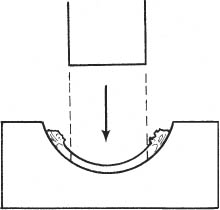
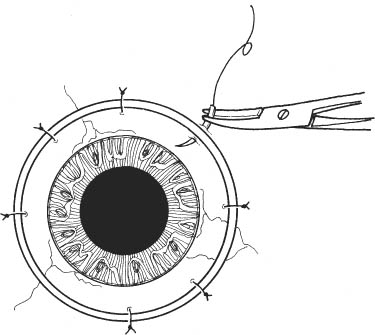
15 See Chapter 3. 1. Phakic eye Pilocarpine 1% every 15 minutes beginning 1 hour before surgery for a total of three drops to produce miosis, which protects lens during surgery. Alternatively, intraoperative acetylcholine (Miochol) may be used. 2. Aphakic eye a. If anterior vitrectomy is anticipated, it may be facilitated by preoperative pupil dilatation (e.g., tropicamide 1%, cyclopentolate 1% and phenylephrine 2.5% every 15 minutes beginning 1 hour before surgery). b. If a vitrectomy is not planned, preoperative dilation or constriction is unnecessary. 1. Anesthesia: Retrobulbar or peribulbar injection plus lid block. May use general anesthesia if preferred, and for younger or uncooperative patients, hearing or mentally impaired patients, those with language obstacles, or patients with ruptured globes. 2. Decompress eye to avoid positive vitreous pressure. a. Mannitol 20% solution, 250 ml intravenous (slow drip over 1 hour) given 1 hour preoperatively. b. Patient to void before entering operating room. c. Secure Honan balloon in position for ~15 minutes (except in cases with globe perforation). 3. Prep and drape. a. Use povidone-iodide 5% on a cotton-tipped applicator to gently clean eyelashes and lid margins. b. Place one or two drops of povidone-iodide in the conjunctival fornix. Note: There are many different trephines and corneal punches. The system used is based on surgeon preference. Figure 15.1 4. Trephine donor button from corneoscleral rim (Fig. 15.1). Note: Secure a sterile work area with comfortable surgeon access and adequate lighting, away from the surgical instruments and patient (e.g., work table with stool) a. Hold corneoscleral rim with toothed forceps (e.g., Bishop-Harmon). b. Remove residual fluid from epithelial side of donor to avoid sliding during trephination (cellulose sponges). c. Place donor tissue epithelial side down (endothelial side up) and center on Teflon cutting block. d. Trephine appropriately sized button (disposable trephine on universal handle). Note: An 8.0 mm donor button placed into a 7.5 mm recipient bed is a standard size differential. i. Keep trephine perpendicular to cornea. ii. Punch button in one fluid motion through entire donor thickness to avoid beveling the edge (listen for “crunch” sound). iii. May use guillotine-style trephine to better control trephination. e. Before removing trephine, ensure that the cut is through full-thickness cornea by gently raising the remaining scleral rim from the cutting block with toothed forceps, leaving the donor button behind. f. Remove trephine. g. Place a few drops of storage medium on the endothelial side of the button and cover the block to prevent drying of the donor. h. Keep corneal donor on work table in secure location and inform all operating room staff. i. Send corneoscleral rim and storage media for culture. 5. Return attention to the patient’s eye. 6. Insert lid speculum, attempting to minimize pressure against globe from lid speculum. a. Optional: Place 4–0 silk bridle sutures. Figure 15.2 7. Secure Flieringa ring (Fig. 15.2). a. Choose ring size to leave ~2–3 mm between the ring and limbus. b. Secure globe with toothed forceps. c. Secure ring using four to eight equally spaced interrupted 7–0 Vicryl sutures. d. Place sutures through conjunctiva and episclera. e. Tie all sutures to equal tension to avoid distortion of globe. Note: A Flieringa ring is not necessary in phakic keratoplasty, unless there is a possibility of lens removal at the time of surgery. a. Stain the corneal indentations with methylene-blue or gentian-violet marking pen or b. Use cautery at limbus to more permanently mark the cardinal positions. 9. Dry host corneal surface using Weck cell sponges. 10. Perform recipient trephination. Note: Trephine system is based on surgeon preference. Systems include Hessburg-Barron, Storz, Hanna, and Krumeich. a. Storz or Weck handheld trephine: i. Preset at ~0.6 mm depth, depending on measurement of corneal thickness.
Penetrating Keratoplasty
Indications
 Replacement of optically inadequate cornea for visual rehabilitation (e.g., scarring, edema, dystrophy, degeneration)
Replacement of optically inadequate cornea for visual rehabilitation (e.g., scarring, edema, dystrophy, degeneration)
 Tectonic support in cases of severe corneal melting, thinning, and impending or frank perforation
Tectonic support in cases of severe corneal melting, thinning, and impending or frank perforation
 Removal of infected cornea in certain cases of recalcitrant microbial keratitis
Removal of infected cornea in certain cases of recalcitrant microbial keratitis
 Select traumatic corneal injuries
Select traumatic corneal injuries
 Select cases of disfiguring corneal opacity for cosmesis
Select cases of disfiguring corneal opacity for cosmesis
Preoperative Procedure
Pupil Management
Instrumentation
 Honan balloon
Honan balloon
 Mannitol 20% solution
Mannitol 20% solution
 Speculum (Lieberman or Barraquer)
Speculum (Lieberman or Barraquer)
 Fine tissue forceps (e.g., 0.12 mm straight Castroviejo, 0.12 Colibri, Pierse)
Fine tissue forceps (e.g., 0.12 mm straight Castroviejo, 0.12 Colibri, Pierse)
 Bishop-Harmon forceps
Bishop-Harmon forceps
 Teflon cutting block
Teflon cutting block
 Cellulose sponges
Cellulose sponges
 Disposable trephine (e.g., Katena, Storz, Weck)
Disposable trephine (e.g., Katena, Storz, Weck)
 Vacuum trephine (e.g., Hessburg-Barron)
Vacuum trephine (e.g., Hessburg-Barron)
 Sutures (7–0 Vicryl, 4–0 silk, 10–0 nylon)
Sutures (7–0 Vicryl, 4–0 silk, 10–0 nylon)
 Kalt or other strong needle holder
Kalt or other strong needle holder
 Fine nonlocking needle holder
Fine nonlocking needle holder
 Radial keratotomy (RK) marker
Radial keratotomy (RK) marker
 Marking pen (e.g., methylene blue, gentian violet)
Marking pen (e.g., methylene blue, gentian violet)
 Cautery
Cautery
 Microsurgical knife (e.g., Superblade, 15 degree, Beaver #75M)
Microsurgical knife (e.g., Superblade, 15 degree, Beaver #75M)
 Viscoelastic substance (e.g., Healon, Amvisc, Viscoat)
Viscoelastic substance (e.g., Healon, Amvisc, Viscoat)
 Corneal scissors (right and left)
Corneal scissors (right and left)
 Paton corneal spatula
Paton corneal spatula
 Vannas scissors
Vannas scissors
 Westcott scissors
Westcott scissors
 Intraocular lens (IOL) scissors
Intraocular lens (IOL) scissors
 McPherson tying forceps
McPherson tying forceps
 Cyclodialysis spatula
Cyclodialysis spatula
 Flieringa scleral ring
Flieringa scleral ring
 Hemostats
Hemostats
 Jeweler’s forceps
Jeweler’s forceps
 Microvitrectomy suction/cutting instrumentation
Microvitrectomy suction/cutting instrumentation
 Acetylcholine solution (e.g., Miochol)
Acetylcholine solution (e.g., Miochol)
Operative Procedure
Phakic Penetrating Keratoplasty
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


