Periorbital Abscess
The most common complication of sinus infections in children is a periorbital subperiosteal abscess: a collection of pus between the bony orbital wall and periorbita. This most often occurs secondary to ethmoid sinusitis but may be caused by frontal and maxillary disease. The clinical presentation of an abscess includes pain, orbital erythema and swelling, chemosis, proptosis, gaze restriction, and visual disturbances.
23-1 Endoscopic Drainage of a Periorbital Subperiosteal Abscess
Indications
Presence of an abscess on computed tomography (CT) is an indication for surgery. Progressive or severe proptosis, gaze restriction, or decrease in visual acuity makes surgical drainage urgent. Periorbital subperiosteal abscesses that are located between the periorbita and medial orbital wall may be drained endoscopically. The endoscopic approach can provide excellent visualization of the lamina papyracea and adjacent periorbita. The advantages of this approach include avoidance of a facial scar, more rapid resolution of the periorbital inflammation, and shorter hospitalization.
Preoperative Evaluation
Children suspected of having a periorbital subperiosteal abscess should immediately be treated medically with intravenous antibiotics, nasal decongestants, steroids, and saline nasal sprays. An initial ophthalmologic consultation and, when indicated, serial assessments are essential. CT of the sinuses that identifies the involved sinuses, extent of disease, and location and size of the abscess is necessary. Only abscesses that are located between the medial orbital wall and periorbita can be drained endoscopically. Magnetic resonance imaging (MRI) should be performed if an associated intracranial complication is suspected.
Operative Technique
1. The preliminary steps for endoscopic sinus surgery are performed as described in Section 22-1, steps 1 through 6.
2. An uncinectomy and anterior ethmoidectomy are performed in a similar manner to endoscopic sinus surgery (see Section 22-1).
3. Unlike endoscopic sinus surgery for chronic sinus disease, bleeding is more likely to occur from the inflamed, infected mucosa, and visualization may be more difficult. If this occurs, oxymetazoline-soaked pledgets should be reinserted and left in place for at least 3 minutes to achieve hemostasis before proceeding with the dissection. This may have to be repeated throughout the surgery.
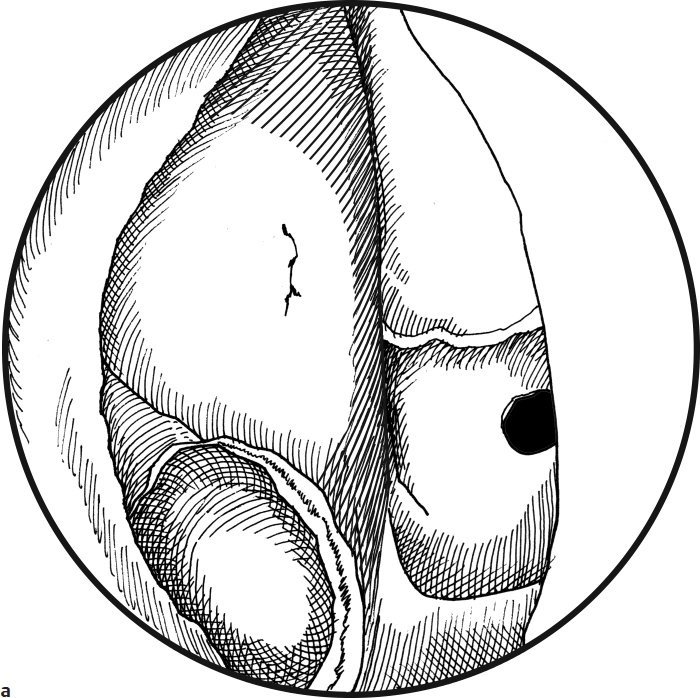
4. Using an upbiting forceps, suction, and/or microdebrider, the pus and inflammatory tissue are thoroughly removed from the anterior ethmoid cavity to expose the lateral ethmoid wall (lamina papyracea) (Fig. 23.1a).
5. While visualizing the lamina papyracea with the telescope, gentle pressure is placed on the globe. The periorbita may bulge into the ethmoid cavity through the dehiscence in the lamina papyracea, or pus may drain through the bony defect (Fig. 23.1b).
6. The dehiscence can be enlarged with a J-curette. Care must be taken to avoid violating the periorbita (Fig. 23.1c).
7. No packing or stents are placed to permit further intranasal drainage.
8. The patient remains on antibiotics, steroids, and saline nasal sprays until seen in the office in 2–3 weeks.
Advantages
1. No external scar
2. Less postoperative edema
3. More rapid resolution of signs and symptoms
4. Shorter hospital stay
Disadvantages
1. Visualization may be difficult because of smaller anatomy and bleeding
2. Need for pediatric instruments
3. Not applicable for superior, lateral, and inferior abscesses
Complications
1. Recurrence of abscess
2. Complications of endoscopic sinus surgery