Purpose
To study the etiology and characteristics of pediatric cataracts in a large sample from 1 institution.
Design
Observational case series.
Methods
The study population included 778 consecutive cases (1122 eyes) of children presenting with any type of pediatric cataract over a 10-year period. Age at presentation, laterality, cataract morphology and etiology, and presence of strabismus were recorded. Association with systemic diseases or syndromes and coexistent ocular anomalies were noted. Snellen or Allen picture charts were used to record visual acuity, when able.
Results
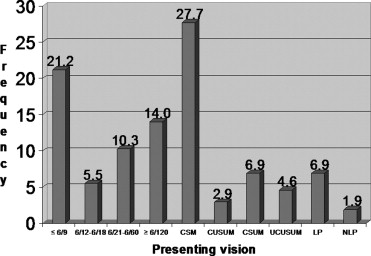
Unilateral cataract accounted for slightly over half of the cases. The etiology was idiopathic in the majority of patients. The most common systemic association was diseases with steroid treatment–induced cataracts. Cataracts, when associated with other isolated ocular anomalies, tended to occur unilaterally. Among syndrome-associated cataracts, Down syndrome represented a third of the cases. Posterior subcapsular cataract was the most common morphologic type. Almost half of the patients presented with Snellen 6/9 or better or “central, steady, maintained” vision where it was not possible to obtain quantitative vision data.
Conclusions
Despite the diverse nature of cases with frequent systemic associations, unilateral cataracts and idiopathic etiology accounted for the majority of cases.
Cataract is a major preventable cause of childhood visual impairment and blindness in the world. Its prevalence has been reported as 1 to 15 per 10 000 children. In developed countries, the prevalence of blindness from childhood cataracts is 0.1 to 0.4 per 10 000 children and approximately 10 times more in developing countries. Globally, an estimated 200 000 children are bilaterally blind from cataracts.
Most of what is known about the epidemiology of childhood cataracts is restricted to studies of congenital cataracts. In the United Kingdom, the incidence of congenital cataracts was reported as 2.49 per 10 000 children in the first year of life, increasing to 3.46 per 10 000 by 15 years. In the United States, the incidence rate has been reported as 2.03 per 10 000 births. In a large cohort prospective study of 55 908 pregnancies in the United States, the prevalence of infantile cataracts was reported as 13.6 per 10 000 infants.
Data on the characteristics of pediatric cataracts are useful for the purposes of diagnosis, genetic counseling, and selection of treatment options. Prevention strategies also require information about etiology. Many studies that examine variables other than overall aggregate incidence are restricted to small numbers of patients. At The Hospital for Sick Children (HSC) in Toronto, we were able to review a large, diverse cohort of patients under care during a 10-year period to better study the etiology and characteristics of pediatric cataracts.
Methods
We retrospectively reviewed the health records of all patients who presented at HSC from January 1, 1992 through December 31, 2002 with any type of cataract cared for by the senior author, Dr Alex Levin, or another ophthalmologist (Dr David Rootman), who managed all the childhood cataract cases at our hospital during that time period. Patients who required surgical intervention were identified using the hospital surgical data program Surgiserver (McKesson Corporation, San Francisco, California, USA). Those who were managed without surgery were identified from the outpatient billing records of the Department of Ophthalmology and Vision Sciences as well as the clinical database of patients seen by Dr Levin. For billing purposes, cataract types and related conditions were coded using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). The following codes were utilized for case identification through the billing records: infantile cataract (366.0), congenital cataract and lens anomalies (743.3), and aphakia and other disorders of lens (379.3).
Individual case records were reviewed to confirm the presence of cataracts. Patients who had cataracts prior to January 1, 1992, with or without surgery, but who received subsequent care during the 10-year interval of interest, were also included. Data were entered into SPSS for Windows version 12.0 statistical software (SPSS Inc, Chicago, Illinois, USA). We recorded the age of each patient at diagnosis, age at surgery (where applicable), laterality, cataract morphology, cataract etiology, and association with systemic disease or syndromes. Coexistent ocular anomalies were also recorded. Prevalence of strabismus was recorded without differentiating development pre or post cataract surgery. Because of the retrospective nature of our study, it was not always clear if the strabismus noted was present preoperatively or postoperatively. Inherited cataracts were defined as morphologically similar cataracts occurring in childhood within the same family and included autosomal dominant, autosomal recessive, and X-linked recessive patterns of inheritance. We recognize that some sporadic cases, in the absence of identifiable causation, may be heritable but were labeled as idiopathic in the absence of other affected family members or an identifiable cause.
The authors acknowledge that it is difficult to identify the cause of cataract or glaucoma in patients with iritis who are also receiving steroids. Patients with cataracts in the presence of iritis were labeled to have “iritis-induced cataracts” even if they were being treated with topical or systemic steroids. Patients with “steroid-induced cataracts” included those whose disease control required systemic steroids as well as those on topical steroids. Likewise, patients whose systemic disease control specifically required systemic steroids and those on topical steroids were included in the category “diseases with steroid-induced cataracts.” Patients with glaucoma in the presence of iritis were labeled to have “iritis-induced glaucoma” even if they were being treated with topical or systemic steroids, unless there was clearly an elevation of intraocular pressure that was relieved by the discontinuation of steroids or the change to another agent known to have a lesser effect on intraocular pressure (eg, switching from prednisolone acetate 1% to fluorometholone).
Presenting visual acuity was recorded using projected Snellen distance or Allen picture charts. In infants and preliterate young children, if preferential-looking data were unavailable, visual acuity was recorded subjectively as “central, steady, maintained” (CSM) and other descriptive qualitative designations ( Figure ).
SPSS statistical software was used to analyze the data. χ 2 and McNemar tests for categorical variables were used with P values of <.05 considered statistically significant.
Results
A total of 1122 eyes in 778 children were identified. 55.5% (432/778) had unilateral cataracts. The right eye was involved in 25.4% (198/778) of cases and the left in 30.0% (234/778) of cases, with the remaining 44.5% (346/778) bilaterally involved. Males comprised 56.2% (437/778) of patients. The median age at presentation was 42.0 months.
The most common diagnostic classification was idiopathic (58.2% [453/778]), followed by traumatic (12.9% [100/778]) and inherited (11.7% [91/778]) cataracts ( Table 1 ). As a group, the most common systemic associations were diseases with steroid treatment–induced cataracts (44.2% [57/129]) and juvenile idiopathic arthritis (18.6% [24/129]) ( Table 2 ). Of the 68 patients who were on steroids, 54.4% (37/68) were on systemic steroids only, 16.2% (11/68) on topical steroids only, and the remaining 29.4% (20/68) were on both. There were 11 cases of congenital infections, with rubella the etiology in 6 cases.
| Etiology | Number of Patients (n = 778) [%] |
|---|---|
| Idiopathic | 453 [58.2] |
| Traumatic | 100 [12.9] |
| Inherited | 91 [11.7] |
| Association with systemic disease not including those on steroids or with iritis | 33 [4.2] |
| Syndromes | 56 [7.2] |
| Steroid-induced (includes patients on topical steroids and those whose disease control specifically required systemic steroids, eg, iritis) | 45 [5.8] |
| Disease | Number of Patients (n = 129) [%] |
|---|---|
| Diseases with steroid-induced cataracts (excluding JIA, SLE, and dermatomyositis) | 57 [44.2] |
| JIA with iritis (all on steroids) | 24 [18.6] |
| Malignancies with nonsteroid treatment–induced cataracts | 15 [11.6] |
| Congenital infection | 11 [8.5] |
| SLE | 6 [4.7] |
| Galactosemia | 5 [3.9] |
| Diabetes mellitus b | 4 [3.1] |
| Sarcoidosis with panuveitis | 2 [1.6] |
| Dermatomyositis (all on steroids) | 2 [1.6] |
| Other c | 3 [2.3] |
a Total number of patients exceeds sample size as patients with both steroid-induced and disease-causing cataracts (eg, JIA with iritis) are included in both categories.
b Previously reported in Wilson ME, Levin AV, Trivedi RH, et al, Cataract associated with type-1 diabetes mellitus in the pediatric population. J AAPOS 2007;11(2):162–165.
c Includes hypothyroidism, Behçet disease, and psoriasis with uveitis.
Among isolated cataracts, 61.9% (280/453) were unilateral ( P < .001, odds ratio 1.9). Among bilateral cases, 50.9% (176/346) were isolated. Among cases with a systemic cause other than syndromes, only 36.0% (46/129) were unilateral ( P < .001, odds ratio 2.4). For those with a family history, 82.4% (75/91) were bilateral ( P < .001, odds ratio 7.2).
A total of 73.7% (73/99) of cataracts associated with other isolated ocular anomalies occurred unilaterally. Persistent fetal vasculature (PFV) accounted for 10.6% (46/432) of all unilateral and 1.7% (6/346) of all bilateral cases. Overall, there were 6 cases of bilateral PFV among the 52 PFV-associated cataract cases (11.5%).
Where specific disease patterns could not be identified, isolated central nervous system anomalies such as microcephaly, ventriculomegaly, and sensorineural hearing loss were most likely to be associated with cataracts ( Table 3 ).
| Organ System | Number of Patients (n = 99) [%] |
|---|---|
| Central nervous system | 48 [48.5] |
| Respiratory system | 19 [19.2] |
| Gastrointestinal system | 9 [9.1] |
| Cardiovascular system | 8 [8.1] |
| Urologic system | 6 [6.1] |
| Limbs and skeletal system | 5 [5.1] |
| Facial anomalies | 3 [3.0] |
| Skin | 1 [1.0] |
a Excludes patients who have cataract-causing diseases or syndromes.
Of the syndromes observed with cataracts, Down syndrome comprised almost a third of cases ( Table 4 ). The median age at presentation of these 18 children was 2.0 months. A third (6/18) had dense total or near-total cataracts, followed next by posterior subcapsular (18.2% [3/18]) and nuclear (15.2% [2/18]) cataracts. The majority (72.2% [13/18]) had bilateral cataracts. Sixteen of the 18 patients (88.9%) required cataract surgery, with a median age at surgery of 3.3 months. Ten patients (55.6%) had strabismus. Six (33.3%) had other ocular anomalies.
| Syndrome | Number of Patients (n = 56) [%] |
|---|---|
| Down syndrome | 18 [32.1] |
| Sturge-Weber syndrome | 5 [8.9] |
| Trisomy 13 | 3 [5.4] |
| WAGR syndrome (Wilms tumor, aniridia, genital abnormalities, retardation) | 3 [5.4] |
| Neurofibromatosis type 1 | 2 [3.6] |
| CHARGE association | 2 [3.6] |
| Stickler syndrome | 2 [3.6] |
| Chondrodysplasia punctata | 2 [3.6] |
| Myotonic dystrophy | 2 [3.6] |
| Other a | 17 [30.4] |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


