Penetrating keratoplasty (PK) is the surgical removal of diseased cornea with replacement by full-thickness corneal donor tissue. The procedure is performed for either optical reasons (restoration of corneal clarity) or tectonic reasons (restoration of structural integrity). At present, PK addresses both endothelial and stromal failures in either structure or function. With current and future developments, posterior lamellar keratoplasty with endothelial replacement may become an alternative to PK for cases of endothelial failure with a clear, healthy stroma. Most surgeons favor a PK over an anterior lamellar keratoplasty for deep stromal diseases because the visual acuity results appear to be better with PK. Deep anterior lamellar keratoplasty is, however, being revisited. Anterior and posterior lamellar keratoplasties are discussed in
Chapters 62 and
63.
In 1838, Kissam performed a xenograft from the pig to a human, which failed (
1). Zirm, however, is the first to have performed a successful human corneal PK in 1905, in Eastern Europe. In Prague, Elschnig emphasized the use of PK soon after 1910 (
2). Tudor-Thomas popularized keratoplasty in Great Britain two decades later (
3). An increased interest in PK arose with the arrival of corticosteroids in the 1950s, with the development of improved microsurgical techniques in the 1970s, including operative microscopes and fine sutures, and with improvements in availability and preservation of corneal tissue (
4,
5) (
Fig. 61-1). PK has become the most frequently performed solid tissue transplantation, with over 46,949 corneal donor grafts obtained from the Eye Bank Association of America in 2000 used for transplantation in the United States (71% of donor grafts) or exported internationally (
6).
When low- and high-risk PK cases are combined, corneal transplantation is as successful as kidney transplantation, with a 75% success rate at 5 years (
7). In low-risk clinical situations, PK is one of the most successful transplantations, with a 10-year success rate, defined as corneal clarity, of 72% to 80% (
8,
9,
10). This very high success rate in uncomplicated cases is despite the fact that tissue matching is not routinely performed and that systemic immunosuppression is rarely used unless required by high-risk clinical indications. Repeat corneal transplantation (
10,
11,
12,
13) and other high-risk cases, in particular recipients with significant corneal vessels (
10,
11,
14), carry a poor 40% to 50% success rate, comparable with that of liver transplantation (
7).
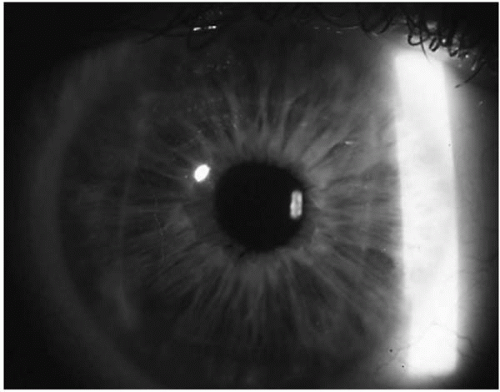
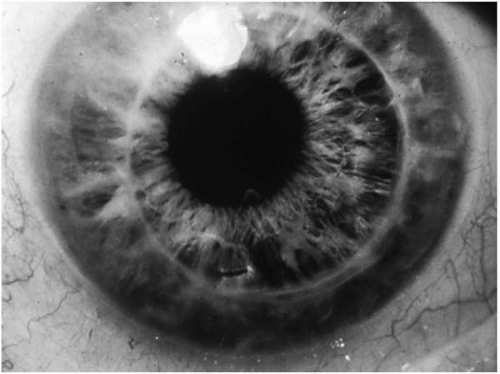
A successful outcome after PK should, however, be measured not only by corneal clarity (
Fig. 61-2). A clear cornea does not always correspond to improved visual acuity in the grafted eye, mostly because of residual regular and irregular astigmatism (
15). Also, daily-life functional improvement after PK is greater if the level of vision is low in the other eye (
16,
17,
18).
This chapter reviews donor and recipient preoperative considerations, the PK surgical procedure, surgical complications and their management, and immunologic rejection and tissue matching.
DONOR CONSIDERATIONS
Although there are anecdotal reports of xenografts, human donor corneas with a viable endothelial layer are required for corneal allografts. At present, one of the most important determinants of a successful corneal transplant program is high-quality eye bank screening and processing of human donor corneal tissue. Artificial corneas made of 2-hydroxyethyl methacrylate (PHEMA) with porous skirts are being developed (
19). Similar to a keratoprosthesis, these artificial corneas can be associated with wound healing problems at the recipient-artificial cornea interface (
20). Although promising, there is no indication that artificial corneas will substantially replace human donor tissue in the next few years.
Donor screening for infectious diseases is essential to protect recipients from severe or life-threatening illnesses by donor tissue transmission of human immunodeficiency virus (HIV) (
21) and prions (
22,
23,
24). Donor serology is used to screen for syphilis, hepatitis, and HIV (
25). Eye bank staff aim to detect donor risk behaviors for HIV with a detailed sociobehavioral history. They also screen for Creutzfeld-Jakob disease, searching for the quadrate clinical prodrome of cognitive changes, speech abnormalities, cerebellar findings, and myoclonus or a history of recent travel to countries
with reported prion encephalitis. There is no proven laboratory test yet available to eliminate the presence of prions in ocular tissue. The only available experimental marker testing for the presence of prions is the protease-resistant isoform of the prion protein. It has been detected in the human retina and optic nerve, but not yet in the cornea (
26). It therefore is theoretically probably safer to procure the donor cornea with a scleral rim directly from the donor than to enucleate the donor before cutting out a corneoscleral button. There are other factors that bear on the decision about the suitability of donor tissue for transplantation. The Eye Bank Association of America has an ongoing committee that periodically reviews available data and sets criteria for donor tissue selection and eye banking in the United States. Its most recent exclusion criteria, which are followed in many other countries, are reproduced in
Table 61-1.
In our experience, donor corneas obtained from infants younger than 18 months of age should be avoided for transplantation because corneal ectasia and high myopia tend to develop in recipients after PK. Although it is common for surgeons to refuse corneal tissue from older donors, the scientific literature is not conclusive about this matter (
27,
28,
29,
30,
31,
32,
33,
34,
35,
36). There are reports suggesting that, given a normal endothelial cell count, older tissue performs equally as well as younger tissue. A 5-year prospective, masked trial designed to determine the safety and efficacy of using older donor tissue for keratoplasty is currently underway: the Cornea Donor Study. Specular microscopy with corneal endothelial cell count on donor tissue of all ages is an important preventive measure against primary donor failure.
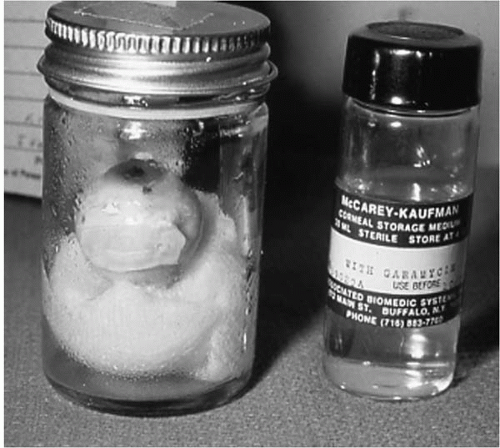
Adequate donor cornea preservation before PK is essential because PK requires a viable donor endothelial layer that can sustain the surgical trauma and future cellular changes and cell loss (
37). A variety of methods have been developed to ensure endothelial cell viability since the earlier methods of storage at 4°C and the first storage media introduced by McCarey and Kaufman (
4) (
Fig. 61-3). Most surgeons now use storage in nutrient media such as Optisol for up to several days (
38) from the time of donor cornea procurement to the time of surgery. Other surgeons, mostly in Europe, have developed methods of long-term incubation at 37°C for several weeks before transplantation (
39,
40,
41). Cryopreservation (
42) is an alternative rarely used today because the local need for corneal tissue exceeds the supply.
TISSUE MATCHING
The benefits of donor-recipient tissue matching to prevent allograft immune rejection and ultimate graft failure are still controversial. The normal cornea enjoys a relative immune privilege well described by Streilein (
43), with a low antigen load, few antigen-presenting cells, and a donor-specific anterior chamber (AC)-associated immune deviation that develops after transplantation. The suppression of the delayed-type hypersensitivity immune reaction is elicited by the intracameral inoculation of allogeneic antigens (
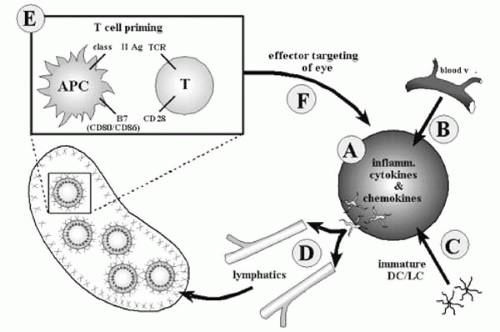
44). This immune privilege is nonetheless relative. Both major
and minor histocompatibility antigens present in the donor cornea can activate lymphokines as well as donor and recipient antigen-presenting cells to trigger lymphocyte proliferation in the draining lymph node (
Fig. 61-4). If activated, these lymphocytes will return to the eye to destroy donor corneal cells.
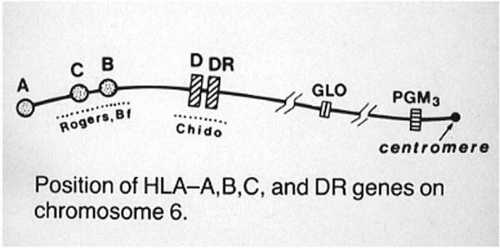
Major histocompatibility complex (MHC) antigens, known in humans as human leukocyte antigens (HLA), are genetically determined protein antigens. Class I MHC antigens such as HLA-A and HLA-B are present on all human living cells, including corneal cells. The class II MHC antigen (HLA-DR) phenotype is expressed on circulating cells and antigen-presenting cells, as in inflamed or vascularized corneas, and on Langerhans dendritic cells (
Fig. 61-5).
In the rat animal model, class I MHC and non-MHC (i.e., minor histocompatibility antigens) antigen mismatching is associated with significantly lower rejection-free graft survival rates (
45,
46). This is probably also the case in humans. The large prospective cohort studies on class I HLA-A and HLA-B matching were based on serologic specificities, with variable reproducibility of laboratory data from one institution to another. This may in part explain why the Collaborative Corneal Transplantation Studies (CCTS) did not confirm the association of good donor-recipient HLA-A and HLA-B matching and improved graft survival with less frequent immunologic rejection episodes (
47,
48,
49,
50). Furthermore, the CCTS protocol probably used enough topical corticosteroids to obscure some effects of tissue compatibility. Class II HLA-DR matching does not appear to be associated with improved graft survival (
47,
51). Some reports have even suggested that a perfect HLA-DR match can be deleterious (
52).
With molecular biology technology, the great polymorphism of the HLA system is now better recognized. For example, the 21 HLA-A antigens determined as serologic specificities are now known to correspond to 225 alleles determined as nucleotide sequences (
53). The HLA polymorphism may theoretically be limited by race matching (
53), which limits the pool of different possible alleles. Until revisited with cheaper HLA matchmakers based on
nucleotide sequence allele determination and large cohort studies, class I HLA-A and HLA-B matching is probably not more cost-efficient than using systemic or intensive topical immunosuppression. Avoiding, whenever possible, corneal donor grafts of 8 mm or larger is probably a good preventive measure for decreasing the antigenic load and rate of immune rejection and failure (
47).
Minor histocompatibility antigens are small sugar antigens that can be attached to MHC antigens (
54). ABO blood group and male sex Y-antigens are such minor histocompatibility antigens. ABO blood group matching prevents early allograft rejection and failure in vascularized corneas in high-risk patients (
12,
55,
56). The current state of knowledge about tissue matching for corneal transplantation programs is that ABO blood group matching prevents graft failure at a currently acceptable cost in high-risk patients.
RECIPIENT CONSIDERATIONS
The most common indication for PK is pseudophakic corneal edema, although there is a decreasing trend for this indication (
6), which accounted for 20% of cases in 2000 according to Eye Bank Association of America survey statistics. Fuchs’ dystrophy, repeat corneal transplantation, and keratoconus are the next most frequent indications. Their order of frequency and the percentage of cases for these three indications vary from one study to another (
57,
58,
59,
60). Corneal opacity as the end result of trauma or inflammatory or infectious conditions (herpes simplex virus [HSV], in particular) and hereditary stromal dystrophies are other conditions that may benefit from PK. The surgeon should, however, have exhausted all medical measures (antiinfectious, antiinflammatory, and hypertonic agents) and should have attempted visual correction by optical means (e.g., contact lenses) before recommending a PK procedure for these conditions.
There is a trend toward increasing numbers of repeat corneal transplantation in the United States and certain parts of Canada (
6,
57,
60,
61). This may in part be due to the fact that corneal donor tissue is more readily available in these locations. Repeat PK has a poorer outcome compared with primary PK (
11,
13,
61,
62,
63,
64). The recipient with a previous history of graft failure has often been exposed to poor prognostic factors such as presence of corneal vessels, peripheral anterior synechiae, and prior immune allograft reaction mediators (
13,
65).
Restoration of optical clarity for the aforementioned indications is therefore the most frequent goal of PK. Tectonic PK is also indicated for those situations in which lamellar keratoplasty would not be expected to alleviate the situation. Corneal perforations, ongoing diffuse inflammatory processes in which medical measures have failed to halt stromal loss, might be indications for tectonic PK. The surgeon should consider a tectonic lamellar keratoplasty for cases with marked variations in stromal thickness.
The surgeon must be convinced that the patient will benefit from PK. The macular and optic nerve function should be assessed to ensure a reasonable visual potential. Pupillary reflexes to light, visual fields, B-scan ultrasonography, optical coherence tomography, and electrophysiology testing should be performed as needed. Intraocular pressure control in patients with glaucoma before or at the time of surgery is essential because a preoperative diagnosis of glaucoma comorbidity is the primary risk factor for corneal graft failure. Although high pressure itself can usually be controlled after surgery by a combination of medical and surgical means, there is a fourfold increased risk of graft failure for recipients with a preoperative diagnosis of glaucoma or increased intraocular pressure (
11,
65,
66). Preoperative glaucoma is frequently made worse after PK by partial loss of the filtration angle. The chronic use of steroids after PK may also induce glaucoma in patients who are steroid responders. Abnormally low preoperative intraocular pressure, such as in patients with chronic uveitis,
may be further aggravated by the surgery, causing macular edema and poor visual outcome.
Any intraocular inflammation must be controlled before PK unless surgery is required in an emergency situation (e.g., corneal perforation). The outcome of a PK is much poorer for patients with active corneal herpetic inflammation than for patients with a quiet herpetic corneal scar (
67,
68). The presence of deep corneal vessels is associated with a twofold increased risk of allograft immune reaction and failure (
10,
50,
69).
Ocular surface conditions such as cicatricial conjunctival diseases (e.g., ocular cicatricial pemphigoid and the Stevens-Johnson’s spectrum of diseases), severe dry eye (e.g., Sjögren’s syndrome), or limbal stem cell deficiency conditions (e.g., congenital aniridia, chemical burn) all carry with them a dire prognosis for PK because epithelial healing is very poor in such conditions. Limbal stem cell transplantation alone for congenital aniridia keratopathy (
70,
71) should be considered. For cicatricial conjunctival diseases with corneal scarring, either a two-step procedure with limbal stem cell transplantation followed by PK or a keratoprosthesis is preferable to PK. Persistent epithelial defects, stromal melting, and corneal perforation may well develop after PK in these patients.
Major mechanical or inflammatory lid abnormalities must be noted and corrected before surgery. Lid notching and malposition or incomplete lid closure may all produce localized or generalized areas of inadequate corneal epithelial wetting, causing corneal melting. Patients with severe chronic blepharitis and atopic blepharitis are at high risk for graft infection and melt (
72). These conditions must be under control at the time of and after PK.
The level and expectation of improvement in quality of life after PK depend on the best eye corrected visual acuity (
17,
18,
73). Consideration of the vision in the other eye is therefore important. Patient satisfaction is better predicted by subjective outcomes than by objective outcomes such as visual acuity (
74). The needs of the patient as defined by age, occupation, and preferred activities of daily living must also be taken into account. The patient’s and family’s compliance with postoperative care and safety recommendations must be taken into consideration, particularly for PK in the pediatric age group and in patients with mental retardation. One must also consider the general health status of the patient. Severe obesity is also associated with intraoperative complications (
75).