Parathyroid carcinoma is a rare tumor that is prone to recurrence and poor local-regional control. Despite advances in technologies that have shown promise for accurate diagnosis, the mainstay of initial diagnosis remains pathologic analysis and clinical assessment. A surgeon’s intraoperative analysis is important in managing patients with parathyroid carcinoma. If parathyroid carcinoma is suspected intraoperatively, a more aggressive surgical strategy should be implemented. This article presents a case series and summary of the existing parathyroid carcinoma literature.
Parathyroid carcinoma is an uncommon endocrine malignancy that was first described in 1904 by de Quervain. de Quervain described a metastatic, nonfunctioning parathyroid carcinoma; subsequent descriptions of functioning parathyroid carcinoma were reported in the 1930s. Since that time, only a few hundred cases have been reported in the literature.
The natural history of parathyroid carcinoma is described as slow but progressive. This entity has a tendency for spread to local lymph nodes with eventual metastasis to the lung and less commonly to the liver and bone. The majority of tumors are functional (ie, they secrete parathyroid hormone [PTH] with resulting elevated serum calcium levels). Morbidity and mortality usually result from unremitting hypercalcemia and its complications rather than mass effect from tumor burden. Nonfunctional tumors present as an expanding neck mass; typically, they are diagnosed at a more advanced stage and subsequently have a generally poorer prognosis. Mortality also is associated with regional disease and metastasis. The cause of parathyroid carcinoma is unknown and at present there are no data describing causal relationships between parathyroid carcinoma and any risk factors.
Epidemiology
The frequency of parathyroid carcinoma is reported as greater than 1% of patients with primary hyperparathyroidism, although a higher rate of 5% is reported from Japan. It is the least common endocrine malignancy, with a prevalence of 0.005% of all cancers. According to a report from the National Cancer Data Base, the estimated incidence is 30 new cases per year in the United States. Most reports indicate an equal gender distribution. The typical age at presentation is reported to be from the 40s to the mid-50s, slightly younger than the average age of patients with primary hyperparathyroidism. Parathyroid carcinoma may occur as a sporadic event or as part of a syndrome; relationships are described with hyperparathyroidism–jaw tumor (HPT-JT) syndrome, multiple endocrine neoplasia types 1 and 2A, and familial hypocalciuric hypercalcemia.
Case studies
Case studies can be a helpful tool in expanding understanding of rare diseases seldom encountered in clinical practice. From the surgical experience of the senior author (BCS) with 8 cases, the following 2 cases are presented.
Patient 1
A 50-year-old man was referred to the authors’ clinic with a chief complaint of dyspnea of more than 1 year’s duration and a right-sided neck mass. Ultrasound (his only preoperative imaging) demonstrated a large, noncystic, right-sided neck mass, which was initially thought a benign colloid goiter. The patient’s preoperative calcium level was incidentally noted as 10.6 mg/dL. Hemithyroidectomy was performed; however, operative findings revealed an exceptionally large right inferior parathyroid mass with mediastinal extension just behind and intimately associated with the thyroid lobe. After this discovery, a blood sample was sent and intraoperative measurement of the patient’s PTH (ioPTH) was 415 pg/dL (normal range, 10–65 pg/mL). Parathyroidectomy with dissection of the tracheoesophageal groove was undertaken. After dissection, his ioPTH level fell to 86 pg/dL and hypercalcemia normalized postoperatively. Histopathologic examination of surgical specimens revealed extensive necrosis and vascular and perineural invasion, leading to a diagnosis of parathyroid carcinoma.
During the surgery, there was a concern that residual disease might have been left in the mediastinum. A postoperative neck and chest CT scan with contrast was ordered ( Fig. 1 ). A right mediastinal lesion was noted. Approximately 1 month later, after the initial surgery, the patient underwent right thoracotomy for excision of a mediastinal mass. Gross findings on thoracotomy included a soft, well-encapsulated mass with necrosis and mustard brown–colored debris that encompassed the right vagus nerve; the involved nerve was sacrificed. Histopathologic examination revealed no evidence of malignancy.

The patient’s PTH levels remained elevated for 10 months after surgery (97 to 160 pg/dL, normal range 12 to 88). During this time, his calcium levels were consistently low to low normal (8.2 to 8.9 mg/dL, normal range 8.7 to 10.5); subsequently, a 25-hydroxy (OH) vitamin D level was obtained and was 14 ng/mL (normal range, 30 to 80 ng/mL). The patient was determined to have vitamin D–deficient secondary hyperparathyroidism and he was repleted. On correction of vitamin D levels (44 ng/mL), his calcium and PTH levels normalized (9.0 mg/dL and 68.2 pg/dL, respectively). PTH and chorioembryonic antigen (CEA) levels were used for surveillance of disease recurrence; although PTH levels fluctuated, his CEA levels remained consistently normal (1.3–2.1 ng/mL, normal range 0.5–10). He refused radiation therapy and has since been only sporadically compliant with follow-up.
Patient 2
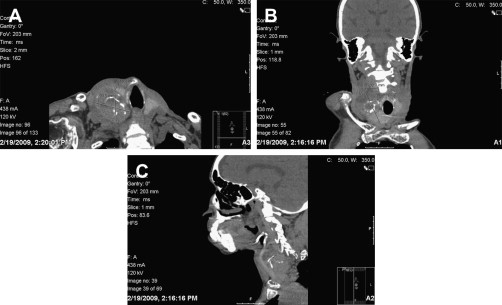
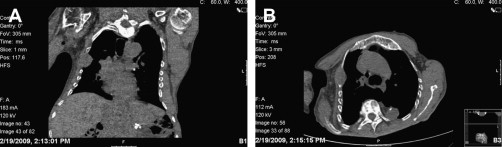
A 63-year-old man was referred to the authors’ clinic for evaluation of a neck mass that had gradually increased in size over a 2-year time period. During this time the patient developed progressive back pain, kyphoscoliosis ( Fig. 2 ), a 50-lb weight loss, and a pathologic fracture of the left scapula while attempting to start his lawn mower. Initial workup revealed a PTH level of 5578 pg/dL, elevated serum calcium and bone alkaline phosphatase, and decreased activated (25-OH) vitamin D. The findings of a palpable neck mass along with massively elevated PTH led to a high index of suspicion for parathyroid carcinoma. Before his scheduled surgery, he was admitted to the hospital in acute renal failure and his hypercalcemia was treated with aggressive hydration. Results of soft tissue CT scan of the neck with contrast were consistent with a malignant neoplasm arising from the right inferior parathyroid ( Fig. 3 ). CT scanning also detected the presence of a mass on the right third rib that was suspicious for a metastasis ( Fig. 4 ).

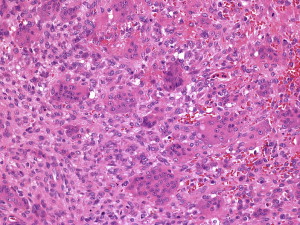
Right-sided inferior parathyroidectomy, hemithyroidectomy, modified neck dissection, and rib resection were performed by a team effort of otolaryngologists and cardiothoracic surgeons. Histopathologic examination of surgical specimens confirmed diagnosis of parathyroid carcinoma with lymphovascular invasion. Examination of the rib mass revealed a fibrohistiocytic lesion with abundant giant cells, which, given the context of hypercalcemia, was identified as a brown tumor of hyperparathyroidism. This is a classic association but rarely encountered in clinical practice ( Fig. 5 ). After resection, his PTH level normalized but hypocalcemia developed due to severe osteoporosis. Unfortunately, the patient’s recovery was complicated by acute tubular necrosis, acute renal failure requiring dialysis, bacteremia, and respiratory insufficiency. Attempts to wean him off the ventilator were unsuccessful. Palliative care was initiated, and he was discharged to hospice care.
Case studies
Case studies can be a helpful tool in expanding understanding of rare diseases seldom encountered in clinical practice. From the surgical experience of the senior author (BCS) with 8 cases, the following 2 cases are presented.
Patient 1
A 50-year-old man was referred to the authors’ clinic with a chief complaint of dyspnea of more than 1 year’s duration and a right-sided neck mass. Ultrasound (his only preoperative imaging) demonstrated a large, noncystic, right-sided neck mass, which was initially thought a benign colloid goiter. The patient’s preoperative calcium level was incidentally noted as 10.6 mg/dL. Hemithyroidectomy was performed; however, operative findings revealed an exceptionally large right inferior parathyroid mass with mediastinal extension just behind and intimately associated with the thyroid lobe. After this discovery, a blood sample was sent and intraoperative measurement of the patient’s PTH (ioPTH) was 415 pg/dL (normal range, 10–65 pg/mL). Parathyroidectomy with dissection of the tracheoesophageal groove was undertaken. After dissection, his ioPTH level fell to 86 pg/dL and hypercalcemia normalized postoperatively. Histopathologic examination of surgical specimens revealed extensive necrosis and vascular and perineural invasion, leading to a diagnosis of parathyroid carcinoma.
During the surgery, there was a concern that residual disease might have been left in the mediastinum. A postoperative neck and chest CT scan with contrast was ordered ( Fig. 1 ). A right mediastinal lesion was noted. Approximately 1 month later, after the initial surgery, the patient underwent right thoracotomy for excision of a mediastinal mass. Gross findings on thoracotomy included a soft, well-encapsulated mass with necrosis and mustard brown–colored debris that encompassed the right vagus nerve; the involved nerve was sacrificed. Histopathologic examination revealed no evidence of malignancy.
The patient’s PTH levels remained elevated for 10 months after surgery (97 to 160 pg/dL, normal range 12 to 88). During this time, his calcium levels were consistently low to low normal (8.2 to 8.9 mg/dL, normal range 8.7 to 10.5); subsequently, a 25-hydroxy (OH) vitamin D level was obtained and was 14 ng/mL (normal range, 30 to 80 ng/mL). The patient was determined to have vitamin D–deficient secondary hyperparathyroidism and he was repleted. On correction of vitamin D levels (44 ng/mL), his calcium and PTH levels normalized (9.0 mg/dL and 68.2 pg/dL, respectively). PTH and chorioembryonic antigen (CEA) levels were used for surveillance of disease recurrence; although PTH levels fluctuated, his CEA levels remained consistently normal (1.3–2.1 ng/mL, normal range 0.5–10). He refused radiation therapy and has since been only sporadically compliant with follow-up.
Patient 2
A 63-year-old man was referred to the authors’ clinic for evaluation of a neck mass that had gradually increased in size over a 2-year time period. During this time the patient developed progressive back pain, kyphoscoliosis ( Fig. 2 ), a 50-lb weight loss, and a pathologic fracture of the left scapula while attempting to start his lawn mower. Initial workup revealed a PTH level of 5578 pg/dL, elevated serum calcium and bone alkaline phosphatase, and decreased activated (25-OH) vitamin D. The findings of a palpable neck mass along with massively elevated PTH led to a high index of suspicion for parathyroid carcinoma. Before his scheduled surgery, he was admitted to the hospital in acute renal failure and his hypercalcemia was treated with aggressive hydration. Results of soft tissue CT scan of the neck with contrast were consistent with a malignant neoplasm arising from the right inferior parathyroid ( Fig. 3 ). CT scanning also detected the presence of a mass on the right third rib that was suspicious for a metastasis ( Fig. 4 ).
Right-sided inferior parathyroidectomy, hemithyroidectomy, modified neck dissection, and rib resection were performed by a team effort of otolaryngologists and cardiothoracic surgeons. Histopathologic examination of surgical specimens confirmed diagnosis of parathyroid carcinoma with lymphovascular invasion. Examination of the rib mass revealed a fibrohistiocytic lesion with abundant giant cells, which, given the context of hypercalcemia, was identified as a brown tumor of hyperparathyroidism. This is a classic association but rarely encountered in clinical practice ( Fig. 5 ). After resection, his PTH level normalized but hypocalcemia developed due to severe osteoporosis. Unfortunately, the patient’s recovery was complicated by acute tubular necrosis, acute renal failure requiring dialysis, bacteremia, and respiratory insufficiency. Attempts to wean him off the ventilator were unsuccessful. Palliative care was initiated, and he was discharged to hospice care.
Presentation
Parathyroid carcinoma is often misdiagnosed preoperatively as primary hyperparathyroidism due to parathyroid adenoma or hyperplasia. Clinical and laboratory findings may suggest carcinoma, but these findings are nonspecific. At this time, there is no external independent reference standard for the diagnosis of parathyroid carcinoma, and histopathologic diagnosis can be equivocal. A palpable neck mass has been reported in approximately half of patients with parathyroid carcinoma but in less than 1% of patients with primary hyperparathyroidism. The degree of hypercalcemia is often more pronounced in parathyroid carcinoma. Calcium levels above 14 mg/dL (normal, 8.5 to 9.9 mg/dL) are common, in contrast to the elevations of 1 to 2 mg/dL above normal levels typically seen in primary hyperparathyroidism. PTH levels are frequently 2 to 10 times the normal values in parathyroid carcinoma (normal intact PTH [iPTH], 10 to 65 pg/mL), whereas PTH levels approximately twice the normal range are more commonly seen in primary hyperparathyroidism. Alkaline phosphatase is also more commonly elevated in parathyroid carcinomas compared with adenomas and hyperplasia; this finding is thought to result from the higher incidence of concomitant bone disease. Hypophosphatemia is not a common feature of the disease. Curiously, parathyroid cancers seem to have a predilection for the inferior parathyroid glands, a finding noted by several investigators.
The most commonly affected organ systems in patients with primary hyperparathyroidism are the renal and skeletal systems. Parathyroid adenomas and hyperplasia are reported to cause renal impairment (nephrolithiasis, nephrocalcinosis, or impaired glomerular filtration) in fewer than 20% of patients. Renal involvement in parathyroid carcinoma is reported as higher, affecting 32% to 84% of patients. Radiologic signs of skeletal abnormalities secondary to hyperparathyroidism (osteitis fibrosa cystica, absent lamina dura, diffuse spinal osteopenia, subperiosteal bone resorption, or salt-and-pepper skull) have been reported in 44% to 91% of patients with parathyroid carcinoma, whereas specific radiologic findings have been reported in less than 10% of patients with benign primary hyperparathyroidism. Patients with parathyroid carcinoma are also at a higher risk for developing complications, such as severe pancreatitis, peptic ulcer disease, and anemia, in other organ systems.
None of these findings is specific to the diagnosis of parathyroid carcinoma. For this reason, a high index of preoperative suspicion and the intraoperative recognition of malignant features are of fundamental importance.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


