Purpose
To evaluate Pentacam ectasia detection indices in topographically normal patients and in subclinical keratoconus cases.
Design
Prospective, observational case series.
Methods
setting : Institutional. patients : Group 1 comprised 1 eye from 189 patients with unremarkable topography and Groups 2 and 3 included the better and worse eyes, respectively, of 55 keratoconic patients. Group 2 eyes with normal topography (n = 37) were considered subclinical keratoconus cases. observation procedure : Pentacam Scheimpflug tomography. main outcome measures : Eleven Pentacam ectasia detection indices.
Results
All Pentacam ectasia indices significantly differed between Groups 1 and 2 and were correlated with keratoconus grade. Only 99 eyes (52%) in Group 1 had normal values for every index, whereas 7 subclinical keratoconus eyes (19%) showed 2 or fewer abnormal indices. Standardized relational thickness and overall deviation indices had 73% and 89% sensitivity for subclinical keratoconus, respectively. Both average and maximum pachymetric progression indices offered 84% sensitivity while maximum relational thickness index showed 78% sensitivity for subclinical keratoconus. Optimized cutoff values for subclinical keratoconus increased the sensitivity of the standardized and maximum relational thickness indices.
Conclusion
Pentacam Scheimpflug tomography can detect most subclinical keratoconus cases with unremarkable topography, but performance is not as good as reported and varies considerably for each index. The overall deviation, average and maximum pachymetric progression, and maximum relational thickness indices offer the highest sensitivity, which can be improved by using optimized cutoff values. Specificity constitutes an issue for some indices and up to 10% of subclinical keratoconus cases may go undetected by this technology.
Moderate and severe keratoconus cases are relatively easy to identify because of the typical clinical signs and topographic features, but its subclinical forms (topographically unremarkable corneas that later develop ectatic changes) represent a diagnostic challenge. Early keratoconus detection, especially in its subclinical form, increases the safety of corneal refractive surgery and allows for prompt treatment and prevention of ectatic disease. Placido disk–based corneal topography is commonly used for keratoconus diagnosis, but it is of little help with subclinical cases because of the lack of unequivocal findings when considered alone. Fortunately there are several complementary techniques that can aid the physician in the detection of this disorder, especially in its initial stages and in dubious cases.
Scheimpflug tomography has become a widely employed technique for anterior eye imaging, probably because it conveys a wealth of information concerning corneal thickness and back surface. As keratoconus-associated changes allegedly first arise in the posterior corneal surface, it has been proposed that corneal Scheimpflug tomography could readily detect topographically normal keratoconus cases. To this end, the Pentacam system (a widely spread Scheimpflug tomograph) provides standardized indices for ectasia detection (at least 8 indices in software version 1.19r11), but their diagnostic performance has not been thoroughly explored when dealing with truly subclinical keratoconus eyes. More importantly, these indices yield information on complementary aspects of corneal shape but their comparative effectiveness has not been addressed. There is a real need for studies that mimic the clinical setting, where a refractive surgery candidate presents with an abnormal value in only 1 or 2 of the many keratoconus detection indices and the ophthalmologist must decide without knowing the relative importance of each corneal descriptor. Some of the published studies did not analyze a strictly subclinical sample of keratoconus cases or focused on particular aspects of the Pentacam’s Belin/Ambrosio Enhanced Ectasia display. To address these issues, we set out in this study to, on the one hand, analyze Scheimpflug tomography findings in a large sample of healthy young patients with unremarkable corneal topography, and on the other hand, assess the actual diagnostic yield of each of the Pentacam’s ectasia detection indices for truly subclinical keratoconus cases.
Materials and Methods
The study was an observational case series. The research protocol followed the tenets of the Declaration of Helsinki and was approved by the Hospital de Clínicas José de San Martín ethics committee. All subjects were told of the purpose of the study and gave written informed consent before inclusion. Patients were recruited between March and November 2013 at ECOS (Clinical Ocular Studies) Laboratory and had been referred for spectacle or contact lens prescription, preoperative screening, or keratoconus diagnosis. Each subject underwent slit-lamp examination, Placido disk topography, and aberrometry (iTrace; Tracey Technologies, Houston, Texas, USA; software version 4.2.1) and Pentacam HR Scheimpflug tomography (Oculus Optikgerate GmbH, Wetzlar, Germany; software version 1.19r11). All measurements were performed by experienced operators (P.R.V., J.D.G., and M.D.) in a darkened room within a 15-minute period, and the subjects were told to blink immediately before each examination. Only good-quality examinations were accepted, defined as automated captures for the iTrace device in which all the reflected Placido rings were free of artifacts, and as automatic Scheimpflug scans (25 images in 2 seconds) that passed the Pentacam software’s quality check. For topography and keratoconus grading, the Keratoconus Severity Score was used, which is based on average corneal power and corneal higher-order aberrations (expressed in μm as root mean square values). The Keratoconus Severity Score scale ranges from 0 to 5, as follows: 0: unaffected, normal topography; 1: unaffected, atypical topography; 2: suspect; 3: mild keratoconus; 4: moderate keratoconus; and 5: severe keratoconus. Participant exclusion criteria were the following: previous eye surgery, any eye disease other than keratoconus, chronic use of topical medications, or corneal opacities. Patients were asked to cease contact lens wear at least 3 weeks before examination.
Three independent groups were recruited for this study. Patients with unremarkable slit-lamp examination and normal topography (Keratoconus Severity Score 0: typical axial topography pattern, average corneal power ≤47.75 diopters, and higher-order aberrations <0.65 μm) in both eyes were recruited in Group 1 (only 1 eye was randomly selected). Such strict topographic criteria were established to restrict the sample to patients without suspicious clinical and topographic findings and were adapted from Buhren and associates. Patients with biomicroscopy and topographic findings of manifest keratoconus (Keratoconus Severity Score 3 or greater: axial topography pattern consistent with keratoconus, may have positive slit-lamp findings, no corneal scarring, average corneal power >49.00 diopters, and higher-order aberrations >1.50 μm) in at least 1 eye were considered keratoconic, and corneal curvature was used as a surrogate indicator of ectasia grade : the eye with the lowest average corneal power was included in Group 2 (better or less advanced keratoconic eyes) while the eye with the highest average corneal power was included in Group 3 (worse or more advanced keratoconic eyes). No patient had exactly the same average corneal power in both eyes. Eyes in Group 2 with insufficient topographic findings to meet diagnostic criteria for keratoconus (Keratoconus Severity Score 0–2) were considered subclinical cases and analyzed further as Subgroup 2SC.
The following corneal descriptors were obtained from the Pentacam software Belin-Ambrósio Enhanced Ectasia Display: central and thinnest pachymetry; front and back corneal elevation at the thinnest corneal point; pachymetric progression indices (minimum, average, and maximum); normalized indices Df (deviation of normality of the front elevation), Db (deviation of normality of the back elevation), Dp (deviation of normality of pachymetric progression), Dt (deviation of normality of corneal thinnest point), Da (deviation of normality of relational thickness), and D (overall deviation of normality); and Ambrosio’s average and maximum relational thickness indices. The methodology for calculation has been disclosed by the manufacturer for some but not all of these indices. Pachymetric progression refers to the percentage in corneal thickness increase along each meridian starting from the thinnest corneal point, and the minimum, average, and maximum values are reported, whereas relational thickness indices (average and maximum) express the ratio of the thinnest pachymetry and the respective pachymetric progression. Upon request, the manufacturer informed that the deviation indices, average pachymetric progression, and maximum relational thickness are classified by the software as normal (<1.6 standard deviation [SD] from the population mean, shown in white), suspicious (≥1.6 SD and <2.6 SD, highlighted in yellow), and pathologic (≥2.6 SD, highlighted in red), from the data reported by Ambrosio and associates, and this scheme was followed throughout this work. For the normalized indices, each observation was classified into 1 of the 3 categories, whereas for the pachymetric progression and relational thickness indices, each observation was categorized as normal or abnormal according to the cutoff values reported by Ambrosio and associates : minimum pachymetric progression ≥0.79, average pachymetric progression ≥1.06, maximum pachymetric progression ≥1.44, average relational thickness ≤424, and maximum relational thickness ≤339 were considered abnormal.
Normality of the data was assessed by the Kolmogorov-Smirnov test, and parametric or nonparametric tests were subsequently used. Receiver operating characteristic (ROC) curves were used to calculate sensitivity, specificity, and area under the curve of each corneal index, as previously described. Optimal cutoff points for each index were obtained from the ROC curves as those closest to the perfect classification point. Logistic regression with forward stepwise inclusion (logistic function 1: logit = 0.467 × Db + 2.625 × Da − 4.871) and all variables entered at once (logistic function 2: logit = 0.333 × Df + 0.353 × Db − 0.466 × Dp + 0.077 × Dt + 3.149 × Da − 5.257) was employed to combine the 5 individual D indices, with a 0.5 cutoff. Statistical tests and analysis were performed with Prism 5 software (GraphPad Software, La Jolla, California, USA) and SPSS 17 software (SPSS Inc, Chicago, Illinois, USA). Statistical significance was set at P < .05 and data are shown as mean ± standard deviation unless otherwise stated. Data collection and sorting were done with the aid of Microsoft Excel 2010 software.
Results
Demographics and Keratoconus Grade Distribution
Group 1 (control eyes) comprised 189 eyes (94 right and 95 left) from 189 patients with unremarkable topography (Keratoconus Severity Score 0) in both eyes. The less advanced eye (29 right and 26 left) of 55 keratoconus patients was included in Group 2, whereas the worse eye (26 right and 29 left) was included in Group 3. There was no significant difference in mean age between control (32.3 ± 8.1 years, range 14–71) and keratoconic (32.5 ± 11.7 years, range 14–65) patients, but sex distribution significantly differed (41% vs 60% male, P = .01) between groups. According to Keratoconus Severity Score grading, Group 2 included 21 grade 0 eyes (38%), 7 grade 1 eyes (13%), 9 grade 2 eyes (16%), 15 grade 3 eyes (27%), 1 grade 4 eye (2%), and 2 grade 5 eyes (4%), whereas Group 3 comprised 33 grade 3 eyes (60%), 11 grade 4 eyes (20%), and 11 grade 5 eyes (20%).
Corneal Descriptors in Control and Keratoconic Eyes
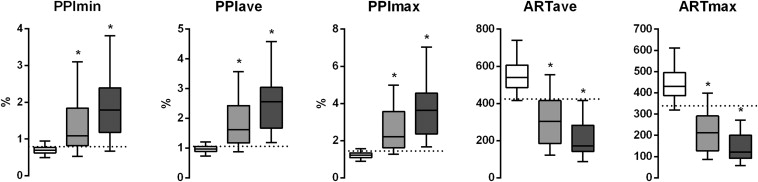
Conventional corneal descriptors are summarized in Table 1 and depicted in Figure 1 . Means for every Pentacam corneal descriptor in Groups 2 and 3 were significantly different when compared with Group 1 ( Table 1 , Figures 2 and 3 ). In Group 2 eyes, every keratoconus index was significantly correlated with Keratoconus Severity Score grading (Spearman correlation, Table 1 for r values, P < .001). Truly subclinical keratoconus eyes (n = 37 [67%], Group 2 eyes with Keratoconus Severity Score 0–2) were analyzed further as Subgroup 2SC ( Table 1 ), and they also differed significantly in means with Group 1 eyes for every Pentacam corneal descriptor analyzed.
| Control Patients Group 1 (n = 189) | Keratoconus Patients (n = 55) | |||
|---|---|---|---|---|
| Subclinical Keratoconus Eyes Group 2SC (n = 37) | Better Keratoconus Eyes Group 2 (n = 55) | Worse Keratoconus Eyes Group 3 (n = 55) | ||
| Conventional corneal descriptors | ||||
| ACP (D) | 44.48 ± 1.48 (40.83–47.48) | 44.71 ± 2.19 (40.76–48.90) | 46.03 ± 3.50 a (40.76–56.56) | 51.53 ± 7.48 a (42.23–77.24) |
| HOA (μm) | 0.251 ± 0.070 (0.145–0.497) | 0.669 ± 0.350 a (0.183–1.472) | 1.153 ± 0.947 a (0.183–5.596) | 3.261 ± 5.918 a (0.373–36.840) |
| CCT (μm) | 532 ± 33 (449–628) | 502 ± 37 a (412–587) | 491 ± 39 a (407–587), r = 0.364 | 479 ± 76 a (321–940) |
| TP (μm) | 528 ± 32 (448–625) | 489 ± 37 a (409–572) | 474 ± 43 a (376–572), r = 0.474 | 443 ± 45 a (298–550), r = 0.415 |
| Front elevation at thinnest location | 3 ± 2 (−3–14) | 10 ± 8 a (−3–36) | 16 ± 12 a (−3–43), r = 0.779 | 26 ± 15 a (−11–72), r = 0.676 |
| Back elevation at thinnest location | 4 ± 5 (−7–37) | 24 ± 21 a (0–85) | 36 ± 27 a (0–90), r = 0.757 | 54 ± 26 a (−1–130), r = 0.667 |
| Pentacam’s keratoconus indices | ||||
| PPImin | 0.70 ± 0.13 (0.37–1.16) | 1.02 ± 0.41 a (0.46–2.25) | 1.34 ± 0.70 a (0.46–3.48), r = 0.722 | 1.90 ± 0.86 a (0.59–4.28), r = 0.695 |
| PPIave | 0.97 ± 0.14 (0.61–1.44) | 1.42 ± 0.48 a (0.75–2.97) | 1.79 ± 0.77 a (0.75–3.67), r = 0.773 | 2.53 ± 0.99 a (1.03–5.61), r = 0.741 |
| PPImax | 1.22 ± 0.20 (0.73–2.02) | 2.06 ± 0.81 a (0.90–4.90), r = 0.464 | 2.61 ± 1.17 a (0.90–5.35), r = 0.743 | 3.70 ± 1.53 a (1.41–8.35), r = 0.670 |
| Df | 0.44 ± 1.07 (−1.79–4.13) | 2.71 ± 2.48 a (−1.19–8.67) | 5.43 ± 5.18 a (−1.19–21.97), r = 0.850 | 11.68 ± 8.25 a (−1.86–35.29), r = 0.821 |
| Db | −0.21 ± 0.90 (−1.49–4.05) | 2.00 ± 2.31 a (−1.30–7.58) | 4.15 ± 4.44 a (−1.30–23.22), r = 0.808 | 9.63 ± 6.98 a (−1.03–29.83), r = 0.854 |
| Dp | 0.44 ± 0.92 (−1.99–3.63) | 3.49 ± 3.24 a (−1.05–13.94) | 5.97 ± 5.09 a (−1.05–18.15), r = 0.772 | 11.01 ± 6.62 a (0.84–31.85), r = 0.736 |
| Dt | 0.33 ± 0.96 (−2.16–3.09) | 1.64 ± 1.31 a (−0.91–4.84) | 2.31 ± 1.85 a (−0.91–9.28), r = 0.479 | 3.50 ± 2.06 a (−0.35–12.46), r = 0.419 |
| Da | 0.39 ± 0.79 (−2.62–2.29) | 2.08 ± 0.94 a (−1.20–3.74) | 2.48 ± 1.00 a (−1.20–3.99), r = 0.664 | 3.21 ± 0.96 a (1.00–8.28), r = 0.636 |
| D | 1.03 ± 0.70 (−0.87–4.86) | 4.26 ± 3.03 a (0.55–16.55) | 6.08 ± 3.98 a (0.55–16.55), r = 0.757 | 9.81 ± 4.70 a (1.42–22.92), r = 0.833 |
| ARTave (μm) | 555 ± 98 (333–893) | 381 ± 125 a (160–744) | 318 ± 142 a (112–744), r = −0.757 | 208 ± 99 a (53–518), r = −0.704 |
| ARTmax (μm) | 445 ± 87 (237–770) | 269 ± 101 a (97–620) | 223 ± 109 a (78–620), r = −0.729 | 145 ± 73 a (42–379), r = −0.662 |


Classification of Control Eyes According to Their Pentacam Corneal Indices
The classification results according to each keratoconus detection index are summarized in Table 2 and Figure 4 . In Group 1, 129 eyes (68.3%) had normal values for every D index; of these, all but 3 (126 eyes, 66.7%) also showed normal values for maximum relational thickness and all but 21 (108 eyes, 57.1%) also exhibited normal average pachymetric progression values. When considering every deviation index and maximum relational thickness and average pachymetric progression altogether, 107 eyes (56.6%) showed normal values for every index. Regarding the pachymetric progression indices, only 128 eyes (67.7%) exhibited normal values in all of them, whereas for average and maximum relational thickness, 169 eyes (89.4%) had normal values in both indices. Only 99 eyes (52.4%) in Group 1 did not show abnormal scores in each of the 11 indices reported by the Pentacam. Group 1 eyes with normal overall deviation values (n = 152, 80.4%) did not significantly differ in higher-order aberrations compared with those with suspicious or abnormal values (0.250 ± 0.072 vs 0.256 ± 0.060 μm, P = .66). Group 1 eyes with normal pachymetric progression deviation values (n = 173, 91.5%) also did not differ in higher-order aberrations when compared with those Group 1 eyes flagged as suspicious or abnormal (≥1.6 SD) according to this metric.
| Control Eyes Group 1 (n = 189) | Subclinical Keratoconus Eyes Subgroup 2SC (n = 37) | Better Keratoconus Eyes Group 2 (n = 55) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Normal (<1.6 SD) | Suspect (≥1.6 SD) | Abnormal (≥2.6 SD) | Normal (<1.6 SD) | Suspect (≥1.6 SD) | Abnormal (≥2.6 SD) | Normal (<1.6 SD) | Suspect (≥1.6 SD) | Abnormal (≥2.6 SD) | |
| Df | 162 (85.7%) | 23 (12.2%) | 4 (2.1%) | 16 (43.2%) | 6 (16.2%) | 15 (40.5%) | 16 (29.1%) | 6 (10.9%) | 33 (60.0%) |
| Db | 182 (96.3%) | 4 (2.1%) | 3 (1.6%) | 17 (45.9%) | 4 (10.8%) | 16 (43.2%) | 17 (30.9%) | 4 (7.3%) | 34 (61.8%) |
| Dp | 173 (91.5%) | 14 (7.4%) | 2 (1.1%) | 12 (32.4%) | 6 (16.2%) | 19 (51.4%) | 12 (21.8%) | 6 (10.9%) | 37 (67.3%) |
| Dt | 172 (91.0%) | 15 (7.9%) | 2 (1.1%) | 21 (56.8%) | 9 (24.3%) | 7 (18.9%) | 23 (41.8%) | 11 (20.0%) | 21 (38.2%) |
| Da | 183 (96.8%) | 6 (3.2%) | 0 (0%) | 10 (27.0%) | 16 (43.2%) | 11 (29.7%) | 10 (18.2%) | 17 (30.9%) | 28 (50.9%) |
| D | 152 (80.4%) | 34 (18.0%) | 3 (1.6%) | 4 (10.8%) | 7 (18.9%) | 26 (70.3%) | 4 (7.3%) | 7 (12.7%) | 44 (80.0%) |
| Normal | Abnormal | Normal | Abnormal | Normal | Abnormal | ||||
| PPImin | 151 (79.9%) | 38 (20.1%) | 13 (35.1%) | 24 (64.9%) | 13 (23.6%) | 42 (76.4%) | |||
| PPIave | 142 (75.1%) | 47 (24.9%) | 6 (16.2%) | 31 (83.8%) | 6 (10.9%) | 49 (89.1%) | |||
| PPImax | 168 (88.9%) | 21 (11.1%) | 6 (16.2%) | 31 (83.8%) | 6 (10.9%) | 49 (89.1%) | |||
| ARTave | 177 (93.7%) | 12 (6.3%) | 11 (29.7%) | 26 (70.3%) | 11 (20.0%) | 44 (80.0%) | |||
| ARTmax | 173 (91.5%) | 16 (8.5%) | 8 (21.6%) | 29 (78.4%) | 8 (14.5%) | 47 (85.5%) | |||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


