Perilymph Fistula Repair
Perilymph fistula is a leak of fluid from the inner ear into the aerated middle ear. It is important to stress that this is a rare condition that typically requires great clinical suspicion to make the diagnosis; this is especially true when there is no antecedent trauma. In children, it usually occurs following severe head trauma or barotrauma. Spontaneous fistulas do occur and most often happen suddenly during physical stress.
Intermittent vertigo and fluctuating hearing loss are characteristics of perilymph fistulas, but both are not always present. Recurrent meningitis may result from a perilymph fistula that allows cerebrospinal fluid (CSF) to enter the middle ear space. The two structurally weakest points implicated in a perilymph fistula are the round window and oval window. The oval window leaks typically occur on the anterior edge of the footplate. However, congenital fissures or traumatic injuries may also be the site of the leak. What makes intraoperative identification challenging is the low volume of the perilymphatic space; these are typically very subtle leaks if they are seen intraoperatively. Topical anesthetics from canal injection will often dissect into the middle ear and confuse the picture; it is essential to be patient during this operation and observe for an active leak to confirm the diagnosis.
The diagnosis of a perilymphatic fistula is often controversial, even intraoperatively. The leaks, if present, are typically very subtle. It is not uncommon to have a negative middle ear exploration. Some surgeons in this instance advocate placing grafts over both oval and round windows; others do not, citing the risk of creating a conductive hearing loss or possibly injuring the inner ear.
7-1 Perilymph Fistula Repair
Indications
Given how controversial this operation currently is, it is wise to recommend that patients obtain a second opinion before considering surgical intervention, unless the diagnosis is imminently clear or strongly suspected.
Most fistulas respond to conservative treatment, which includes a week or more of bed rest and stool softeners with avoidance of barotrauma for several months, provided that hearing is stable or improving. Some surgeons advocate for the placement of tubes stating that they mollify external barotrauma and may allow the fistula to repair itself (but will not help avoid pressure variation from internal pressure/Valsalva maneuvers). Given that the middle ear already communicates with the nasopharynx through the eustachian tube, it is unlikely that it would result in a labyrinthitis.
Middle ear exploration and repair of perilymph fistula are indicated if a perilymph fistula is suggested as the cause of vertigo and/or hearing loss, or recurrent meningitis, especially if it has not responded to conservative treatment and there is evidence of progressive hearing loss.
Preoperative Evaluation
The preoperative evaluation of a child with suspected perilymph fistula includes an audiogram to assess for hearing loss. A fistula test, the application of positive tympanic pressure and observing for nystagmus, can be very subtle, producing little or no nystagmus; however, a frankly positive test is a solid indication to consider operative intervention. Computed tomography (CT) may demonstrate inner ear pathology, such as Mondini’s deformity, or middle ear pathology, such as dislocated incus, especially following severe trauma. A CT may demonstrate a dehiscent superior semicircular canal in an older child, which would be a relative contraindication to a middle ear exploration. However, imaging studies are rarely positive. Electronystagmography may be helpful to document the nystagmus that may accompany the perilymph fistula and can generally be done under the age of 4 in the hands of an experienced tester.
Operative Technique
1. General anesthesia and local infiltration with 1% lidocaine with 1:100,000 epinephrine are used as described for tympanoplasty. A standard postauricular incision for maximum exposure is also employed. In older children with a large external auditory canal, a transcanal approach can be used as described for middle ear exploration.
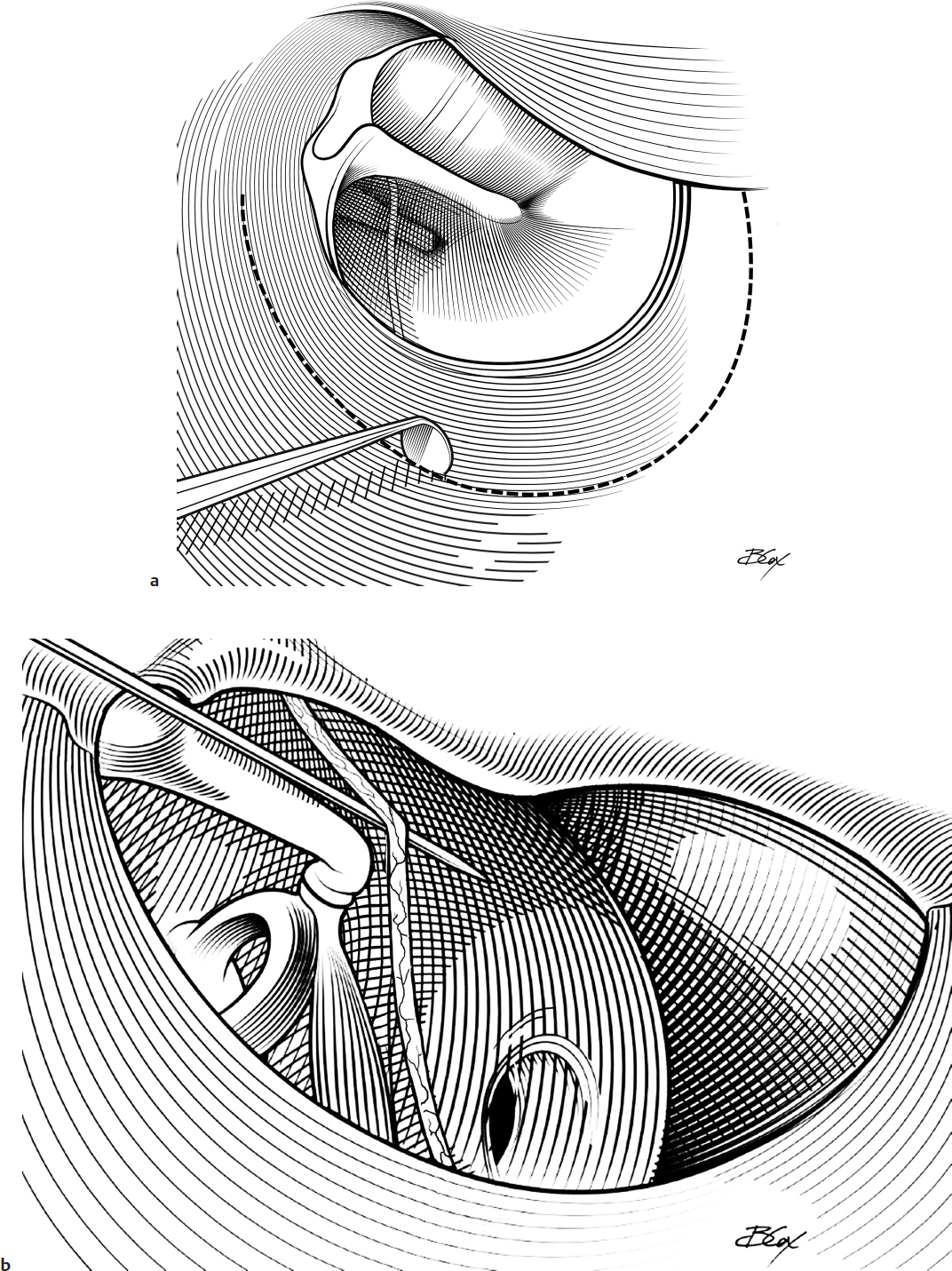
2. The middle ear space is exposed by incision and elevating the tympanomeatal flap (Fig. 7.1a).
3. Bone is removed with a curette or drill in the posterosuperior portion of the ear canal to provide visualization of the entire stapes footplate. Care is taken to avoid traumatizing the chorda tympani nerve (Fig. 7.1b,c).
4. Sufficient bone is removed to permit complete visualization of the oval and round window areas. The middle ear is examined, and the fistula, if present, is located. The region of the oval window and round window should be dried with gentle suction and watched for accumulation of fluid for up to 20 minutes (Fig. 7.1d). Having the anesthesiologist maintain a full inhalation for several seconds may increase the pressure in the subarachnoid space and increase the flow of fluid out of the fistula. If no obvious leaks are noted, the round window should be carefully assessed for a leak or the absence of a reflex while the ossicular chain is gently mobilized.
5. If the fistula is small, the mucosa surrounding the edges of the fistula of the round and/or oval window is removed with a pick and small hook (Fig. 7.1e).
6. The defect and surrounding denuded bone are covered with connective tissue (Fig. 7.1f) (e.g., fascia or perichondrium). Fascia may be obtained from the temporalis muscle, and the perichondrium is easily obtained from the tragus or conchal cartilage. The connective tissue graft can be overlaid with a small muscle graft. The grafts are then held firmly in place with Gelfoam (Pfizer) pledgets. Fibrin glue (Fig. 7.1g) can also be considered. Fat should be avoided as a graft because it is associated with a higher recurrence rate of fistulas.
7. The tympanomeatal flap is then replaced and is held in place with Gelfoam.
Typically the removal of the stapes should not be considered during the first two to three attempts to seal a perilymphatic leak as there is an increased risk of high-frequency sensorineural hearing loss with stapedectomy. However, if a large or complex defect occurs in the stapes footplate, removal of the mucosal edge of the fistula may be difficult, and covering the defect with connective tissue may not be sufficient to close the leak (Fig. 7.1h). Stapedectomy is then required. A piece of “boat-shaped” perichondrium is obtained from the tip of the tragus.
8. The suprastructure of the stapes should be removed by disarticulating the incudostapedial joint and cutting the stapedius tendon (Fig. 7.1i,j).
9. The crura should be removed with a forceps or hook exposing the remaining footplate (Fig. 7.1k).
10. The footplate fragments and mucosal adhesions are removed with a hook (Fig. 7.1l).
11. The previously obtained perichondrial “boat” graft is placed over the open oval window (Fig. 7.1m).
12. A stapes prosthesis is then positioned between the incus and the connective tissue graft overlying the oval window if the ear has auditory function (Fig. 7.1n).
13. The prosthesis is secured by securing it to the lenticular process of the incus with a crimper, alligator forceps, laser, or heat source (depending on the type of prosthesis). Several small pieces of connective tissue can then be placed around the wire to hold it in place if a wire prosthesis is selected.
14. The tympanomeatal flap is then replaced and the postauricular incision is closed as described for tympanoplasty.
Complications
1. Recurrent fistula
2. Trauma to the chorda tympani nerve
3. Facial nerve injury
4. Tympanic membrane perforation
5. Sensorineural hearing loss
6. Vertigo