Purpose
To evaluate the long-term risk of endothelial rejection, graft survival, and associated factors following penetrating keratoplasty (PK) for keratoconus, with and without prior resolved corneal hydrops.
Design
Retrospective cohort study.
Methods
Primary outcome measures were endothelial rejection–free survival and failure-free survival. Secondary outcome measures were corneal neovascularization following hydrops and complications following PK.
Results
A total of 245 eyes underwent PK for keratoconus with mean follow-up of 5.6 ± 3.6 years. Eyes with prior hydrops (n = 74) had lower endothelial rejection–free survival rates compared with eyes without prior hydrops: 86.5% ± 4.0% vs 86.5% ± 2.6% at 1 year, 61.0% ± 6.2% vs 76.9% ± 3.3% at 5 years, and 45.8% ± 10.1% vs 70.9% ± 4.3% at 10 years, respectively ( P = .023). Multivariate analysis identified factors associated with endothelial rejection as age ≤25 years ( P = .017), corneal neovascularization ( P = .001), donor trephination size >8 mm ( P = .017), and poor clinic attendance ( P = .015). There was no difference in the failure-free survival rates with and without prior hydrops: 98.6% ± 1.3% vs 97.1% ± 1.3% at 1 year, 97.3% ± 1.9% vs 95.1% ± 1.9% at 5 years, and 97.3% ± 1.9% vs 92.2% ± 2.7% at 10 years, respectively ( P = .42). Corneal neovascularization was present at the time of PK in 44.6% of eyes with prior hydrops and 7.6% without prior hydrops ( P < .001).
Conclusions
Corneal neovascularization, a frequent complication of corneal hydrops, was associated with increased risk of endothelial rejection following PK. However, allograft survival was similar in eyes with and without prior hydrops.
Acute corneal hydrops is the development of marked corneal edema owing to a break in the Descemet membrane what allows aqueous humor to enter the corneal stroma and epithelium. Corneal hydrops is frequently seen in eyes with keratoconus and has been reported to occur in approximately 3% of patients with this condition, but also occurs in other ectatic conditions such as pellucid marginal degeneration and keratoglobus. The natural course of hydrops typically involves the spontaneous resolution of corneal edema over 2–4 months. Upon resolution of the edema, patients may have minimal to severe vision loss depending on the degree of residual scarring.
Following resolution of hydrops, up to 60% of eyes may require keratoplasty for visual rehabilitation. Although penetrating keratoplasty (PK) performed for keratoconus carries a favorable overall prognosis, endothelial graft rejection may result in graft failure. Numerous studies have reported the long-term outcomes of PK for keratoconus and factors associated with increased risk of rejection and/or failure. However, only a few studies have specifically assessed the outcomes of PK for eyes with prior resolved hydrops, with conflicting results. A study by Tuft and associates found a higher risk of endothelial rejection following PK in 87 eyes with prior resolved hydrops, although other associated and potentially confounding factors were not evaluated. Basu and associates also found a higher rate of endothelial rejection in their study of 32 eyes with prior hydrops and subanalysis identified longer duration of corneal hydrops (>3 months) and ocular allergies as significant factors. However, Akova and associates did not find an increased rate of endothelial rejection in 35 eyes with prior hydrops.
The current study assessed the long-term outcomes of penetrating keratoplasty for keratoconus in a large series of eyes with and without prior resolved corneal hydrops to evaluate the long-term risk of endothelial rejection, graft survival, and associated factors.
Methods
We conducted a retrospective cohort study of all patients who underwent PK for keratoconus between January 2000 and June 2013 in the Ophthalmology Department, Greenlane Clinical Centre, Auckland, which is the major tertiary center for corneal transplantation in New Zealand. The study was approved by the University of Auckland Ethics Committee (#013907) and followed the tenets of the Declaration of Helsinki.
Exclusion criteria included post-PK follow-up of less than 2 years, repeat PK, prior hydrops of unknown duration or treatment, hydrops complicated by microbial keratitis, PK performed for nonoptical reasons, and PK performed before clinical resolution of hydrops.
Data Collection
The medical records of all eligible patients were reviewed by 1 experienced clinical investigator (J.M.). Acute corneal hydrops was defined clinically as the onset of corneal edema in eyes with keratoconus with or without an identifiable break in Descemet membrane and without signs of an alternative diagnosis. The duration of hydrops was calculated as the date of onset of symptoms to the date of complete disappearance of corneal edema by slit-lamp examination.
Atopy (nonocular) was defined as a history of asthma, atopic dermatitis/eczema, or allergic rhinitis and was self-reported by the patient and/or was identified by review of patients’ nonophthalmologic electronic medical record or electronic pharmacy records for medications used to treat these conditions. Ocular allergy was diagnosed based on a history of symptoms of ocular itching and ocular findings of a papillary reaction or hyperemia of the conjunctiva, or if topical medications for allergic conjunctivitis were prescribed.
The treatments of episodes of hydrops were recorded, including type, frequency, and duration of topical corticosteroid, if prescribed. All episodes of acute corneal hydrops were treated with topical medications at the discretion of the clinician.
All PK procedures were performed using standard techniques under general anesthesia. Donor corneas were stored at 34 C in New Zealand Eye Bank organ culture medium. The donor corneal button was typically oversized by 0.25 mm and sutured using 10-0 nylon in an interrupted, continuous, or combined interrupted and continuous fashion. Patients were examined 1 day, 1 week, 1 month, and 3 months postoperatively, and then scheduled for examinations approximately every 3 months. All patients received a topical antibiotic (chloramphenicol 0.5% or ciprofloxacin 0.3%) 3–4 times daily and corticosteroid (prednisolone acetate 1%) every 1–2 hours for the first week. Thereafter, the corticosteroid was typically reduced to 4 times daily and tapered by 1 drop every 3 months to 1 drop daily and was continued until suture removal. Loose or broken sutures were removed upon presentation. Intact sutures were routinely removed in one sitting in the operating theatre at 18–24 months post-PK using aseptic technique, followed by topical antibiotic coverage for 2 weeks and topical corticosteroid with g. prednisolone acetate 1% 4 times a day for 1 month and discontinued thereafter if no previous rejection or significant risk factors for rejection.
Corneal neovascularization was recorded by the surgeon at the time of PK and was reported to the New Zealand National Eye Bank on a standardized pro forma, as is required for each transplant procedure. Corneal neovascularization was recorded as the number of quadrants of neovascularization present and the number of quadrants of neovascularization crossing the trephination.
Endothelial rejection was defined clinically as the acute onset of anterior uveitis with overlying graft edema. Endothelial rejection episodes were all initially treated with topical corticosteroids (prednisolone acetate 1%) every hour. Patients treated with intravenous (IV) methylprednisolone received 500–1000 mg daily for 1–3 days. Graft failure was defined clinically as the loss of transparency for at least 3 months with associated decline in vision.
Compliance with clinic appointments was calculated as the number of appointments attended divided by the number of appointments scheduled, during the first 2 years following PK.
Analysis
The primary outcome measures were (1) endothelial rejection–free allograft survival and (2) failure-free allograft survival. The rejection-free survival time was calculated as the date of the PK to the date of the first episode of endothelial rejection. Secondary analyses were degree of corneal neovascularization in eyes with prior hydrops and complications in all eyes following PK.
All statistical analyses were performed using SPSS 19.0 for Windows (SPSS; IBM, Chicago, Illinois, USA). Preoperative features were compared using the χ 2 test. Primary analyses involved Kaplan-Meier survival analysis to estimate the cumulative probability (reported as percentage with standard error) of endothelial rejection–free allograft survival and failure-free allograft survival; univariate analysis of potential risk factors for endothelial rejection, performed using the log-rank test; and multivariate analysis of factors with significant univariate associations, performed using a Cox proportional hazards model to estimate the relative effect of variables on allograft survival.
Secondary analyses were focused on potential risk factors for endothelial rejection specific to eyes with prior hydrops only, and on risk factors for the development of corneal neovascularization prior to undergoing PK. Univariate associations were determined using the χ 2 test, log-rank test, and independent samples t test. A P value of less than .05 was considered statistically significant.
Results
Of the 410 eyes that underwent PK for keratoconus in the study period, 245 were included in the study (74 with prior hydrops, 171 without prior hydrops), with a mean follow-up of 5.6 ± 3.6 years. Excluded eyes were as follows: 96 (23.4%) repeat PK, 23 eyes (5.6%) that showed evidence of prior hydrops but had not been seen in the service acutely, 34 eyes (8.3%) with inadequate (<2 years) post-PK follow-up, 9 eyes that underwent nonoptical PK, 2 eyes with PK prior to complete resolution of hydrops, and 1 eye with microbial keratitis at the time of hydrops.
The mean age of the patients at the time of PK was 29.6 ± 9.9 years (26.6 ± 7.0 years with prior hydrops, 30.9 ± 10.6 years without hydrops; P = .002). In the 74 eyes with hydrops, the mean age of patients at the onset of acute hydrops was 24.8 ± 7.1 years. The mean duration of corneal hydrops was 3.2 ± 2.6 months, and the duration between resolution of hydrops and PK was 17.3 ± 24.9 months. The cohort of eyes with prior hydrops had a higher percentage of patients with age <25 years at the time of PK, greater frequency of ocular allergy, greater degree of corneal neovascularization (both overall and crossing the trephination), and a higher percentage of donor button size >8 mm ( Table 1 ).
| Characteristics | Total, n (%) | Hydrops, n (%) | No Hydrops, n (%) | P Value |
|---|---|---|---|---|
| Sex | ||||
| Male | 138 (56.3) | 39 (52.7) | 99 (57.9) | .270 |
| Female | 107 (43.7) | 35 (47.3) | 72 (42.1) | |
| Age at PK (y) | ||||
| ≤25 | 91 (37.1) | 34 (45.9) | 57 (33.3) | .042* |
| >25 | 154 (62.9) | 40 (54.1) | 114 (66.7) | |
| Laterality of operated eye | ||||
| Right | 112 (45.7) | 37 (50) | 75 (43.9) | .228 |
| Left | 133 (54.3) | 37 (50) | 96 (56.1) | |
| Ocular allergy | ||||
| Present | 44 (18.0) | 25 (33.8) | 19 (11.1) | <.001* |
| Absent | 201 (82.0) | 49 (66.2) | 152 (88.9) | |
| Atopy | ||||
| Yes | 159 (64.9) | 51 (68.9) | 108 (63.2) | .236 |
| No | 86 (35.1) | 23 (31.1) | 63 (36.8) | |
| Corneal neovascularization | ||||
| Present | 46 (18.8) | 33 (44.6) | 13 (7.6) | |
| Absent | 199 (81.2) | 41 (55.4) | 158 (92.4) | <.001* |
| Vessels crossing trephination | ||||
| Yes | 39 (15.9) | 29 (39.2) | 10 (5.8) | <.001* |
| No | 7 (2.9) | 4 (5.4) | 3 (1.8) | |
| Absent | 199 (81.2) | 41 (55.4) | 158 (92.4) | |
| Donor trephine size (mm) | ||||
| ≤8 | 117 (47.8) | 23 (31.1) | 94 (55.0) | <.001* |
| >8 | 128 (52.2) | 51 (68.9) | 77 (45.0) | |
| Recipient trephine size (mm) | ||||
| ≤8 | 229 (93.5) | 67 (90.5) | 162 (94.7) | .173 |
| >8 | 16 (6.5) | 7 (9.5) | 9 (5.3) | |
| Donor ECD (cells/mm 2 ) | ||||
| ≤3000 | 87 (35.5) | 24 (32.4) | 63 (36.8) | .304 |
| >3000 | 158 (64.5) | 50 (67.6) | 108 (63.2) | |
| Appointments attended a | ||||
| ≤80% | 94 (38.4) | 26 (35.1) | 68 (39.8) | |
| >80% | 151 (61.6) | 48 (64.9) | 103 (60.2) | .295 |
| Suture complication b | ||||
| Yes | 69 | 17 (23.0) | 52 (30.4) | |
| No | 176 | 57 (77.0) | 119 (69.6) | .151 |
a Percentage attended during first 2 years following PK.
b Postoperative loose and/or broken suture(s) and/or suture infiltrate(s).
Outcomes of Primary Analyses
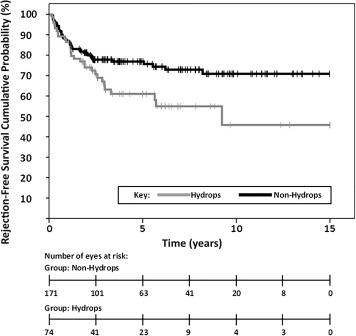
The overall rejection-free survival rates were 86.5% ± 2.2% at 1 year, 72.1% ± 3.0% at 5 years, and 64.1% ± 4.0% at 10 years. An endothelial rejection episode occurred in 29 of the 74 eyes (39.2%) with prior hydrops and 42 of 171 eyes (24.5%) without prior hydrops ( P = .031). There was a significant difference ( P = .023) in the endothelial rejection–free allograft survival rates for the eyes with and without prior hydrops: 86.5% ± 4.0% vs 86.5% ± 2.6% at 1 year, 61.0% ± 6.2% vs 76.9% ± 3.3% at 5 years, and 45.8% ± 10.1% vs 70.9 ± 4.3% at 10 years, respectively ( Figure 1 ).
On univariate analysis, significant associations with decreased 5-year endothelial rejection–free survival were as follows: female sex, age ≤25 years, previous episode of hydrops, presence of corneal neovascularization, corneal neovascularization crossing trephination, donor trephine size >8 mm, and attendance of ≤80% of clinic appointments in the first 2 years following PK ( Table 2 ). Female subjects had lower mean compliance with clinic appointments (78.3% ± 23.3%) compared to male subjects (82.98% ± 18.37%), though this difference was not significant ( P = .086).
| Factor | Total | Rejection | Endothelial Rejection–Free Survival at 5 Years ± SE (%) | P Value |
|---|---|---|---|---|
| Gender | ||||
| Male | 138 | 33 | 75.3 ± 3.9 | .043* |
| Female | 107 | 38 | 67.9 ± 4.7 | |
| Age at PKP (y) | ||||
| ≤25 | 91 | 34 | 65.5 ± 5.0 | .013* |
| >25 | 154 | 37 | 76.1 ± 3.7 | |
| Laterality of operated eye | ||||
| Right | 112 | 27 | 76.0 ± 4.3 | .201 |
| Left | 133 | 44 | 69.0 ± 4.2 | |
| Ocular allergy | ||||
| Present | 44 | 14 | 71.7 ± 3.4 | .812 |
| Absent | 201 | 57 | 74.0 ± 6.8 | |
| Atopy | ||||
| Present | 159 | 53 | 68.7 ± 3.8 | .061 |
| Absent | 86 | 18 | 78.3 ± 5.0 | |
| Prior episode of hydrops | ||||
| Present | 74 | 29 | 61.0 ± 6.2 | .023* |
| Absent | 171 | 42 | 76.9 ± 3.3 | |
| Duration of hydrops (mo) | ||||
| No hydrops | 171 | 42 | 76.9 ± 3.3 | .038* |
| ≤3 | 47 | 17 | 63.7 ± 7.7 | |
| >3 | 27 | 12 | 58.8 ± 9.6 | |
| Corneal neovascularization | ||||
| Present | 46 | 46 | 45.8 ± 8.0 | <.001* |
| Absent | 199 | 25 | 78.2 ± 3.1 | |
| Vessels crossing trephination | ||||
| Yes | 39 | 22 | 43.8 ± 8.9 | <0.001* |
| No | 7 | 3 | 53.6 ± 20.1 | |
| Absent | 199 | 46 | 78.2 ± 3.1 | |
| Donor trephine size (mm) | ||||
| ≤8 | 117 | 26 | 81.6 ± 3.8 | .007* |
| >8 | 128 | 45 | 63.6 ± 4.5 | |
| Recipient trephine size (mm) | ||||
| ≤8 | 229 | 65 | 72.8 ± 3.1 | .470 |
| >8 | 16 | 6 | 62.5 ± 12.1 | |
| Donor ECD (cells/mm 2 ) | ||||
| ≤3000 | 87 | 29 | 67.0 ± 5.3 | .212 |
| >3000 | 158 | 42 | 75.0 ± 3.6 | |
| Appointments attended a | ||||
| ≤80% | 94 | 36 | 64.6 ± 5.1 | .010* |
| >80% | 151 | 35 | 76.9 ± 3.7 | |
| Suture complication b | ||||
| Present | 69 | 23 | 68.6 ± 5.7 | .415 |
| Absent | 176 | 48 | 73.5 ± 3.5 | |
a Percentage attended during first 2 years following PK.
b Postoperative loose and/or broken suture(s) and/or suture infiltrate(s).
Multivariate analysis showed a significantly higher risk of endothelial rejection at 5 years in eyes of patients ≤25 years of age at PK (hazard ratio 1.82; 95% confidence interval 1.11–2.98; P = .017), presence of corneal neovascularization (hazard ratio 2.99; 95% confidence interval 1.58–5.66; P = .001), donor trephination size >8 mm (hazard ratio 1.86; 95% confidence interval 1.12–3.08; P = .017), and attendance of ≤80% of clinic appointments in the first 2 years following PK (hazard ratio 1.80; 95% confidence interval 1.12–2.89; P = .015).
All keratoplasties that failed had at least 1 prior episode of endothelial rejection in the study period. Graft failure occurred in 2 of 74 eyes (2.7%) with prior hydrops and 9 of 171 eyes (5.3%) without prior hydrops during the study period. There was no difference ( P = .42) in the failure-free survival rates of eyes with and without prior hydrops: 98.6% ± 1.3% vs 97.1% ± 1.3% at 1 year, 97.3% ± 1.9% vs 95.1% ± 1.9% at 5 years, and 97.3% ± 1.9% vs 92.2% ± 2.7% at 10 years, respectively ( Figure 2 ). Univariate analysis did not identify any factors associated with graft failure.



