Purpose
To examine the clinical, demographic, and anthropometric patient characteristics of secondary pseudotumor cerebri syndrome in children and adolescents based on the recently revised diagnostic criteria.
Design
Retrospective observational case series.
Methods
Patients seen at a tertiary children’s hospital for pseudotumor cerebri syndrome were classified as having either primary idiopathic (n = 59) or secondary pseudotumor cerebri syndrome (n = 16), as rigorously defined by recently revised diagnostic criteria. Outcomes included body mass index Z-scores (BMI-Z), height and weight Z-scores, demographics, and clinical features at presentation, such as headache, sixth nerve palsy, and cerebrospinal fluid (CSF) opening pressure.
Results
In this cohort, the associated conditions and exposures seen in definite secondary pseudotumor cerebri syndrome included tetracycline-class antibiotics (n = 11), chronic kidney disease (n = 3), withdrawal from chronic glucocorticoids (n = 1), and lithium (n = 1). Other associations observed in the possible secondary pseudotumor cerebri syndrome group included Down syndrome, vitamin A derivatives, and growth hormone. In comparison with primary pseudotumor cerebri syndrome, definite secondary pseudotumor cerebri syndrome patients were on average older (15.0 vs 11.6 years; P = .003, Mann-Whitney test). According to US Centers for Disease Control (CDC) classifications, 79% of children with secondary pseudotumor cerebri syndrome were either overweight or obese (36% overweight [n = 5] and 43% obese [n = 6]), as compared to 32% nationally.
Conclusions
Even when a potential inciting exposure is identified for pediatric pseudotumor cerebri syndrome, the possible contribution of overweight and obesity should be considered.
Pseudotumor cerebri syndrome is an umbrella term for the constellation of symptoms caused by elevated intracranial pressure with normal cerebrospinal fluid constituents and brain parenchyma. In adults, primary pseudotumor cerebri syndrome, also known as idiopathic intracranial hypertension, tends to affect obese female individuals of childbearing age who present with headache and papilledema. Pediatric pseudotumor cerebri syndrome shares some, but not all, features of adult pseudotumor cerebri syndrome. Both female sex and obesity are more strongly associated with pseudotumor cerebri syndrome in older, but not younger, pediatric patients. The clinical presentation of pediatric pseudotumor cerebri syndrome may also vary with age, with a greater number of younger patients presenting without symptoms, as compared to adolescents.
Although many cases of pseudotumor cerebri syndrome are idiopathic (ie, primary pseudotumor cerebri syndrome), a number of medications and medical conditions have been associated with the disease (ie, secondary pseudotumor cerebri syndrome). Disease resolution following removal of the presumed trigger has been demonstrated for commonly reported offenders including tetracycline-related antibiotics, withdrawal from chronic glucocorticoid therapy, growth hormone, and retinoids. Presumed causality was further supported in several of these studies, in which rechallenge exposures resulted in recurrence of pseudotumor cerebri syndrome (eg, growth hormone and tetracycline antibiotics). Comprehensive lists of secondary pseudotumor cerebri syndrome associations have been reviewed elsewhere.
Many of the secondary associations in pediatric pseudotumor cerebri syndrome are unique to or more prevalent in childhood, such as growth hormone supplementation and acne therapy involving tetracycline or retinoid medications. Few studies have directly compared primary and secondary pediatric pseudotumor cerebri syndrome, which limits our current understanding of how these subgroups could differ with regard to clinical presentation, treatment response, and pathophysiology. It is thus unclear whether certain demographics might predispose a child to developing secondary pseudotumor cerebri syndrome or whether the risk factors of obesity and female sex are as important for secondary pseudotumor cerebri syndrome as in primary pseudotumor cerebri syndrome.
The purposes of this study were (1) to identify “true” cases of pediatric pseudotumor cerebri syndrome through rigorous application of the recently revised diagnostic criteria, (2) to examine the secondary pseudotumor cerebri syndrome associations seen in a pediatric group, and (3) to compare the initial presentation of primary and secondary pseudotumor cerebri syndrome in children. In particular, we hoped to characterize similarities or differences between the 2 subgroups of pseudotumor cerebri syndrome that might generate new insights into the disease pathogenesis.
Methods
Study Design and Definitions
This study was a retrospective chart review. The following protocol was approved by the Institutional Review Board at The Children’s Hospital of Philadelphia (IRB# 13-010158), including waivers of consent and of Health Insurance Portability and Accountability Act (HIPAA) authorization. Criteria for inclusion in this study are outlined in Figure 1 . Patient charts were identified via an electronic medical record search for ICD-9 code 348.2 and a pediatric neuro-ophthalmologist’s database (G.T.L.) from a tertiary-care children’s hospital (The Children’s Hospital of Philadelphia, diagnoses from July 1, 1993 to April 16, 2013, initial n = 363). Only patients aged 2-18 years were included in the study, as we considered the pathophysiology of any diagnosis in infancy to be distinct. Cases of pseudotumor cerebri syndrome were categorized through manual chart review using recently revised diagnostic criteria for pseudotumor cerebri syndrome.
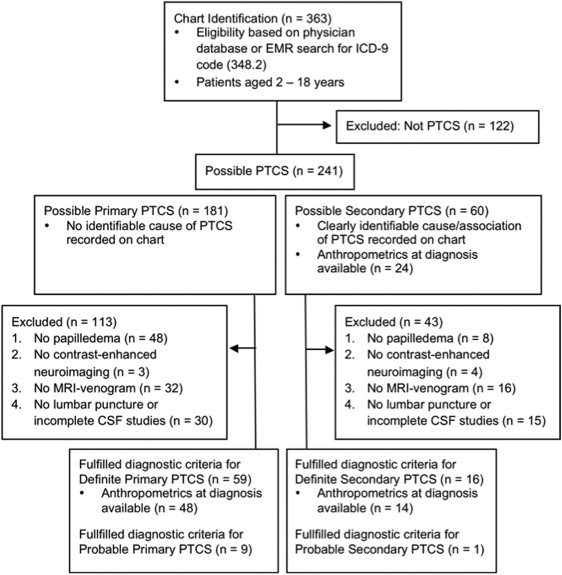
Cases that clearly did not meet the revised diagnostic criteria or represented ICD-9 codes entered in error were considered as not pseudotumor cerebri syndrome ; these cases were hence excluded from the study. Following their exclusion, the remaining pool of cases was defined as possible pseudotumor cerebri syndrome . Next, the revised diagnostic criteria were strictly applied. Cases excluded were those that did not fulfill all of the definite pseudotumor cerebri syndrome criteria, typically because their medical records lacked necessary diagnostic studies (eg, lumbar punctures not completed, cerebrospinal fluid [CSF] results not recorded, or magnetic resonance venography [MRV] studies not done for atypical patients [ie, male patients or nonobese female patients]). Cases were excluded in the order of the criteria as numbered in Figure 1 (eg, a patient without neuroimaging was excluded before a patient lacking lumbar puncture results). Cases of “typical pseudotumor cerebri syndrome patients” (ie, obese and female) did not require an MRV study for inclusion in the definite pseudotumor cerebri syndrome pool. Patients fulfilling all diagnostic criteria except for the requirement of elevated opening pressure on lumbar puncture were identified as probable pseudotumor cerebri syndrome (n = 10). Thus, cases meeting all revised diagnostic criteria were considered to be definite pseudotumor cerebri syndrome (n = 75, of which 59 had primary pseudotumor cerebri syndrome and 16 had identifiable secondary associations).
For both possible and definite cases of pseudotumor cerebri syndrome, primary and secondary subgroups were defined. Primary pseudotumor cerebri syndrome (also known as idiopathic intracranial hypertension) was defined as cases of intracranial hypertension that had no reasonably identifiable cause (aside from obesity) and included young, thin children and patients of both sexes. Secondary pseudotumor cerebri syndrome was defined according to published lists of confirmed and suspected causes of pseudotumor cerebri syndrome or conditions associated with pseudotumor cerebri syndrome. If an obese adolescent female had been exposed to tetracycline antibiotics within 3 months preceding the onset of pseudotumor cerebri syndrome symptoms, we defined this as secondary pseudotumor cerebri syndrome attributable to tetracycline. We chose this 3-month exposure window because the average duration of antibiotic treatment prior to pseudotumor cerebri syndrome diagnosis was approximately 3 months in previous studies, and to strengthen the temporal likelihood of exposure-disease association. If the patient had a chronic medical condition (eg, chronic kidney disease or Down syndrome) with published associations to pseudotumor cerebri syndrome, and that condition was present at the time of pseudotumor cerebri syndrome diagnosis, then we defined that case as secondary pseudotumor cerebri syndrome associated with that condition. The various conditions associated with secondary pseudotumor cerebri syndrome were identified for the group with definite pseudotumor cerebri syndrome (n = 16), as well as for a larger cohort of possible secondary pseudotumor cerebri syndrome (n = 60) that included the definite pseudotumor cerebri syndrome cases as well as cases that did not have complete chart evidence to fulfill the revised diagnostic criteria. For patients with 2 or more potential secondary causes of or associations with pseudotumor cerebri syndrome, manual chart review and reassessment by 1 of the authors (G.T.L.) were employed to determine the most likely primary cause or association based on proximity of exposure and magnitude of the expected effect. For example, if a patient had a remote history of retinoid use but developed pseudotumor cerebri syndrome less than 3 months after starting tetracycline, the secondary pseudotumor cerebri syndrome was attributed to the antibiotic.
Patient Characteristics of Interest, Data Management, and Data Analysis
For the definite cases of pseudotumor cerebri syndrome, we noted age, height, and weight measurements from the electronic medical record at the time of pseudotumor cerebri syndrome diagnosis (defined as within 3 months of the date of initial diagnosis), when these data were available. Anthropometric Z-scores for body mass index (BMI-Z) were calculated from these data according to the national pediatric dataset published by the US Centers for Disease Control (CDC). Overweight and obese were defined according to the CDC classifications of overweight (BMI-Z ≥1.04 and <1.64) and obese (BMI-Z ≥1.64) in children. BMI-Z scores were used to quantify degree of obesity since, as a continuous measure, these values provide more information than prior categorical designations of normal weight, overweight, and obese. Other assessment parameters collected from the time of initial presentation included sex, population ancestry, CSF opening pressure, Snellen visual acuity, and the presence of various clinical features (headache, visual symptoms, sixth cranial nerve palsy). Study data were collected and managed securely using HIPAA-compliant REDCap (Research Electronic Data Capture) tools hosted at The Children’s Hospital of Philadelphia.
Statistical comparisons between the primary and secondary pseudotumor cerebri syndrome groups used either Mann-Whitney tests or Fisher exact tests, as indicated in the legends in Tables 1 and 2 . Statistical analysis of the secondary pseudotumor cerebri syndrome group used the 1-sample Wilcoxon signed rank test with the theoretical median Z-score equaling zero (ie, in comparison with a theoretical average Z-score of zero) or with the theoretical median Z-score equaling published national averages as referenced in the text. Additionally, a 1-proportion test was performed comparing the frequency of overweight and/or obese children in this study to the null value of the reported national frequency in all children, as referenced in the text. Standard deviations (SD) and interquartile intervals (IQI) were calculated, as appropriate.
| Presumed Secondary Cause of PTCS (n) | Mean Age (y) ± SD | Sex (% Female) | Median BMI-Z [IQI] (n) | Clinical Features | |||
|---|---|---|---|---|---|---|---|
| Sixth Nerve Palsy | Headache (n) | Blurry Vision, Double Vision, or Visual Obscurations (n) | Median CSF Opening Pressure, mm CSF [IQI] (n) | ||||
| Antibiotics (11) | 15.5 ± 2.0 | 82% | 1.58 [1.29-1.87] (9) | 36% | 82% (9) | 82% (9) | 430 [345-550] (11) |
| Chronic kidney disease (3) | 12.8 ± 5.2 | 67% | 1.42 [1.10-1.46] (3) | 0% | 100% (3) | 33% (1) | 360 [343-425] (3) |
| Withdrawal from chronic glucocorticoids (1) | 17.5 | 100% | 1.73 | No | Yes | No | 294 |
| Lithium (1) | 14.0 | 100% | 2.46 | No | No | Yes | 280 |
| Characteristic at Time of Diagnosis of PTCS | Secondary PTCS (All Causes Considered Together) | Primary PTCS | P Value a |
|---|---|---|---|
| Mean age (y) ± SD (n) | 15.0 ± 2.8 (16) | 11.6 ± 4.3 (59) | .003 |
| Sex, % female (n) | 81% (13) | 66% (39) | .36 |
| Population ancestry, self-reported (% for each group) | 31% African-American, 69% white | 22% African-American, 71% white, 7% unknown or not reported | – |
| Median BMI-Z [IQI] | 1.54 [1.18-2.02] | 1.58 [0.76-2.09] | .79 |
| Median height-Z [IQI] | -0.38 [−1.03 to 1.13] | 0.63 [−0.12 to 1.31] | .06 |
| Median weight-Z [IQI] | 1.40 [1.06-2.02] | 1.68 [0.91-2.19] | .65 |
| Sixth nerve palsy (n) | 31% (5) | 34% (20) | 1.00 |
| Median CSF opening pressure, mm CSF [IQI] | 365 [306-535] | 390 [355-475] | .70 |
| Presence of headache (n) | 81% (13) | 75% (44) | .44 |
| Presence of visual symptoms (n) | 69% (11) | 54% (32) | 1.00 |
| Visual acuity: % patients with 20/20 or better in both eyes b (n) | 50% (8) | 34% (19) | .24 |
| Visual acuity: % patients with 20/50 or worse in either eye b (n) | 19% (3) | 9% (5) | .36 |
| Asymptomatic (incidental papilledema found on ophthalmologic examination) (n) | 0% | 12% (7) | .33 |
a P values for age, BMI-Z, height-Z, weight-Z, and CSF opening pressure as calculated from Mann-Whitney test. P values for sex, sixth nerve palsy, headache, visual symptoms, and asymptomatic patients as calculated from Fisher exact test.
b Best-corrected visual acuity when available, otherwise uncorrected visual acuity.
Results
Of 363 patients seen for presumed pseudotumor cerebri syndrome at our hospital, 60 patients had possible secondary pseudotumor cerebri syndrome. As shown in Figure 2 (Top), the secondary associations from most to least common were tetracycline-class antibiotics (52%, n = 31), Down syndrome (12%, n = 7), retinoids and other vitamin A derivatives (10%, n = 6), growth hormone (8%, n = 5), chronic kidney disease (7%, n = 4), withdrawal from chronic glucocorticoids (5%, n = 3), lithium (3%, n = 2), cerebral venous sinus thrombosis (2%, n = 1), and anemia (2%, n = 1).



