Purpose
To assess the efficacy and safety of intravitreous pegaptanib sodium (Macugen; EyeTech Pharmaceuticals/Pfizer Inc, New York, New York, USA) for macular edema secondary to branch retinal vein occlusion (BRVO).
Design
Prospective, randomized, dose-finding study.
Methods
Twenty subjects from three clinical practices in the United States with BRVO of more than 1 month’s and fewer than 6 months’ duration; best-corrected visual acuity (BCVA) 70 to 25 Early Treatment Diabetic Retinopathy Study letters inclusive (approximately 20/40 to 20/320 Snellen); and central foveal thickness of 250 μm or more were included. Subjects were randomized 3:1 to intravitreous injections of pegaptanib 0.3 or 1 mg at baseline and at weeks 6 and 12 with subsequent injections at 6-week intervals at investigator discretion until week 48. Principal efficacy outcomes were change from baseline to week 54 in BCVA, center point thickness, central subfield thickness, and macular volume as measured by optical coherence tomography.
Results
Fifteen subjects received pegaptanib 0.3 mg and 5 received pegaptanib 1 mg. Eighteen subjects completed the 54-week follow-up. Results were similar in both the 0.3- and 1-mg groups. Overall improvements from baseline to week 54 occurred in mean BCVA (+14 ± 13 letters), center point thickness (−205 ± 195 μm), central subfield thickness (−201 ± 153 μm), and macular volume (−2.2 ± 1.6 mm 3 ). The response was rapid after the first injection, with a mean BCVA improvement of 11 ± 7 letters at 1 week from the baseline of 56 ± 12 letters (approximately 20/80 Snellen). One retinal detachment and no cases of endophthalmitis or traumatic cataract were seen.
Conclusions
Intravitreous pegaptanib offers a promising alternative as a treatment for macular edema secondary to BRVO.
Branch retinal vein occlusion (BRVO) typically occurs at an arteriovenous crossing, with venous compression by the more rigid thick-walled artery, degenerative vessel wall changes, and abnormal hematologic factors all believed to be contributing factors. Significant visual impairment may result from the associated perifoveal retinal capillary nonperfusion, edema, and hemorrhage as well as retinal neovascularization. Overall, approximately 50% to 60% of patients with all types of BRVO maintain visual acuity (VA) of 20/40 or better after 1 year. Although some studies report that a slight majority of patients recover some vision without treatment, chronic macular edema (ME), macular ischemia, bleeding into the vitreous from neovascularization, or a combination thereof frequently may account for a poor final VA.
Most of the proposed treatment methods for BRVO, which include antiaggregative therapy and fibrinolysis, isovolemic hemodilution, laser treatment, intravitreous corticosteroids, and intravenous corticosteroids with vitrectomy with sheathotomy, target the sequelae of the occlusion. Unfortunately, well-controlled, prospective, randomized trials supporting their efficacy are significantly limited. Of these treatments, only grid laser photocoagulation has been proved efficacious in a randomized clinical trial.
Over the past decade, investigations into the pathophysiologic features of retinal ischemic disease have elucidated a central role of vascular endothelial growth factor (VEGF) A in promoting both edema and neovascularization. These sequelae reflect the actions of VEGF-A as both the most potent known inducer of vascular permeability and as a key regulator of angiogenesis. Synthesis of VEGF-A is upregulated further by the retinal hypoxia that accompanies ischemia. In clinical studies, VEGF levels were found to be elevated in the vitreous fluid of patients with BRVO compared with patients with nonischemic ocular disease, and this elevation was correlated directly with the severity of ME and the area of nonperfusion ; these findings recently were extended to the aqueous humor as well. Similar correlations have been established for other ischemic retinopathies, including proliferative diabetic retinopathy and central retinal vein occlusion (CRVO), and have prompted interest in the use of targeted anti-VEGF therapies for their treatment.
Pegaptanib sodium (Macugen; EyeTech Pharmaceuticals/Pfizer Inc, New York, New York, USA) is a 40-kDa ribonucleic acid aptamer that binds VEGF 165 selectively, the isoform that exerts especially pathogenic effects in animal models of ischemia-mediated ocular neovascularization and diabetes-induced breakdown of the blood-retinal barrier. Intravitreous pegaptanib is approved for the treatment of neovascular age-related macular degeneration (AMD) and has shown efficacy in phase 2 trials as a treatment for both the edema and neovascularization characteristic of diabetic retinopathy. Pegaptanib has also been shown to confer significant improvements in the VA of patients with CRVO, suggesting that VEGF contributes to the edema and subsequent visual loss resulting from occlusive retinal vascular diseases. Based on this hypothesis, a small prospective, randomized study was conducted to evaluate the effects of 0.3 or 1.0 mg intravitreous pegaptanib in the treatment of BRVO.
Methods
This was a prospective, multicenter, uncontrolled, dose-finding study conducted in 3 retinal specialty practice settings in the United States. Eligible male or female subjects were 50 years of age or older, had ME secondary to BRVO involving the foveal center of more than 1 month’s and fewer than 6 months’ duration before baseline, and had a best-corrected visual acuity (BCVA) in the study eye of between 70 and 25 Early Treatment of Diabetic Retinopathy Study letters inclusive (Snellen equivalent, 20/40 to 20/320) using the 4-m testing method. ME was assessed by optical coherence tomography (OCT; Stratus OCT, Carl Zeiss Meditec, Dublin, California, USA).
Study eyes were required to have a central foveal thickness of 250 μm or more at baseline, and the investigator had to be comfortable with deferring macular laser for 18 weeks from baseline. Subjects with an ophthalmic history of significant cataract, diabetic retinopathy, AMD, glaucoma, uveitis, epiretinal membrane, vitreomacular traction, or tumor were excluded. Additional exclusion criteria were presence of dense hemorrhage or lipid in the foveal center; intraocular surgery within the previous 3 months; significant enlargement of the foveal avascular zone (more than 50% disruption of the capillary ring); likelihood of any evidence-driven indication for peripheral photocoagulation in the next 6 months, prior grid laser within 4 months of baseline, or more than 1 prior grid laser treatment; and prior intravitreous or periocular corticosteroid injections in the study eye. Subjects also were excluded if they showed evidence of spontaneous improvement from the initial examination to day 0 as determined by an improvement of more than 15 letters of vision or by thinning of the center point on OCT of more than 20% from the initial determination. Subjects were randomized 3:1 to receive intravitreous injections of 0.3 or 1 mg pegaptanib sodium at baseline, week 6, and week 12, with subsequent injections at 6-week intervals at the discretion of the investigator until week 48. Macular grid laser treatment was allowed at 18 weeks at the discretion of the investigator and could be repeated every 4 months.
Study Assessments and Endpoints
An ophthalmologic history and all baseline assessments were repeated on day 0, the first study treatment day. The baseline evaluation included BCVA, complete ophthalmic examination, OCT measurement of central foveal thickness, and fluorescein angiography assessment of retinal perfusion. The complete ophthalmic examination and BCVA measurement were repeated at each of 6 weekly preinjection visits and at the week 1 postinjection visit. OCT measurements of central foveal thickness were carried out at baseline and weeks 1, 6, 12, 18, 24, 30, 36, 42, 48, and 54. Subjects were followed up for 54 weeks.
The endpoints included the percentage of treated eyes showing a gain of 3 lines or more in BCVA at 54 weeks and OCT measurements of macular thickness (central point, central subfield, and macular volume) at 54 weeks. The last observation carried forward method was used to replace missing postbaseline data. Safety end points included all adverse events spontaneously reported, elicited, or observed by the investigators at any visit. Adverse events were graded as mild, moderate, or severe and were assessed as being either related to the injection procedure or to the study drug or as being unrelated to the study treatment. All serious adverse events were recorded regardless of whether deemed related to treatment. Descriptive statistics, including means and standard deviations (SD), were calculated. No comparative statistical testing was performed.
Results
The study was conducted between February 2006 and April 2008. A total of 20 subjects (10 males; 10 females) ranging from 58 to 88 years of age was enrolled: 15 were randomized to receive the 0.3-mg pegaptanib dose and 5 were randomized to receive the 1-mg dose ( Table 1 ). One subject had been treated with macular grid photocoagulation 4.5 months before enrollment. All subjects received the first 3 injections (baseline to week 12), and 17 (85%) of 20 subjects returned at week 1 for the OCT assessment. Eighteen subjects completed the 54-week follow-up, with 1 subject in the 0.3-mg group completing therapy by week 19 and another in the 1-mg group completing therapy by week 24 ( Table 1 ). At week 54, the mean and median number of injections was 7.2 and 7.5, respectively, for the 18 subjects who completed the 54-week follow-up. Two subjects required macular grid photocoagulation, 1 at 4 months and the other at 5 and 10 months after enrollment.
| Case No. | Study Eye | Pegaptanib Dose (mg) | Age at BRVO Onset (years) | Follow-up (mos) | No. of Injections | BCVA (Snellen) | Foveal Thickness (μm) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Week 12 | Week 30 | Week 54 (Final) | Baseline | Week 12 | Week 30 | Week 54 (Final) | ||||||
| 01-01 | Right | 0.3 | 73 | 12 | 7 | 20/250 | 20/200 | 20/125 | 20/160 | 439 | 161 | 271 | 606 |
| 01-02 | Left | 0.3 | 78 | 12 | 7 | 20/80 | 20/50 | 20/125 | 20/32 | 294 | 174 | 174 | 283 |
| 01-03 | Left | 0.3 | 66 | 12 | 9 | 20/80 | 20/125 | 20/80 | 20/80 | 516 | 457 | 489 | 249 |
| 01-04 | Left | 0.3 | 72 | 12 | 7 | 20/40 | 20/25 | 20/25 | 20/32 | 508 | 250 | 212 | 160 |
| 02-01 | Left | 1.0 | 69 | 12 | 3 | 20/80 | 20/32 | 20/25 | 20/20 | 434 | 162 | 157 | 170 |
| 02-02 | Right | 0.3 | 72 | 12 | 7 | 20/80 | 20/32 | 20/20 | 20/20 | 341 | 193 | 182 | 145 |
| 02-03 | Right | 0.3 | 58 | 12 | 9 | 20/100 | 20/50 | 20/63 | 20/40 | 624 | 519 | 457 | 443 |
| 02-04 | Right | 0.3 | 78 | 12 | 6 | 20/63 | 20/32 | 20/32 | 20/25 | 473 | 247 | 200 | 136 |
| 02-05 | Left | 0.3 | 62 | 12 | 7 | 20/80 | 20/63 | 20/40 | 20/25 | 465 | 295 | 235 | 269 |
| 02-06 | Right | 0.3 | 71 | 12 | 8 | 20/80 | 20/80 | 20/320 | 20/100 | 411 | 380 | 208 | 219 |
| 02-07 | Left | 0.3 | 74 | 12 | 3 | 20/80 | 20/32 | 20/25 | 20/25 | 416 | 237 | 176 | 165 |
| 02-08 | Left | 1.0 | 84 | 12 | 9 | 20/50 | 20/40 | 20/40 | 20/32 | 512 | 173 | 193 | 167 |
| 02-09 | Right | 0.3 | 80 | 19 wks (EW) | 4 | 20/80 | 20/50 | 20/25 | 20/25 | 635 | 214 | 224 | 224 |
| 02-10 | Left | 0.3 | 75 | 12 | 9 | 20/40 | 26/16 | 20/20 | 20/20 | 501 | 172 | 165 | 131 |
| 02-11 | Right | 0.3 | 63 | 12 | 8 | 20/40 | 20/32 | 20/32 | 20/40 | 516 | 440 | 556 | 594 |
| 02-12 | Right | 1.0 | 69 | 24 wks (EW) | 5 | 20/200 | 20/80 | 20/160 | 20/160 | 860 | 478 | 254 | 254 |
| 02-13 | Left | 0.3 | 87 | 12 | 8 | 20/80 | 20/50 | 20/25 | 20/25 | 509 | 272 | 289 | 261 |
| 02-14 | Left | 1.0 | 88 | 12 | 6 | 20/50 | 20/25 | 20/25 | 20/25 | 454 | 290 | 244 | 257 |
| 03-01 | Right | 1.0 | 75 | 12 | 8 | 20/50 | 20/32 | 20/20 | 20/25 | 503 | 320 | 265 | 404 |
| 03-02 | Left | 0.3 | 85 | 12 | 9 | 20/40 | 20/40 | 20/63 | 20/63 | 357 | 339 | 311 | 542 |
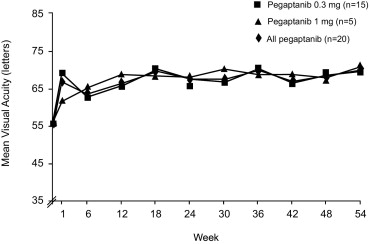
Overall, gains were achieved in mean BCVA with corresponding reductions in center point thickness, central subfield thickness, and macular volume ( Tables 1 and 2 ). The response was rapid after the first injection, with a mean ± SD BCVA improvement of 11 ± 7 letters at 1 week from the baseline of 56 ± 12 letters (approximately 20/80 Snellen; Figure 1 ). After 30 weeks, mean BCVA improved by 12 ± 14 letters, and at week 54, gains increased to 14 ± 13 letters. Similar improvements in mean BCVA were observed with the 0.3- and 1-mg doses. At week 1, 76% of eyes had gained at least 5 letters and 18% had gained 15 letters or more ( Figure 2 ). At week 30, 50% of eyes had gained 15 or more letters. These improvements were sustained at 54 weeks. Two subjects achieved significant reductions in center point thickness without corresponding central VA gains. At baseline, Case 01-03 had significant foveal ischemia masked by intrafoveal avascular zone hemorrhage. The ischemic damage to the neuroretina limited the 54-week visual outcome in this eye. In Case 02-06, clinically significant intrafoveal avascular zone lipid precipitate developed during macular deturgescence. Residual subfoveal fibrous metaplasia of the retinal pigment epithelium limited the week 54 vision in this eye.
| Baseline | Week 54 | Improvement | |
|---|---|---|---|
| BCVA, letters (Snellen) | 56 ± 12 (20/80) | 70 ± 15 (20/40) | 14 ± 13 |
| Center point thickness (μm) | 489 ± 121 | 284 ± 152 | 205 ± 195 |
| Central subfield thickness (μm) | 487 ± 107 | 286 ± 125 | 201 ± 153 |
| Macular volume (mm 3 ) | 10.0 ± 1.4 | 7.8 ± 1.5 | 2.2 ± 1.6 |

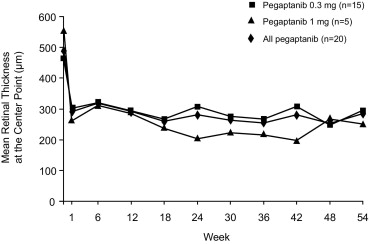
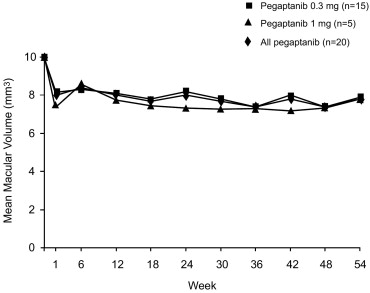
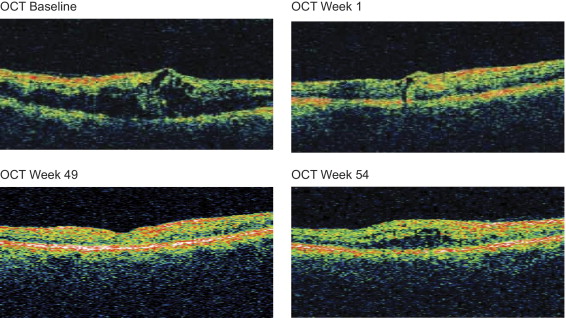
Paralleling the improvement in BCVA, pegaptanib treatment led to a rapid anatomic response in mean retinal thickness at the center point; similar responses were observed with both the 0.3- and 1-mg doses ( Figure 3 ). Center point thickness decreased from a mean ± SD of 489 ± 121 μm at baseline to 291 ± 76 μm at week 1, 263 ± 112 μm at week 30, and 284 ± 152 μm at week 54 ( Table 2 ). In addition, 13 (76%) of 17 subjects who underwent OCT evaluation at week 1 had an absolute reduction in center point thickness of 200 μm or more from baseline. At week 30, 15 (75%) of 20 eyes had a 100-μm or more absolute decrease in center point thickness from baseline; 11 (55%) of 20 eyes had a 200-μm or more decrease. At week 54, reductions in center point thickness of 100 μm or more were maintained, and 10 (50%) of 20 eyes had a 200-μm or more decrease. Similar reductions were also observed for mean macular volume ( Figure 4 ). Figure 5 shows the anatomic response in a 64-year-old male at baseline and at weeks 49 and 54.