and Mitrofanis Pavlidis2
(1)
Department of Ophthalmology, Uppsala University Hospital, Uppsala, Sweden
(2)
Augencentrum Köln, Cologne, Germany
25.1 General Introduction
25.2 Instruments
25.3 Tamponade
25.5.1 Instruments
25.5.2 Tamponade
25.5.4 Complications
25.5.5 FAQ
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-319-20236-5_25) contains supplementary material, which is available to authorized users.
Electronic supplementary material
for this chapter is accessible online at http://extras.springer.com/ by searching via the ISBN.
25.1 General Introduction
Video 25.1: IOFB case 1—stepwise surgery
Video 25.2: IOFB case 2
Video 25.3: IOFB case 3
Penetrating eye injuries should be treated by experienced surgeons. These cases are associated with a high complication rate and a guarded prognosis, and the initial surgical intervention is of vital importance. There has been a long debate about the timing and the extent of the initial surgical intervention.
We prefer a stepwise approach. See Flow chart 25.1. The first step is the primary closure of the wound (cornea or sclera). We do not remove an opacified cataract in the same session. If there is suspicion of a nonsterile penetration, we inject intravitreal antibiotics. We treat the patient then for 10 days with intravenous antibiotics (1,5 g Zinacef® three times daily). We examine the posterior segment with ultrasound. If the retina is attached, we continue to wait; if the retina is detached, we operate immediately. After approximately 2 weeks, we perform a cataract surgery and implant an IOL. In many cases, the lens capsule is injured. We try to implant the IOL into the bag or into a stable sulcus position. Then approximately 2 weeks after phacoemulsification, we perform vitrectomy with foreign body extraction. Vitrectomy is easy because a PVD is present and the retinal wound has healed. The risk of bleeding from the retinal/choroidal wound is much less, and the risk of PVR from the wound edges is highly reduced.
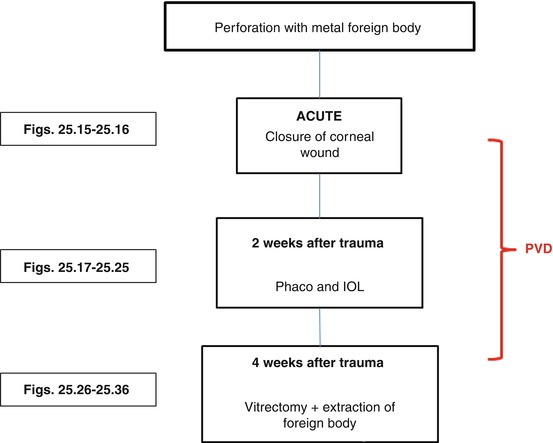
Flow chart 25.1
Our treatment algorithm for stepwise IOFB surgery. After 4 weeks, a PVD is present, the eye is quiet and the PVR risk is low when extracting the IOFB. If the retina is detached, we operate at once
We do not prefer the immediate surgery because (1) the experienced retinal team is often not present when the trauma case arrives at the clinic, (2) a PVD is not present, and (3) if retinal wounds are present and if the foreign body sticks in the retina, then immediate extraction will cause bleeding from the exit wound and result in PVR from the wound edges. Four weeks of waiting will quieten the retinal wound, and the foreign body can be extracted without bleeding or PVR from the wound edges (Figs. 25.1, 25.2, 25.3, 25.4, 25.5, 25.6, 25.7, 25.8, 25.9, 25.10 and 25.11).
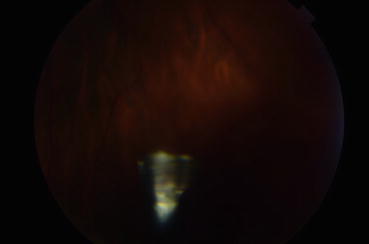


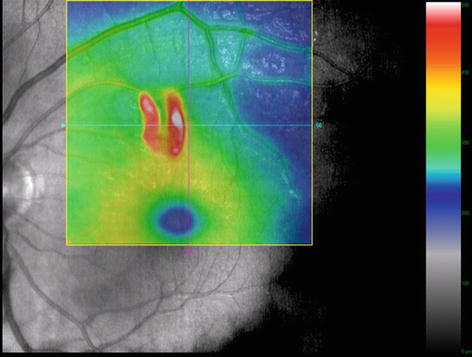
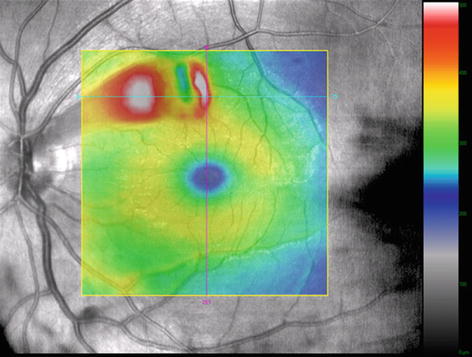
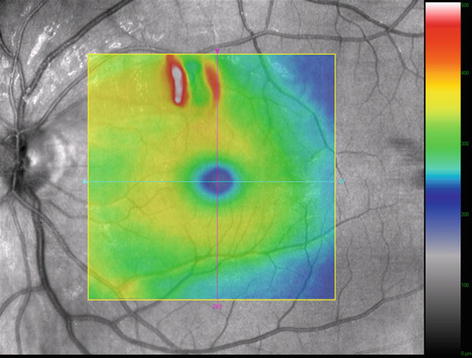
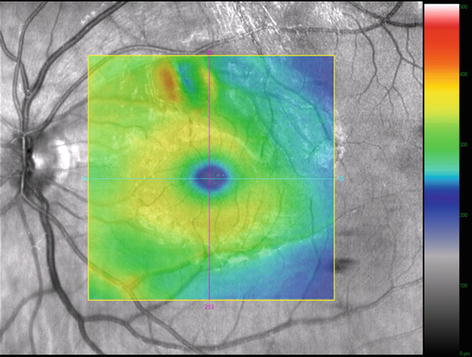
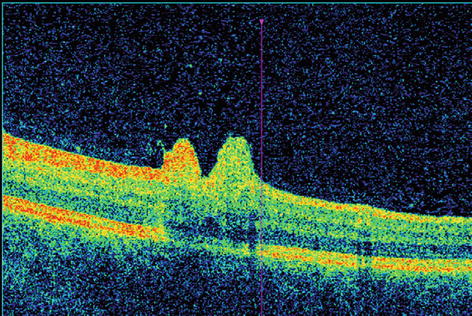
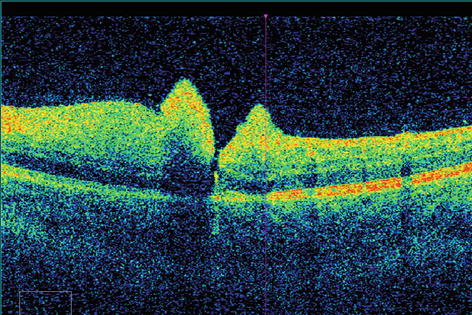
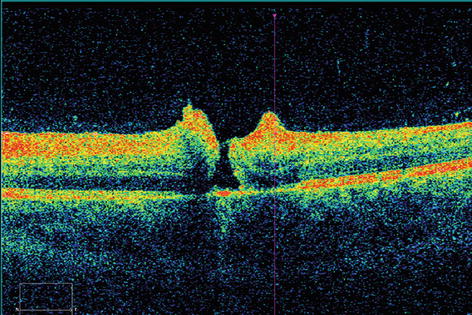
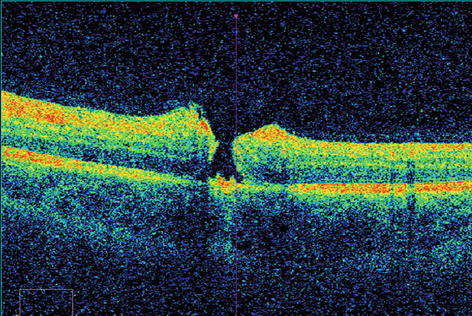
Fig. 25.1
This metal foreign body flew from the blade of a lawn mower into the eye of this male patient, impacted superior to the macula and is now located in the inferior part of the vitreous. VA = 1.0
Fig. 25.2
Note the impact site superior to the macula. The photograph is taken 1 day after the injury
Fig. 25.3
This photograph is taken 11 days after the injury. The retinal swelling is reduced
Fig. 25.4
An OCT 1 day after injury
Fig. 25.5
An OCT 4 days after injury. A severe swelling of the left side of the impact site can be observed
Fig. 25.6
An OCT 11 days after injury. The swelling is reduced
Fig. 25.7
An OCT 20 days after injury. The swelling is almost not noticeable
Fig. 25.8
An OCT 1 day after injury. A section through the impact site
Fig. 25.9
An OCT 4 days after injury. A severe swelling of the inner retina can be observed
Fig. 25.10
An OCT 11 days after injury. The swelling is reduced
Fig. 25.11
An OCT 20 days after injury. A retinal defect remains
We prefer to perform phacoemulsification and vitrectomy at different time points because the posterior capsule is often damaged. Vitrectomy worsens therefore the result of the phacoemulsification if both are performed at the same time points. If phacoemulsification and vitrectomy are performed at the same time, then the extensive vitrectomy with gas tamponade will tamper with the IOL. The gas may luxate the IOL into the anterior chamber, the vitrectomy may cause posterior synechiae and so on.
Surgical Pearls No. 94
Avoid operating an inflamed or vascularly active eye. If the retina is attached, wait and treat the inflammation and vascularization; use steroids and anti-VEGF. If the retina is detached, you have to operate.
25.2 Instruments
1.
27G trocars with chandelier illumination
2.
Endomagnet OR
3.
Diamond dust-coated foreign body forceps
4.
Laser probe
Foreign Body Forceps
The foreign body forceps are executed by a 20G sclerotomy (without trocar) in the eye. Available are 17G, 19G and 20G foreign body forceps. The sclerotomy must of course be enlarged if necessary. I recommend forceps with a roughened surface grip (diamond dusted) (Fig. 25.12a, b).
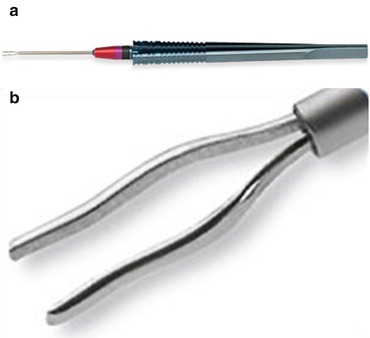
Fig. 25.12
(a) An Avci foreign body forceps. Available in 17G and 20G. DORC. 2286.I. (b) The tip of the foreign body forceps
Endomagnet
Indication: Extraction of a metal foreign body. Synergetics, USA
25.3 Tamponade
Intraoperative: Maybe PFCL
Postoperatively: Air, SF6




