Pediatric Radiation-Induced Cataracts in Retinoblastoma
Rupal H. Trivedi
M. Edward Wilson
Retinoblastoma (RB) represents the most common primary intraocular malignancy in children. Historically, bilateral disease was managed by enucleation of the more involved eye and globe-conserving therapy for the less involved eye. Unilateral tumors generally were treated with enucleation. Treatment has evolved to globe-conserving therapies for both eyes in the setting of bilateral disease and in select cases of unilateral disease. Chemoreduction in combination with local ablative therapies has become the standard of care in lieu of external beam radiotherapy (EBRT) because of radiation-related complications (e.g., cataract). However, EBRT continues to be applied as “salvage” treatment for eyes failing chemoreduction therapy or in the setting of extraocular extension and orbital disease.
The major ocular complication of EBRT is radiation-induced cataracts. The crystalline lens is the most radiosensitive structure in the eye, with doses <2 Gy causing cataract formation. Recent studies indicate that the threshold for cataract development is less than was previously estimated and is approximately 0.5 Gy.1 The treatment of RB requires doses in excess of 40 Gy, so cataract formation is an expected side effect.2 Cataracts impair both the visual development of the child and the ability of the ophthalmologist to examine the eye. Radiation-induced cataracts can be formed as these rays penetrate the cornea and interact with the molecular components of the lens. Kase et al.3 showed that growth factors produced by RB cells may lead to cataract formation. The RB cells lack cohesion. Therefore, detached fragments of tumor are easily separated from the main mass, spread throughout the globe, and seed themselves onto other internal structures including the lens capsule, zonule, ciliary body, iris, and cornea. The tumor deposits in certain parts of the globe influence the clinical behavior. Tumor cells on the lens capsule may lead to secondary cataract.4 Radiotherapy-induced cataracts occur as a result of damage to the germinative zone of the lens epithelium, leading to cell death, compensatory mitosis, and generation of “Wedl” cells. The morphology of radiation-induced cataract was described by Cogan and Donaldson.5 Following exposure of the lens to radiation, there is a latent period of variable length, depending largely on the radiation dose and the age of the patient. The initial changes are seen as vacuoles at the posterior pole, followed by involvement of the cortex. Posterior subcapsular cataract is the most common morphology seen in such eyes. Transforming growth factor-β is known to potentiate radiation effects.
The incidence of radiation-induced cataracts has decreased dramatically because of the growing popularity of chemotherapy rather than radiation and lens-sparing radiotherapy techniques. This may be achieved simply by irradiating the posterior aspect of the globe. When more focused methods are employed or the target is prone to motion, fixation of the globe is required. Such immobilization is available at highly specialized centers of ocular oncology.6 A 1990 study reported that 2 of 23 (9%) eyes developed cataracts after episcleral plaque therapy, 4 of 21 (19%) developed cataracts after EBRT, and 9 of 29 (31%) after combined episcleral plaque and EBRT therapy.7 A 1995 study reported that cataracts occurred in 9/11 (82%) eyes with anterior field techniques and 1/8 (12%) eyes treated with lens-sparing techniques.8 A 1999 study reported radiation-induced cataracts in approximately 20% of eyes over 36 months of follow-up, even when relative lens-sparing radiation protocols are used.9 In 2001, a series was reported where cataract surgery after RB treatment was needed in 45 of 900 (5%) eyes.10 In 2009, Chodick et al.11 reported risk of cataract extraction among adult RB survivors. Authors evaluated 828 eyes for an average of 32 years of follow-up. During this period, 51 cataract extractions were reported. One extraction was reported in an eye with no radiotherapy compared with 36 extractions in 306 eyes with one course of radiotherapy and 14 among 38 eyes with two or three treatments.
Eyes exposed to 5 Gy or more had a sixfold increased risk of cataract extraction compared with eyes exposed to 2.5 Gy or less.
Eyes exposed to 5 Gy or more had a sixfold increased risk of cataract extraction compared with eyes exposed to 2.5 Gy or less.
The interval from EBRT to documentation of a radiation-induced cataract ranged from 9 to 48 months (median, 20 months).12 Portellos and Buckley13 performed surgery for cataract a mean of 54 months after EBRT. In a series by Honavar et al.,10 the mean time interval for cataract surgery was 26 months after the final treatment for RB. As the average age at diagnosis of RB is 18 months, it is reasonable to assume that most of the eyes developing cataracts are still within the amblyogenic age range. However, lifelong follow-up is required as mentioned above. In adult RB survivors, the average time interval to cataract extraction in irradiated eyes was 51 years following one treatment and 32 years after two or three treatments.11
Secondary cataract formation complicates the management of RB by precluding visualization of the tumor and may necessitate enucleation if there is suspicion of tumor recurrence. Intraocular surgery in these eyes raises genuine concerns about the patient’s systemic outcome because of the risks for viable tumor seeding.10,14,15 However, surgical intervention for cataracts is justified in certain clinical settings, especially if the tumor is judged to be clinically stable and in regression.10 A few case reports have documented simultaneous association of RB with cataract.16,17,18 Our focus in this chapter is to review the literature and provide guidelines regarding management of secondary cataracts in eyes with RB (Figs. 40.1 and 40.2).
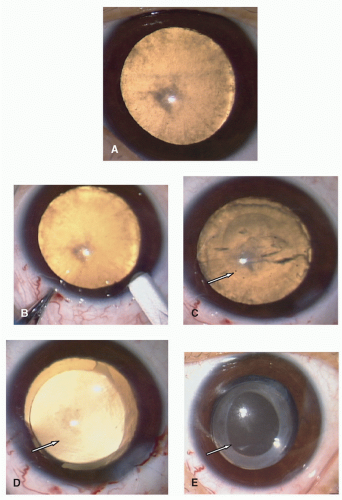 Figure 40.1. A: An eye with a radiation-induced cataract (OD) in a 4-year-old child. RB was treated with radiotherapy and chemotherapy. B: Corneal incision. C: Anterior capsulotomy (arrow shows the edge of the capsulotomy). D: AcrySof® IOL implantation in-the-bag. Note the intact posterior capsule; the arrow shows the edge of the anterior capsule. E: Two months after cataract surgery. The arrow shows the edge of the anterior capsule. |
In 1939, Reese19 first reported operative treatment of radiation cataracts. Of the 112 eyes with cataracts, 25 eyes were operated on; intracapsular extraction was done on 16, extracapsular extraction on 6, and linear extraction on 3. Reese19 noted that in cataract caused by irradiation, there is a tendency toward a proliferation of the epithelium under the anterior capsule into a metaplastic fibrous layer. This strengthens the anterior capsule and makes this type of cataract particularly suitable for intracapsular extraction. Extracapsular extraction in such cases is contraindicated because the lens epithelium remaining after the nucleus is extracted may continue to proliferate and form dense fibrous tissue, which tends




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
