland, Netherlands) and removal of the vitreous up to the vitreous base. Staining of posterior hyaloid with vital dyes during vitrectomy was not performed. For visualization of the residual vitreous (and the posterior hyaloid membrane in some cases), after removal of the anterior and core vitreous, 0.2–0.3 mL triamcinolone acetonide aqueous suspension (40 mg/mL) was injected into the mid vitreous cavity. Induction of PVD was attempted by active aspiration with a vitreous cutter just anterior to the peripapillary retina. In cases with a thickened posterior hyaloid membrane, if PVD could not be induced by this procedure, an end-gripping membrane forceps was used to separate the posterior hyaloid from the retinal surface. The posterior hyaloid, if any, was routinely removed in all cases.
Epiretinal membrane (ERM) peeling was done under perfluorocarbon liquid (DK-Line; Bausch and Lomb Inc, Waterford, Ireland), and retinal massage to flatten the retina was applied. After the ERM removal and retinal massage, and if the scleral buckle was considered insufficient to relieve the retinal traction, 360 degree retinotomy was created. Subretinal membrane peeling was performed and retinal massage under perfluorocarbon liquid was repeated.
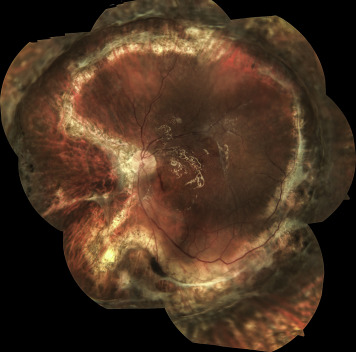
If, despite all these procedures, the intrinsic retinal rigidity did not allow retinal reattachment, radial retinotomy was performed. Radial retinotomies were localized mostly in the nasal quadrant from the circumferential retinectomy edge to 1 disc diameter from the optic disc margin ( Figure ). Retinotomy was completed usually using vertical scissors and, infrequently, a vitreous cutter. To control hemorrhage during retinotomy, blood vessels were cauterized with endodiathermy, and anterior flap retinectomy was usually completed without any bleeding. Bleeding during retinectomy was not an issue in any of the cases. If any bleeding was observed, it was easily controlled with diathermy. The retinectomy was extended circumferentially and as much as possible of the peripheral anterior retinal flap was removed to minimize ischemia and its complications. If the retina was incarcerated in a scleral wound, it was released.
Upon completion of the retinectomy, the retina was flattened with intravitreal injection of perfluorocarbon liquids. Laser photocoagulation was then applied along the posterior retinotomy and radial retinotomy edge. Perfluorocarbon was exchanged with silicone oil (1000 cs or 5000 cs). Because peripheral retinotomy extended over 360 degrees, a direct perfluorocarbon–silicone oil exchange was performed, avoiding retinal slippage in all of the cases.
A lensectomy was performed if lens opacity was limiting intraoperative visualization or if the lens was found to impede adequate dissection of the anterior PVR. Intravitreal or posterior sub-Tenon steroids were not given after surgery. Topical steroid drops were used routinely during postoperative follow-up.
The primary outcome was anatomic surgical success. Secondary outcomes were change in VA, the number of operations required for complete retinal reattachment, the number of operations undergone before retinotomy, any need for lensectomy, and the incidence of hypotony, elevated IOP, keratopathy, and other postoperative complications.
Statistical Analysis
Data were analyzed using independent-sample t tests to compare subgroups’ mean values and Pearson χ 2 test or Fisher exact test to evaluate categorical cross-distributions. Wilcoxon signed rank test was used to compare within groups and Mann-Whitney test between groups for non-normal, ordinal, or integer variables. P < .05 was considered statistically significant. Statistical analyses used SPSS version 20.0 (SPSS, Inc, Chicago, Illinois, USA).
Results
Preoperative Characteristics
Preoperative characteristics and earlier procedures are presented in Table 1 and Table 2 , respectively. For all patients, the mean age was 37.1 (± 16.3) years (range, 7–72 years). The youngest patients in the RRD and trauma groups were aged 19 and 7 years, respectively. Patients were not selected according to age.
| Characteristics | RRD (N = 24) | RD After Penetrating Injury (N = 16) | P |
|---|---|---|---|
| Age (y) | |||
| Mean (SD) | 44.2 (14.8) | 26.3 (13.0) | <.001 |
| Range | 19–72 | 7–51 | |
| Sex, n (%) | |||
| Male | 15 (63) | 12 (75) | .41 |
| Female | 9 (37) | 4 (25) | |
| VA before surgery (logMAR) | |||
| Mean (SD) | 2.46 (0.78) | 2.56 (0.73) | .67 |
| Median | 3.0 | 3.0 | |
| Range | 3.0–2.0 | 3.0–2.0 | |
| Intraocular pressure (mm Hg) | |||
| Mean (SD) | 13.4 (7.47) | 13.0 (5.51) | .85 |
| Median | 11.50 | 11.00 | |
| Range | 4–43 | 5–29 | |
| Elevated IOP, n (%) | 1 (4.2) | 0 (0) | 1.0 |
| Hypotony, n (%) | 1 (4.2) | 1 (6.3) | 1.0 |
| Number of prior operations | |||
| Mean (SD) | 1.04 (0.55) | 1.31 (0.48) | .13 |
| Median | 1.0 | 1.0 | |
| Range | 0–2 | 1–2 | |
| Lens status, n (%) | |||
| Phakic | 10 (41.6) | 6 (37.5) | .24 |
| Pseudophakic | 7 (29.2) | 1 (6.3) | |
| Aphakic | 7 (29.2) | 9 (56.2) | |
| High myopia (>6 D), n (%) | 11 (45.8) | 1 (6.3) | .01 |
| Type of Prior Procedure | RRD (N = 24) a | RD After Penetrating Injury (N = 16) a |
|---|---|---|
| No prior operations, n (%) | 3 (13) | 0 (0) |
| Scleral buckle, n (%) | 5 (20.8) | 3 (18.8) |
| Pars plana vitrectomy, n (%) | 21 (87.5) | 5 (31.3) |
| Lensectomy, n (%) | 7 (29.2) | 9 (56.3) |
| Repair of penetrating injury, n (%) | 0 (0) | 16 (100) |
Twenty-seven patients were male (68%) and 13 were female (32%). For all patients, the mean preoperative logMAR visual acuity was 2.5 (± 0.76), ranging from 3.0 to 1.0. The mean preoperative IOP for all patients was 13.2 (± 6.7) mm Hg, ranging from 4 to 43 mm Hg. Baseline characteristics did not differ between the groups, but there was a trend for the trauma group to be younger than the RRD group ( P < .001). All of the 16 eyes in the trauma group had undergone primary repair following perforating eye injury a mean 5.5 months (range 1–18 months) prior to the 360 degree retinotomy and radial retinotomy procedure. PPV and silicone oil injection in 2 eyes and PPV, scleral buckle, and silicone oil injection in 3 eyes had been performed in the trauma group following a diagnosis of RD a mean 2.2 months (range 2–4 months) prior to the procedure. In the RRD group, 17 eyes had undergone 1 PPV operation a mean 6.0 months (range 2–23 months) prior; 4 patients had had 2 PPV operations, the last performed a mean 2.3 months (range 2–4 months) earlier; and 3 patients had had symptoms for a mean of 3 months and no prior operation. Five cases from this group had had scleral buckling. Silicone oil had been used as a tamponading agent except in 4 cases, in which C3F8 gas had been used. Removal of the silicone oil was not regarded as additional surgery.
Additional Procedures Performed During Surgery
A scleral buckle was placed in 9 eyes (23%) during the 360 degree retinotomy and radial retinotomy procedure, 4 eyes (4/24; 17%) of the RRD group and 5 eyes (5/16; 31%) of the trauma group ( P = .44). Scleral buckling was performed during the same surgical procedure, prior to 360 degree retinotomy and radial retinotomy in cases presenting with significant chronic disease. Eight eyes (20%) had lens removal, 5 eyes (5/24; 21%) of the RRD group and 3 eyes (3/16; 19%) of the trauma group ( P = .34). Silicone oil endotamponade was used in all cases. In 3 patients in this case series, higher-viscosity silicone oil (5000 cs) was used to provide long-term internal tamponade and was removed after 3 months. In 2 of 3 patients the retina remained attached until the last visit, and 2 patients developed persistent hypotony. One pseudophakic eye in the RRD group and 1 in the trauma group had IOL extraction. The retina was reattached intraoperatively in all 40 eyes.
Postoperative Data
Table 3 summarizes the postoperative data for the 2 groups. The mean follow-up time for all patients was 51.5 (± 52.7) months (range, 6–152 months). Final anatomic success was achieved in 31 eyes (78%), with no significant statistical difference between groups: 19 eyes (19/24; 79%) in the RRD group and 12 eyes (12/16; 75%) in the trauma group ( P > .99). Two eyes (8%) in the RRD group and 1 eye (6%) in the trauma group developed recurrent RD underneath the silicone oil and required a second surgery with silicone oil injection. At last visit, there was a recurrent RD underneath the silicone oil in 2 of the 3 cases and 1 patient had RD after silicone oil was removed. At final follow-up there were 5 (21%) failures in the RRD group and 4 (25%) failures in the trauma group in which patients refused reoperation or reoperation was not recommended. Two patients (1 patient in each group) had recurrent RD underneath the silicone oil. In the other 7 patients, the retina redetached after the silicone oil was removed. For all patients, the mean postoperative logMAR visual acuity was 2.2 (± 0.9), ranging from 0.4 to 3.0. The improvement in VA in the RRD group was significant ( P < .04). Functional VA (≥20/200) was achieved in 6 eyes (25%) from the RRD group and 4 eyes (25%) from the trauma group ( P > .99).



