Purpose
To critically assess the evidence base regarding outcomes following cataract surgery in uveitic cases.
Design
Systematic evidence-based review and meta-analysis.
Methods
A comprehensive search query was performed on MEDLINE, EMBASE, CINHAL, and CENTRAL databases. Relevant publications were identified by reviewing query results and reference list searches.
Results
A total of 89 articles met eligibility criteria. Among uveitic eyes with quiet or mostly quiet uveitis before cataract surgery, 20/40 visual acuity or better (≥20/40) was achieved in 68% following phacoemulsification, 72% following extracapsular cataract extraction, and 40% following pars plana lensectomy. More eyes undergoing cataract surgery with intraocular lens (IOL) implantation than eyes left aphakic achieved ≥20/40 postoperatively (71% vs 52%). Eyes receiving acrylic IOLs or heparin-surface-modified (HSM) polymethylmethacrylate had better visual outcomes than those receiving non-HSM polymethylmethacrylate or silicone IOLs. Active uveitis at the time of cataract surgery was associated with worse visual outcomes. Compared with other uveitis cases, the proportion achieving 20/40 or better post cataract surgery was better for Fuchs heterochromic cyclitis cases and worse for uveitis related to Behçet disease, Vogt-Koyanagi-Harada disease, or sympathetic ophthalmia, and also posterior uveitis in general.
Conclusion
Cataract surgery in eyes with uveitis resulted in normal range levels of visual acuity in most cases. The review suggests that preoperative control of uveitis, use of an acrylic or HSM IOL, and a diagnosis of Fuchs heterochromic cyclitis were associated with better outcomes. Posterior-involving uveitides tended to do worse, likely because of vision-limiting complications of uveitis. Average results may not be applicable to specific clinical scenarios.
Cataract is a frequent complication of uveitis, a result of both the primary disease process and its treatment with corticosteroids. Many studies have evaluated the outcome of cataract surgery in patients with uveitis, generating varying opinions on the best approach. Surgical approaches that have been tried in uveitis cases include phacoemulsification, extracapsular cataract extraction, and pars plana lensectomy. Some reports suggest that nonuse of an intraocular lens is preferable in uveitis patients generally or in specific subtypes of uveitis (such as juvenile idiopathic arthritis [JIA]–associated uveitis), while others suggest that use of an intraocular lens is preferred, or that specific types of intraocular lenses are superior to other types in the setting of uveitis.
In this comprehensive, systematic review of the literature regarding the outcome of cataract surgery in uveitis cases, we evaluated visual acuity outcomes based on the type of cataract surgery performed, the subtype of uveitis, and the use or nonuse of an intraocular lens. We also compared outcomes among different types of intraocular lens implants, and by the presence or absence of inflammatory activity preoperatively.
Methods
This systematic literature review and meta-analysis was conducted by applying the methods described by the Cochrane Collaboration for systematic reviews of interventions and in concordance with the PRISMA guidelines for systematic reviews and meta-analysis. A systematic search was conducted of 4 databases: MEDLINE (1950-July 2010), EMBASE (1974-July 2010), CINHAL (up to July 2010), and Cochrane Central Register of Controlled Clinical Trials (CENTRAL, up to July 2010). The search strategies used are detailed in the Supplemental Figure (Supplemental Material available at AJO.com ). Limits were placed so as to retrieve only English-language and human studies. Duplicates were removed. Records were screened for relevance, first by comparing retrieved titles and abstracts against the research questions. If considered potentially suitable or if there was uncertainty regarding suitability after reviewing the title and abstract, full text articles were retrieved and reviewed to see whether they met the following eligibility criteria: (1) studies contained patients with uveitis undergoing cataract surgery; and either (2) studies reported visual acuity outcomes as a percent of uveitis patients undergoing cataract surgery with visual acuity outcomes equal to 20/40 or better or (3) if visual results were not reported as described in #2, then data were reported from which this measure could be derived. We excluded studies only available as conference abstracts or unpublished data, as well as those using irrelevant techniques such as intracapsular cataract extraction, very small series of 3 or fewer patients, and non-English-language reports. Also, studies reporting results of combined cataract and glaucoma surgery or combined cataract and fluocinolone acetonide implant placement were excluded. Two authors independently performed these assessments; any inconsistencies were resolved by consensus. Reference lists from all identified studies also were examined for potentially relevant articles, using the same approach.
All eligible studies identified in the systematic review were included in the meta-analysis. For each study, we standardized results by determining the proportion of uveitic eyes with 20/40 or better visual acuity following cataract surgery with 95% confidence intervals. This measure was selected based on its widespread availability in the reports, use of the approach in a previous review of the outcomes of cataract surgery in the general US population, and its relevance in terms of representing a normal or near-normal visual acuity postoperatively. The results reflect the point in time that authors of each report thought reflected the postoperative outcome, typically within 6–12 months following surgery; unfortunately, it was not possible to use exactly the same time point from all reports because of the variable approaches to reporting that were taken. Because individual-level data were not available for meta-analysis, it was not possible to adjust for multiple characteristics simultaneously. Neither could the expected outcome of surgery be assessed; for a substantial minority of cases, a postoperative outcome of 20/40 or better likely was not expected, and visual improvement to a level worse than 20/40 may have represented a high level of improvement of great benefit to that patient.
Results
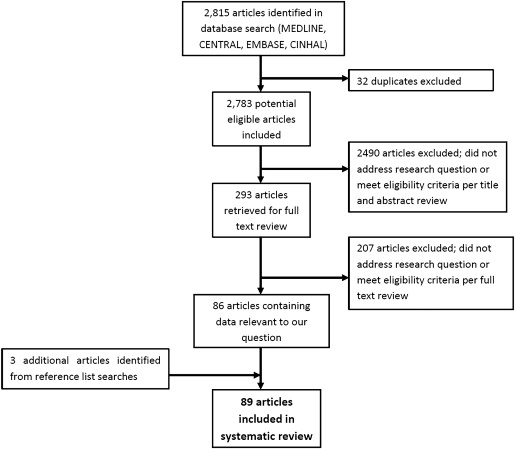
We initially identified 3721 articles from the database searches ( Figure 1 ). English-language and human studies limits reduced the pool to 2815 articles. After removal of duplicate publications, 2783 articles remained. Titles and abstracts were reviewed and 293 articles were retrieved for full text review, of which 86 studies met eligibility criteria; 3 additional articles were added from reference list searches, for a total of 89 articles included in this systematic review. Details regarding each of the 89 articles can be found in the Supplemental Table (Supplemental Material available at AJO.com ). Of the 89 articles, only 2 articles reported a population where many of the patients had active uveitis at the time of cataract surgery, and for 24 additional articles the level of activity prior to cataract surgery was not stated. The remaining 63 articles specifically reported quiet or mostly quiet uveitis at the time of surgery.
Visual Acuity Outcomes by the Type of Cataract Surgery
Studies evaluating visual outcomes following cataract surgery in uveitis cases were grouped by the type of cataract surgery performed ( Figures 2 and 3 ). In order for studies to be included in this section, results of a mixture of uveitis types had to be reported. Studies in which cataract surgery was performed in 1 specific type of uveitis—such as Fuchs heterochromic cyclitis or JIA-associated uveitis—are discussed in the last section on outcomes of cataract surgery by type of uveitis.
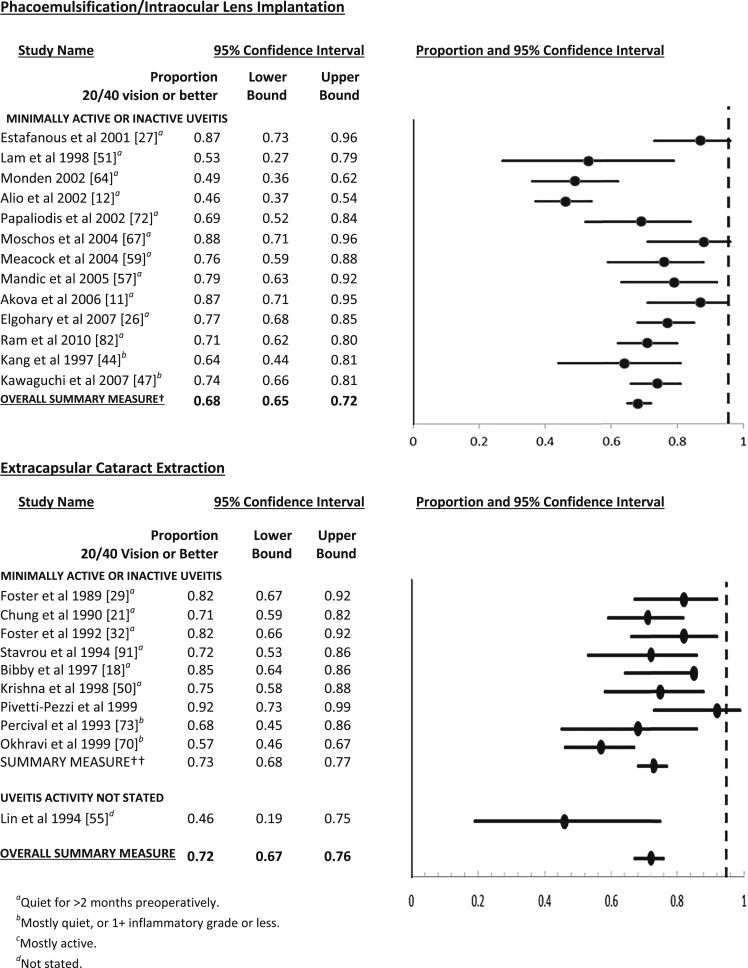
Of the 89 articles, 13 studies evaluated visual outcomes following phacoemulsification with intraocular lens implantation in patients with a mixture of types of uveitis. In each of these reports, the uveitis was quiet for greater than 2 months preoperatively or else mostly quiet, with 1+ anterior chamber cells or less. In aggregate, 68% of uveitis patients achieved 20/40 or better vision (0.68, 95% confidence interval [CI] 0.65–0.72). Of note, 2 studies reported below-average visual outcomes, likely because a disproportionately large number (the majority) of patients in these studies compared to the others had posterior segment pathology such as Behçet disease, sympathetic ophthalmia, syphilitic uveitis, Vogt-Koyanagi-Harada disease (VKH), macular degeneration, macular atrophy, optic atrophy, or glaucomatous optic neuropathy. If these studies are excluded, the aggregate percentage reaching 20/40 or better visual acuity is 76% (0.76, 95% CI 0.72–0.79). It was not possible to sort out the outcomes for patients with and without additional complications of uveitis using meta-analytic techniques with the reported data.
Ten studies evaluated visual outcomes following extracapsular cataract extraction (ECCE) in patients with uveitis. In 9 of these 10 studies, ECCE was performed with intraocular lens implantation. In the remaining study, ECCE with and without intraocular lens implantation was performed. In 1 of the 9 studies, where the level of preoperative uveitis control was not stated, 46% of uveitic eyes had an outcome of 20/40 or better following cataract surgery (0.46, 95% CI 0.19–0.75). Combining data from the remaining 9 studies, in which uveitis was quiet or mostly quiet, 73% of uveitic eyes achieved 20/40 or better vision following ECCE (0.73, 95% CI 0.68–0.77).
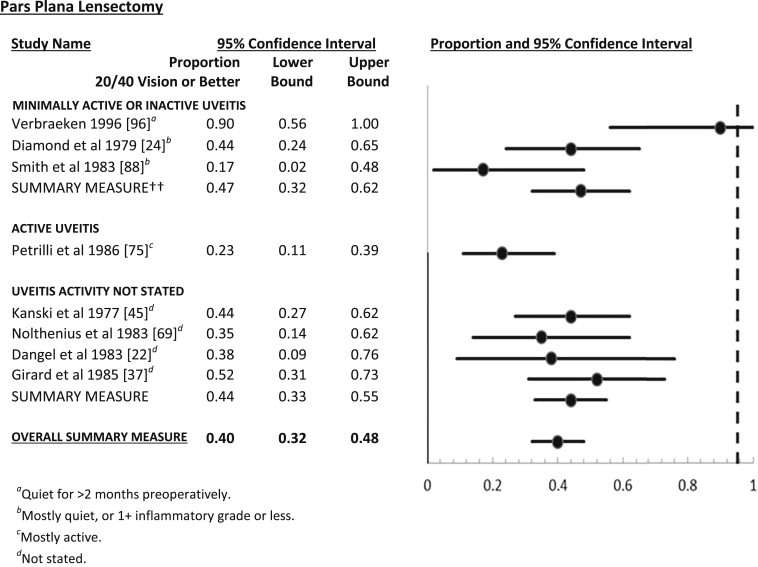
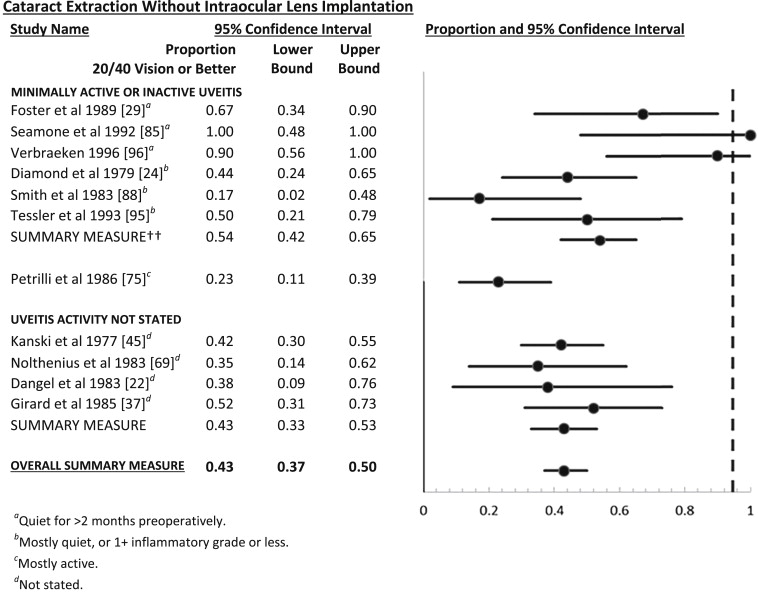
Eight studies evaluated visual acuity outcomes following pars plana lensectomy in uveitis. Preoperative control of uveitis was quiet in 1 of these studies (which was the only study reported since 1990), mostly quiet for 3 studies, mostly active in 1 study, and not stated in 4 studies. Of those 4 studies in which uveitis was quiet or mostly quiet prior to surgery, 20/40 or better visual acuity was achieved in 47% of uveitic eyes following cataract surgery (0.47, 95% CI 0.32–0.62). Among these, the most recent study that had complete preoperative control of uveitis had more favorable results (0.90, 95% CI 0.56–1.00). In cases where uveitis was active at the time of lensectomy, 23% achieved 20/40 or better visual acuity following surgery (0.23, 95% CI 0.11–0.39). Finally, of the 4 studies where activity of uveitis at the time of lensectomy was not reported, 44% achieved 20/40 or better visual acuity postoperatively (0.44, 95% CI 0.33–0.55).
Outcomes of Cataract Surgery With or Without Intraocular Lens Implantation
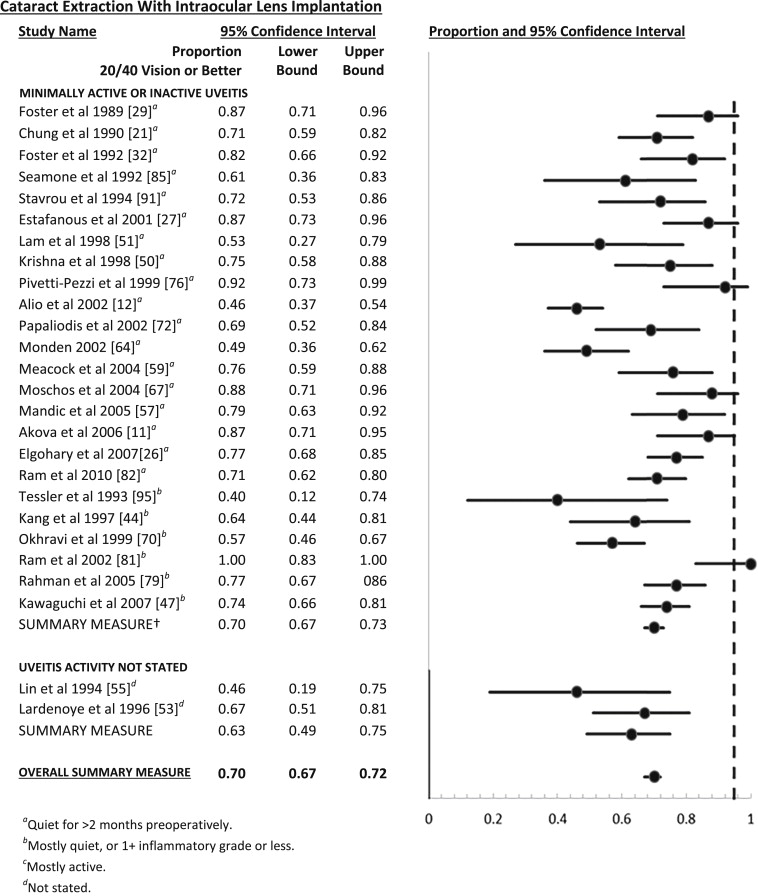
Twenty-six studies evaluated outcomes following cataract surgery with intraocular lens (IOL) implantation in a mixed uveitis population while 11 studies evaluated outcomes following cataract surgery without IOLs ( Figures 4 and 5 ). Studies with intraocular lens implantation used techniques of phacoemulsification or extracapsular cataract extraction, whereas studies without intraocular lens implantation used techniques of extracapsular cataract extraction or pars plana lensectomy. Otherwise, the groups appeared reasonably balanced in terms of type of uveitis and incidence of preoperative posterior pathology. In the 24 studies with quiet or mostly quiet uveitis undergoing cataract surgery with IOL, 70% had 20/40 or better vision postoperatively (95% CI 67%–73%). Including the other 2 studies where preoperative uveitis activity was not explicitly stated, results were similar (70%, 95% CI 67%–72%). In comparison, in the 6 studies evaluating quiet or mostly quiet uveitis undergoing cataract surgery without IOL implantation, only 54% had 20/40 or better vision following surgery (95% CI 42%–65%), and fewer studies where uveitis activity was active or not stated were included (43%, 95% CI 37%–50%). One small trial had randomized 22 cases to use or nonuse of an IOL; there was no statistically significant difference between the groups in this study, which was closed owing to lack of patient interest in enrolling in a study where they could not get an IOL with surgery. Cases where uveitis was active at the time of cataract surgery and no IOL was placed had poor visual outcomes, with 23% achieving 20/40 or better vision (95% CI 11%–39%). On average, uveitic eyes undergoing cataract surgery with IOL implantation had significantly better visual outcomes than eyes undergoing cataract surgery without IOL implantation.
Outcomes of Cataract Surgery With Alternative Intraocular Lens Types
Seven studies evaluated visual outcomes following cataract surgery with acrylic IOL implantation ( Figure 6 ). In all studies, uveitis was quiet or mostly quiet for greater than 2 months prior to surgery. Overall, 69% of uveitic eyes had 20/40 or better vision following cataract surgery with acrylic IOL implantation (95% CI 63%–75%), similar to results for overall IOL surgery.
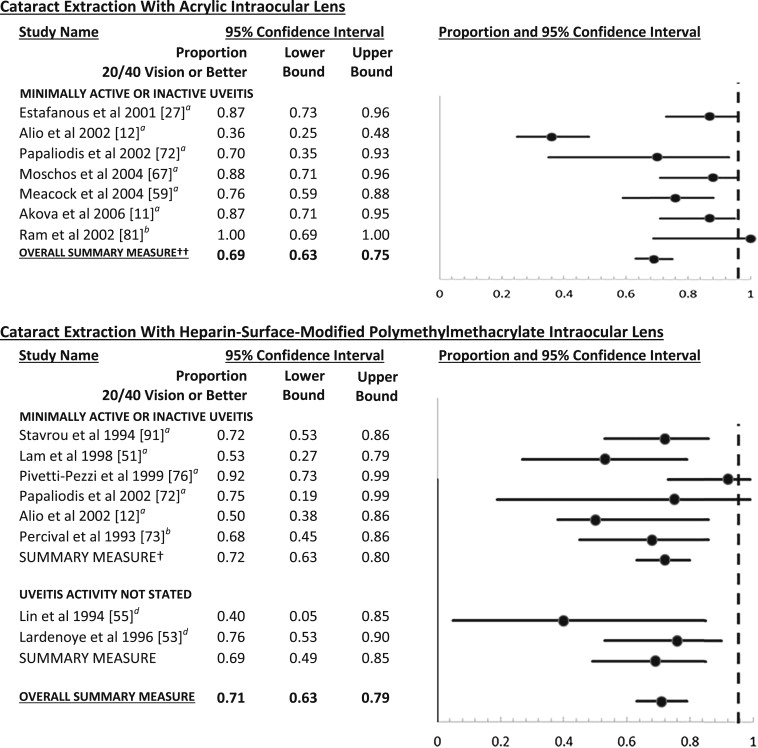
Eight articles evaluated cataract surgery with heparin-surface-modified polymethylmethacrylate IOLs in patients with uveitis. In patients with quiet or mostly quiet uveitis, 72% achieved visual acuity of 20/40 or better following cataract surgery with heparin-surface-modified polymethylmethacrylate IOLs (95% CI 63%–80%), similar to the results with acrylic lenses and better than non–heparin-surface-modified polymethylmethacrylate IOLs (see below). Inclusion of the 2 studies where the level of preoperative uveitis activity was not specified had little impact on the proportion with postoperative visual acuity of 20/40 or better (0.71, 95% CI 0.63–0.79).
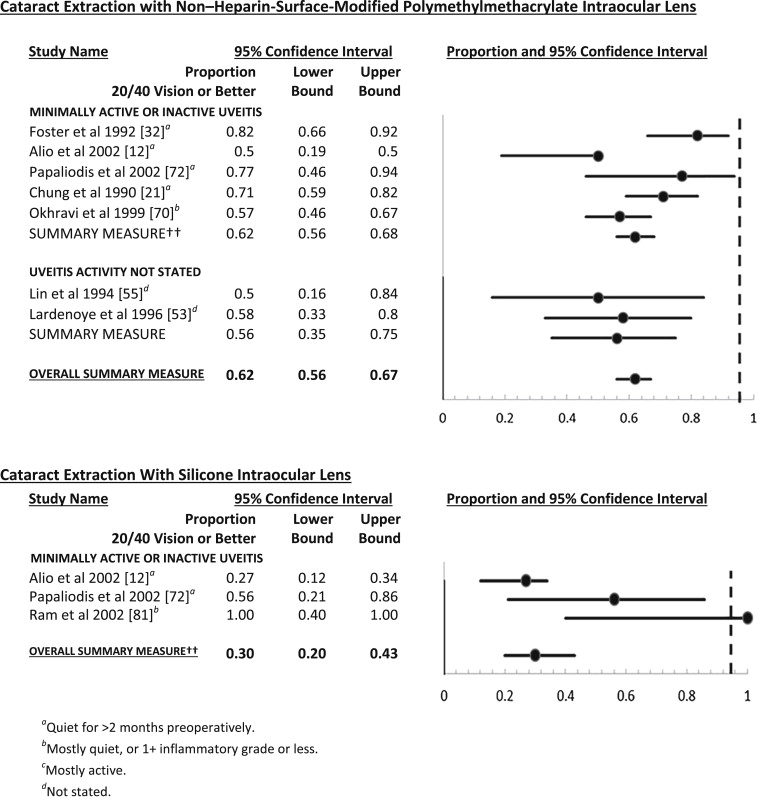
Seven studies evaluated cataract surgery outcomes with non–heparin-surface-modified polymethylmethacrylate IOLs in uveitis cases. Uveitis was quiet in 5 studies and activity status was not stated in the remaining 2 studies (results were similar across these groups, so they are pooled). Overall, 62% of uveitic eyes had 20/40 or better vision following cataract surgery with non–heparin-surface-modified polymethylmethacrylate IOLs (0.62, 95% CI 0.56–0.67), fewer than with acrylic or heparin-surface-modified polymethylmethacrylate IOLs.
Three of 89 articles evaluated outcomes following cataract surgery with silicone IOL implantation in patients with uveitis. In all of these studies, uveitis was quiet or mostly quiet. Overall, 30% uveitic eyes had 20/40 or better vision following cataract surgery with silicone IOL implantation (95% CI 20%–43%), fewer than with other types of intraocular lenses.
In summary, these results suggest similar visual outcomes in cases receiving acrylic or heparin-surface-modified polymethylmethacrylate IOLs, with somewhat less favorable results using non–heparin-surface-modified polymethylmethacrylate IOLs. Silicone IOLs had the worst visual results, on average.
Outcomes of Cataract Surgery by Type of Uveitis
Fuchs heterochromic cyclitis
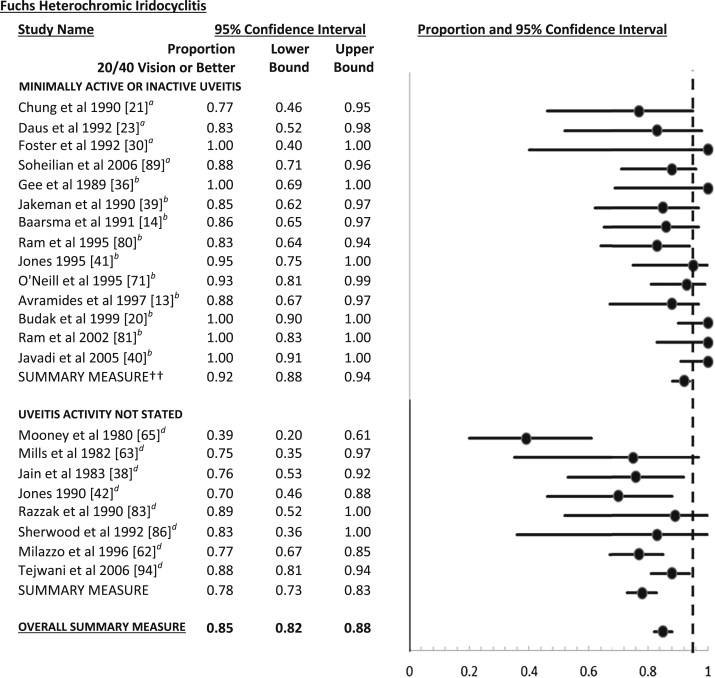
Twenty-two studies evaluated cataract surgery outcomes in patients with Fuchs heterochromic cyclitis ( Figure 7 ). Ninety-two percent of eyes in which uveitis was quiet or mostly quiet achieved 20/40 or better vision following cataract surgery (95% CI 88%–94%). Eyes in which preoperative uveitis control was not stated achieved 20/40 or better vision in 78% of cases (95% CI 73%–83%). Overall, 85% (95% CI 82%–88%) of Fuchs heterochromic cyclitis cases achieved 20/40 or better visual acuity after cataract surgery, significantly better than the average of a mixed population of uveitis cases undergoing phacoemulsification or ECCE.
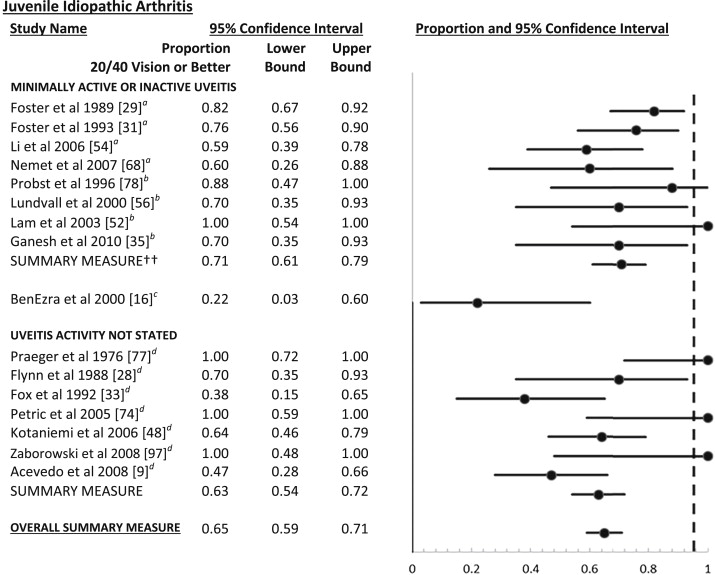
Juvenile idiopathic arthritis
Sixteen articles evaluated cataract surgery outcomes in cases of uveitis associated with JIA ( Figure 7 ). Among uveitic eyes in which intraocular inflammation was quiet or mostly quiet prior to cataract surgery, 71% (95% CI 61%–79%) gained 20/40 visual acuity or better following cataract surgery. A study in which patients with mostly active JIA-associated uveitis underwent cataract surgery reported significantly worse visual outcomes, with 22% attaining 20/40 or better vision following cataract surgery (95% CI 3%–60%). Visual acuity outcomes were intermediate among eyes with JIA-associated uveitis in which preoperative uveitic activity was not specified (0.63, 95% CI 0.54–0.72). Overall, 65% of eyes with JIA-associated uveitis had visual acuity outcomes of 20/40 or better following cataract surgery (0.65, 95% CI 0.59–0.72). Postoperative visual results of these cases were not substantially different from the results of a mixed population of uveitis cases in which patients underwent phacoemulsification or ECCE.
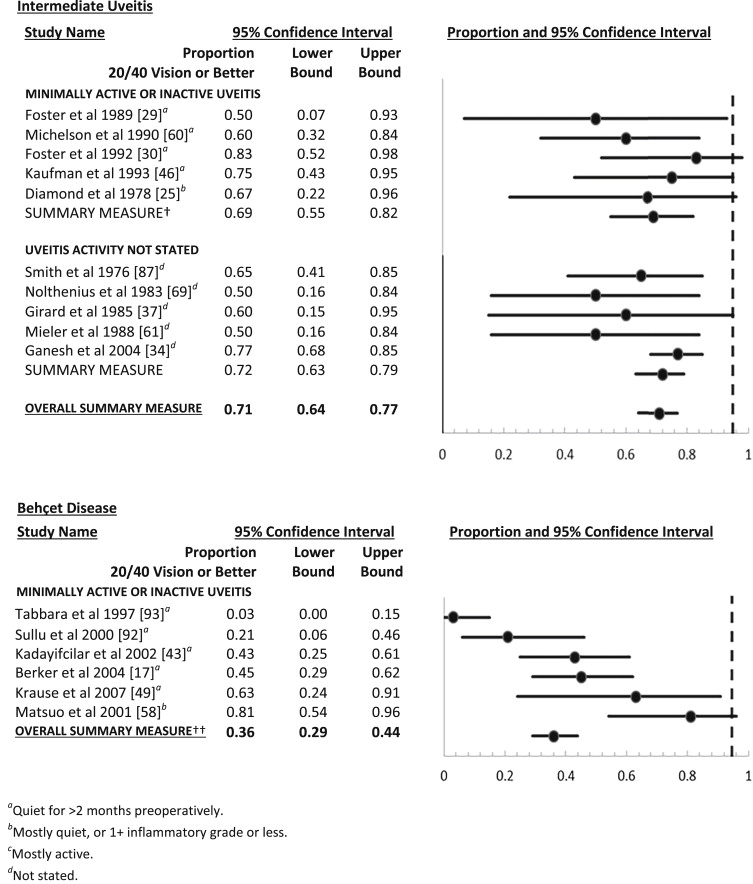
Intermediate uveitis
Ten studies evaluated cataract surgery outcomes in patients with intermediate uveitis ( Figure 7 ). Sixty-nine percent of eyes with quiet or mostly quiet eyes preoperatively had visual acuity outcomes of 20/40 or better (0.69, 95% CI 0.55–0.82), similar to the pooled result for all studies in which 71% of eyes with intermediate uveitis achieve 20/40 or better visual acuity following cataract surgery (0.71, 95% CI 0.62–0.77). No reports were available regarding outcomes in a mostly active cohort. Postoperative visual results of these cases were not substantially different from the results of a mixed population of uveitis cases undergoing phacoemulsification or ECCE.
Behçet disease
Six studies evaluated cataract surgery outcomes in patients with uveitis related to Behçet disease ( Figure 7 ). In 5 of these studies, uveitis had been completely quiet for greater than 2 months prior to surgery and in 1 study uveitis was mostly quiet prior to surgery. Overall, 36% of eyes with uveitis related to Behçet disease had a visual acuity of 20/40 or better following cataract surgery (0.36, 95% CI 0.29–0.44), significantly worse than the outcomes of mixed uveitis populations undergoing phacoemulsification or extracapsular cataract extraction.
Other
Very few studies were identified reporting cataract surgery outcomes in patients with posterior uveitis, VKH, sympathetic ophthalmia, and sarcoidosis ( Supplemental Table ), and none met eligibility criteria regarding other ocular inflammatory conditions. Two studies reported visual outcomes following cataract surgery in patients with various kinds of posterior uveitis. In these studies, posterior uveitis was mostly quiet prior to cataract surgery. Pooling their results, 46% of uveitic eyes gained a visual acuity of 20/40 or better following cataract surgery (0.46, 95% CI 0.35–0.59). Similarly, in cases with VKH, 49% of VKH eyes had 20/40 or better visual acuity following cataract surgery (0.49, 95% CI 0.34–0.65), based on the combination of 2 series, 1 in which the 19 cases were quiet for greater than 2 months prior to surgery and 1 in which preoperative control of uveitis was not mentioned (20 cases). In 1 report regarding cases of sympathetic ophthalmia, in which the level of preoperative control of uveitis was not stated, 40% of cases had a visual acuity of 20/40 or better following cataract surgery (95% CI 4%–78%). In general, cohorts with uveitis involving the choroid and/or retina—which likely have more preexisting vision-limiting macular pathology than in cases of anterior or intermediate uveitis—appeared to have worse visual outcomes than mixed cohorts also including anterior and intermediate uveitis cases.
Results
We initially identified 3721 articles from the database searches ( Figure 1 ). English-language and human studies limits reduced the pool to 2815 articles. After removal of duplicate publications, 2783 articles remained. Titles and abstracts were reviewed and 293 articles were retrieved for full text review, of which 86 studies met eligibility criteria; 3 additional articles were added from reference list searches, for a total of 89 articles included in this systematic review. Details regarding each of the 89 articles can be found in the Supplemental Table (Supplemental Material available at AJO.com ). Of the 89 articles, only 2 articles reported a population where many of the patients had active uveitis at the time of cataract surgery, and for 24 additional articles the level of activity prior to cataract surgery was not stated. The remaining 63 articles specifically reported quiet or mostly quiet uveitis at the time of surgery.
Visual Acuity Outcomes by the Type of Cataract Surgery
Studies evaluating visual outcomes following cataract surgery in uveitis cases were grouped by the type of cataract surgery performed ( Figures 2 and 3 ). In order for studies to be included in this section, results of a mixture of uveitis types had to be reported. Studies in which cataract surgery was performed in 1 specific type of uveitis—such as Fuchs heterochromic cyclitis or JIA-associated uveitis—are discussed in the last section on outcomes of cataract surgery by type of uveitis.
Of the 89 articles, 13 studies evaluated visual outcomes following phacoemulsification with intraocular lens implantation in patients with a mixture of types of uveitis. In each of these reports, the uveitis was quiet for greater than 2 months preoperatively or else mostly quiet, with 1+ anterior chamber cells or less. In aggregate, 68% of uveitis patients achieved 20/40 or better vision (0.68, 95% confidence interval [CI] 0.65–0.72). Of note, 2 studies reported below-average visual outcomes, likely because a disproportionately large number (the majority) of patients in these studies compared to the others had posterior segment pathology such as Behçet disease, sympathetic ophthalmia, syphilitic uveitis, Vogt-Koyanagi-Harada disease (VKH), macular degeneration, macular atrophy, optic atrophy, or glaucomatous optic neuropathy. If these studies are excluded, the aggregate percentage reaching 20/40 or better visual acuity is 76% (0.76, 95% CI 0.72–0.79). It was not possible to sort out the outcomes for patients with and without additional complications of uveitis using meta-analytic techniques with the reported data.
Ten studies evaluated visual outcomes following extracapsular cataract extraction (ECCE) in patients with uveitis. In 9 of these 10 studies, ECCE was performed with intraocular lens implantation. In the remaining study, ECCE with and without intraocular lens implantation was performed. In 1 of the 9 studies, where the level of preoperative uveitis control was not stated, 46% of uveitic eyes had an outcome of 20/40 or better following cataract surgery (0.46, 95% CI 0.19–0.75). Combining data from the remaining 9 studies, in which uveitis was quiet or mostly quiet, 73% of uveitic eyes achieved 20/40 or better vision following ECCE (0.73, 95% CI 0.68–0.77).
Eight studies evaluated visual acuity outcomes following pars plana lensectomy in uveitis. Preoperative control of uveitis was quiet in 1 of these studies (which was the only study reported since 1990), mostly quiet for 3 studies, mostly active in 1 study, and not stated in 4 studies. Of those 4 studies in which uveitis was quiet or mostly quiet prior to surgery, 20/40 or better visual acuity was achieved in 47% of uveitic eyes following cataract surgery (0.47, 95% CI 0.32–0.62). Among these, the most recent study that had complete preoperative control of uveitis had more favorable results (0.90, 95% CI 0.56–1.00). In cases where uveitis was active at the time of lensectomy, 23% achieved 20/40 or better visual acuity following surgery (0.23, 95% CI 0.11–0.39). Finally, of the 4 studies where activity of uveitis at the time of lensectomy was not reported, 44% achieved 20/40 or better visual acuity postoperatively (0.44, 95% CI 0.33–0.55).
Outcomes of Cataract Surgery With or Without Intraocular Lens Implantation
Twenty-six studies evaluated outcomes following cataract surgery with intraocular lens (IOL) implantation in a mixed uveitis population while 11 studies evaluated outcomes following cataract surgery without IOLs ( Figures 4 and 5 ). Studies with intraocular lens implantation used techniques of phacoemulsification or extracapsular cataract extraction, whereas studies without intraocular lens implantation used techniques of extracapsular cataract extraction or pars plana lensectomy. Otherwise, the groups appeared reasonably balanced in terms of type of uveitis and incidence of preoperative posterior pathology. In the 24 studies with quiet or mostly quiet uveitis undergoing cataract surgery with IOL, 70% had 20/40 or better vision postoperatively (95% CI 67%–73%). Including the other 2 studies where preoperative uveitis activity was not explicitly stated, results were similar (70%, 95% CI 67%–72%). In comparison, in the 6 studies evaluating quiet or mostly quiet uveitis undergoing cataract surgery without IOL implantation, only 54% had 20/40 or better vision following surgery (95% CI 42%–65%), and fewer studies where uveitis activity was active or not stated were included (43%, 95% CI 37%–50%). One small trial had randomized 22 cases to use or nonuse of an IOL; there was no statistically significant difference between the groups in this study, which was closed owing to lack of patient interest in enrolling in a study where they could not get an IOL with surgery. Cases where uveitis was active at the time of cataract surgery and no IOL was placed had poor visual outcomes, with 23% achieving 20/40 or better vision (95% CI 11%–39%). On average, uveitic eyes undergoing cataract surgery with IOL implantation had significantly better visual outcomes than eyes undergoing cataract surgery without IOL implantation.
Outcomes of Cataract Surgery With Alternative Intraocular Lens Types
Seven studies evaluated visual outcomes following cataract surgery with acrylic IOL implantation ( Figure 6 ). In all studies, uveitis was quiet or mostly quiet for greater than 2 months prior to surgery. Overall, 69% of uveitic eyes had 20/40 or better vision following cataract surgery with acrylic IOL implantation (95% CI 63%–75%), similar to results for overall IOL surgery.
Eight articles evaluated cataract surgery with heparin-surface-modified polymethylmethacrylate IOLs in patients with uveitis. In patients with quiet or mostly quiet uveitis, 72% achieved visual acuity of 20/40 or better following cataract surgery with heparin-surface-modified polymethylmethacrylate IOLs (95% CI 63%–80%), similar to the results with acrylic lenses and better than non–heparin-surface-modified polymethylmethacrylate IOLs (see below). Inclusion of the 2 studies where the level of preoperative uveitis activity was not specified had little impact on the proportion with postoperative visual acuity of 20/40 or better (0.71, 95% CI 0.63–0.79).
Seven studies evaluated cataract surgery outcomes with non–heparin-surface-modified polymethylmethacrylate IOLs in uveitis cases. Uveitis was quiet in 5 studies and activity status was not stated in the remaining 2 studies (results were similar across these groups, so they are pooled). Overall, 62% of uveitic eyes had 20/40 or better vision following cataract surgery with non–heparin-surface-modified polymethylmethacrylate IOLs (0.62, 95% CI 0.56–0.67), fewer than with acrylic or heparin-surface-modified polymethylmethacrylate IOLs.
Three of 89 articles evaluated outcomes following cataract surgery with silicone IOL implantation in patients with uveitis. In all of these studies, uveitis was quiet or mostly quiet. Overall, 30% uveitic eyes had 20/40 or better vision following cataract surgery with silicone IOL implantation (95% CI 20%–43%), fewer than with other types of intraocular lenses.
In summary, these results suggest similar visual outcomes in cases receiving acrylic or heparin-surface-modified polymethylmethacrylate IOLs, with somewhat less favorable results using non–heparin-surface-modified polymethylmethacrylate IOLs. Silicone IOLs had the worst visual results, on average.
Outcomes of Cataract Surgery by Type of Uveitis
Fuchs heterochromic cyclitis
Twenty-two studies evaluated cataract surgery outcomes in patients with Fuchs heterochromic cyclitis ( Figure 7 ). Ninety-two percent of eyes in which uveitis was quiet or mostly quiet achieved 20/40 or better vision following cataract surgery (95% CI 88%–94%). Eyes in which preoperative uveitis control was not stated achieved 20/40 or better vision in 78% of cases (95% CI 73%–83%). Overall, 85% (95% CI 82%–88%) of Fuchs heterochromic cyclitis cases achieved 20/40 or better visual acuity after cataract surgery, significantly better than the average of a mixed population of uveitis cases undergoing phacoemulsification or ECCE.
Juvenile idiopathic arthritis
Sixteen articles evaluated cataract surgery outcomes in cases of uveitis associated with JIA ( Figure 7 ). Among uveitic eyes in which intraocular inflammation was quiet or mostly quiet prior to cataract surgery, 71% (95% CI 61%–79%) gained 20/40 visual acuity or better following cataract surgery. A study in which patients with mostly active JIA-associated uveitis underwent cataract surgery reported significantly worse visual outcomes, with 22% attaining 20/40 or better vision following cataract surgery (95% CI 3%–60%). Visual acuity outcomes were intermediate among eyes with JIA-associated uveitis in which preoperative uveitic activity was not specified (0.63, 95% CI 0.54–0.72). Overall, 65% of eyes with JIA-associated uveitis had visual acuity outcomes of 20/40 or better following cataract surgery (0.65, 95% CI 0.59–0.72). Postoperative visual results of these cases were not substantially different from the results of a mixed population of uveitis cases in which patients underwent phacoemulsification or ECCE.
Intermediate uveitis
Ten studies evaluated cataract surgery outcomes in patients with intermediate uveitis ( Figure 7 ). Sixty-nine percent of eyes with quiet or mostly quiet eyes preoperatively had visual acuity outcomes of 20/40 or better (0.69, 95% CI 0.55–0.82), similar to the pooled result for all studies in which 71% of eyes with intermediate uveitis achieve 20/40 or better visual acuity following cataract surgery (0.71, 95% CI 0.62–0.77). No reports were available regarding outcomes in a mostly active cohort. Postoperative visual results of these cases were not substantially different from the results of a mixed population of uveitis cases undergoing phacoemulsification or ECCE.
Behçet disease
Six studies evaluated cataract surgery outcomes in patients with uveitis related to Behçet disease ( Figure 7 ). In 5 of these studies, uveitis had been completely quiet for greater than 2 months prior to surgery and in 1 study uveitis was mostly quiet prior to surgery. Overall, 36% of eyes with uveitis related to Behçet disease had a visual acuity of 20/40 or better following cataract surgery (0.36, 95% CI 0.29–0.44), significantly worse than the outcomes of mixed uveitis populations undergoing phacoemulsification or extracapsular cataract extraction.
Other
Very few studies were identified reporting cataract surgery outcomes in patients with posterior uveitis, VKH, sympathetic ophthalmia, and sarcoidosis ( Supplemental Table ), and none met eligibility criteria regarding other ocular inflammatory conditions. Two studies reported visual outcomes following cataract surgery in patients with various kinds of posterior uveitis. In these studies, posterior uveitis was mostly quiet prior to cataract surgery. Pooling their results, 46% of uveitic eyes gained a visual acuity of 20/40 or better following cataract surgery (0.46, 95% CI 0.35–0.59). Similarly, in cases with VKH, 49% of VKH eyes had 20/40 or better visual acuity following cataract surgery (0.49, 95% CI 0.34–0.65), based on the combination of 2 series, 1 in which the 19 cases were quiet for greater than 2 months prior to surgery and 1 in which preoperative control of uveitis was not mentioned (20 cases). In 1 report regarding cases of sympathetic ophthalmia, in which the level of preoperative control of uveitis was not stated, 40% of cases had a visual acuity of 20/40 or better following cataract surgery (95% CI 4%–78%). In general, cohorts with uveitis involving the choroid and/or retina—which likely have more preexisting vision-limiting macular pathology than in cases of anterior or intermediate uveitis—appeared to have worse visual outcomes than mixed cohorts also including anterior and intermediate uveitis cases.
Discussion
Our systematic review of the literature regarding visual outcomes following cataract surgery in uveitis cases offers important insights into the optimal management of these patients. Visual outcomes following cataract surgery in uveitis cases were not as good as in patients with nonuveitic age-related cataracts undergoing cataract surgery, with the possible exception of Fuchs heterochromic cyclitis cases free of inflammation. In this systematic review, 70% of uveitic eyes undergoing phacoemulsification or extracapsular cataract extraction had visual outcomes of 20/40 or better. In contrast, Powe and associates systematically reviewed the evidence base of outcomes for cataract surgery in age-related cataracts and found that 96% had visual outcomes of 20/40 or better following phacoemulsification or extracapsular cataract extraction. Vision-limiting pathology related to preexisting uveitic complications is likely the major factor reducing the proportion with 20/40 or better visual acuity postoperatively, but other factors, including exaggerated postoperative inflammation, may also play a role in limiting visual outcomes. The latter is supported by our results indicating that patients with active inflammation at the time of surgery have poorer visual outcomes, reinforcing the importance of controlling inflammation prior to cataract surgery, preferably for 2 months or more. In addition, studies suggest that uveitic eyes are at increased risk for developing postoperative complications such as posterior capsular opacification, epiretinal membranes, cystoid macular edema, and pupillary membranes.
It is important to note that subjects with uveitis who are known not to have vision-limiting uveitic complications likely have a considerably better prognosis, and that subjects with vision-limiting uveitic complications still may obtain very clinically important improvement as a result of cataract surgery. Current National Quality Forum metrics for cataract surgery are based on 20/40 vision or better at 90 days following surgery. The majority of studies in our systematic review evaluated outcomes at greater than 6 months following surgery. Patients expected to obtain substantial improvement, but not to some prespecified level such as 20/40 or better, should not be denied access to cataract surgery on the basis of limited expectations even in resource-limited settings, because lesser levels of improvement still can be life-transforming. Governmental and nongovernmental cataract surgery outcome monitoring systems should avoid approaches that incentivize denial of surgery to such patients.
With regard to visual outcomes following cataract surgery in uveitis cases by the type of cataract surgery performed, the review indicated that phacoemulsification and ECCE surgeries had similar visual outcomes, but that pars plana lensectomy obtained a visual acuity of 20/40 or better about half as often. Regarding the comparison between phacoemulsification and ECCE, most phacoemulsification studies had minimal exclusion criteria, whereas ECCE studies had more exclusion criteria, favoring better visual outcomes. For example, the phacoemulsification studies performed by Alio and associates and Monden included patients with optic atrophy and macular degeneration, whereas several of the ECCE studies excluded patients with juvenile uveitis, diffuse uveitis, VKH, sympathetic ophthalmia, and Behçet disease. In addition, there were more cases with posterior-involving uveitis in the phacoemulsification studies than in the ECCE studies. Thus, the characteristics of cases in the phacoemulsification and ECCE studies would be expected to bias toward better results with ECCE, yet results of the 2 approaches nevertheless were similar, suggesting that phacoemulsification probably is not inferior to ECCE. Visual outcomes following pars plana lensectomy were much worse compared to outcomes following phacoemulsification or ECCE. Although this may reflect a greater prevalence of preexisting vision-limiting pathology in patients who undergo pars plana lensectomy, approximately 30% of patients in the lensectomy group had posterior uveitis, which is similar to the amount in the ECCE group and less than that in the phacoemulsification group. Pars plana lensectomy patients also were more likely to be left aphakic, which was associated with worse visual outcome (see below). Although a head-to-head comparison would be required to evaluate properly whether pars plana lensectomy has results inferior to anterior segment approaches, the available evidence suggests that an anterior approach may be preferable for cataract surgery when feasible, for an average case. Only 1 report regarding pars plana lensectomy since 1990 was available, which might have led to an underestimate of success with this approach when more modern technology is used, or alternatively may reflect that this approach is no longer widely used by many clinicians—perhaps because of increased difficulty with IOL placement using a posterior approach. Anterior approaches generally mean less surgical time and intraocular manipulation. Anterior approaches require a small-incision corneal wound, use a phacoemulsification handpiece, and generally include intraocular lens placement, whereas posterior approaches generally mean removal of the entire vitreous and parts of the lens capsule, and may not be accompanied by placement of an intraocular lens.
Fuchs heterochromic cyclitis had better outcomes following cataract surgery than other uveitic entities. In our systematic review, among eyes with Fuchs cyclitis that were quiet for greater than 2 months prior to surgery or mostly quiet preoperatively, 92% had 20/40 or better visual acuity outcomes. This result was close to the visual outcome achieved following phacoemulsification or ECCE for nonuveitic age-related cataract (96%). Fuchs cyclitis is a uveitic syndrome in which posterior synechiae and posterior segment complications of uveitis usually do not occur, which may have contributed to better outcomes on the basis of less preexisting vision-limiting pathology and/or less postoperative inflammation than with other types of uveitis.
Based on the available reports, cataract surgery in JIA-associated uveitis had a similar proportion of cases in which patients gained postoperative visual acuity of 20/40 or better to a mixed population of uveitis cases. The evidence base clearly indicates, as expected, that patients in whom JIA-associated uveitis is quiet preoperatively do better than those with active uveitis at the time of surgery. We hope to report on use of IOL with cataract surgery in JIA-associated uveitis in a separate publication. Our analysis reflects relatively early postoperative outcomes and does not address whether long-term outcomes differ with JIA-associated uveitis vs a mixed group of uveitis cases. Research on the optimal surgical approach for JIA-associated uveitis cases with cataract is needed but is difficult logistically because the disease is rare.
In our systematic review, visual outcomes following cataract surgery in intermediate uveitis were similar to those in a mixed population of uveitis cases, whereas results in cases of Behçet disease, Vogt-Koyanagi-Harada disease, sympathetic ophthalmia, and posterior uveitis in general were substantially worse. Patients with posterior uveitis likely have poorer visual results than those with other uveitic entities because chorioretinal injury from the disease limits visual potential following cataract surgery. As mentioned previously, such eyes may nevertheless have a high degree of visual improvement with cataract surgery, even if not to 20/40 or better.
Regarding outcomes of cataract surgery with or without IOL implantation in uveitic eyes, we found that uveitic eyes undergoing cataract surgery with IOL implantation (70%) did better than uveitic eyes undergoing cataract surgery without IOL implantation (43%). Uveitic eyes with quiet or mostly quiet uveitis preoperatively undergoing cataract surgery without IOL implantation (54%) did better than uveitic eyes with active uveitis undergoing cataract surgery without IOL implantation (23%), but neither had as good a visual outcome as uveitic eyes undergoing cataract surgery with IOL implantation, on average . Again, the meta-analytic approach taken does not allow adjustment for case mix. However, given that in general the papers reported the results of the prevailing approach at the time at the reporting center, and also that a meta-analytic comparison of cases with the same level of control of inflammation was conducted, the large difference in results suggests that use of an IOL is to be preferred for the average case. We were unable to evaluate specific circumstances wherein IOL use would be contraindicated, and such may well exist. Interestingly, uveitic eyes undergoing cataract surgery with acrylic IOLs and heparin-surface-modified polymethylmethacrylate IOLs had slightly better visual outcomes, on average , than patients with non–heparin-surface-modified polymethylmethacrylate IOLs, providing modest evidence suggestive of an advantage for these materials. Patients receiving silicone IOLs obtained postoperative visual acuity of 20/40 or better less than half as often as with the other 3 kinds of IOLs, suggesting a possible disadvantage of this IOL material in the uveitis setting. Uveitic eyes with heparin-surface-modified polymethylmethacrylate and acrylic IOLs may do better than non–heparin-surface-modified polymethylmethacrylate and silicone IOLs because of increased biocompatibility of the former IOLs. Postoperative breakdown of the blood–aqueous barrier leads to cellular and protein adhesion to the surface of the implant and to epithelial cell proliferation. Studies have shown that polymethylmethacrylate IOLs induce complement, the coagulation cascade, and a foreign body response. Modification of the polymethylmethacrylate IOL with heparin surface coating provides a more hydrophilic surface, reducing adhesions such as bacteria, fibrin, and white blood cells. Studies also have shown lower laser flare-cell levels in cases following placement of heparin-surface-modified polymethylmethacrylate IOLs than with non–heparin-surface-modified polymethylmethacrylate IOLs and with acrylic IOLs than with silicone IOLs. Our results did not suggest an important degree of difference between acrylic IOLs, which are widely available and foldable, and heparin-surface-modified polymethylmethacrylate IOLs, which are not as widely available and require a larger incision.
This systematic review has several limitations. Because individual-level data were not available, it was not possible to adjust for the various potentially confounding attributes simultaneously in order to account for prognostic characteristics that may have differed substantially between groups, with the result that confounding may have contributed to some of the patterns observed. In addition, results are observational—with the exception of 1 small randomized trial —and in most cases do not reflect a head-to-head comparison between alternative groups, which might have led to indication-for-treatment biases. Thus, decisions to use or not to use a surgical approach such as pars plana lensectomy or nonplacement of an IOL may have been the result of—rather than the cause of—a poor preoperative prognosis. Furthermore, cohort effects may be present, in that older reports may reflect less ideal practices than were followed in more recent times, in ways that cannot be captured by taking into account just uveitis activity as reported in the publications. For example, information regarding pars plana lensectomy or cataract surgery without IOL implantation tends to derive from older reports, whereas results following phacoemulsification with IOL reflect newer practices. Nevertheless, many of the differences observed are large, making it still likely that—for instance—anterior approaches and use of an IOL tend to have more favorable results on average. This being said, some patients may not be average and may do better with different approaches, and some surgeons may be particularly effective with a different-than-average approach. Another well-recognized limitation of meta-analyses is publication bias—that the likelihood of publication of a study varies based on the results of the study. For example, results that were similar to those of previous publications or that were not statistically significant may have been less likely to be published, and thus may not have been included in this meta-analysis. Another limitation of this study is that the makeup of mixed groups of uveitis patients used as a comparison group may have been different between studies. This concern was discussed above in the considerations for which it was most relevant. In addition, the results reported were not at a certain point in time across all publications, and in general do not reflect long-term outcomes following cataract surgery, which might or might not differ considerably with one technique vs another. Thus, it is conceivable that results even could be better in the long run with the approach or subgroup that is worse in the short run. Finally, in using a common visual acuity metric as the basis for comparison, we evaluated the chance of gaining a near-normal visual acuity outcome rather than the chance of a substantial visual improvement, which could not be evaluated in most of the reports of interest but may be very important to patients. Unfortunately, head-to-head randomized comparisons, which would be the ideal approach to evaluate these important questions, were generally not available.
The main strengths of the study are that it systematically synthesizes the available evidence regarding an important and common clinical intervention, and that it points out areas of need for additional studies.
In conclusion, cataract surgery in eyes with uveitis can result in normal or near-normal visual acuity in the majority of cases, at least in the short run, albeit not as frequently as for nonuveitic age-related cataracts. Despite considerable uncertainty as a result of the numerous limitations we have in trying to synthesize the available evidence, it seems warranted to quiet the eye for at least 2 months prior to surgery and to use an anterior approach to cataract surgery in most cases, and to insert an acrylic or heparin-surface-modified polymethylmethacrylate IOL when there is not a specific indication to do otherwise. Further research is needed to increase the level of confidence on which we can make decisions regarding the surgical management of cataract in uveitic eyes, and particularly to develop evidence specifically pertinent to the individual clinical entities making up this heterogeneous group of diseases.
All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest and have made the following disclosure(s): Sonia Mehta (none); Melody M. Linton (none); John H. Kempen: (consultant) Allergan; (consultant) Alcon; (consultant) Can-Fite Biopharma; (consultant) Clearside Biomedical; (consultant) Lux Biosciences; (consultant) Xoma; (grant funding) National Eye Institute; (grant funding) Food and Drug Administration; (grant funding) EyeGate Pharma; (grant funding) Lions Club International Foundation. This study was supported in part by an unrestricted departmental grant from the Research to Prevent Blindness , New York, NY, USA and the Paul and Evanina Mackall Foundation , New York, NY, USA. Contributions of authors: design and conduct of the study (S.M., J.H.K.); collection, management, analysis, and interpretation of the data (all authors); preparation, review, or approval of the manuscript (all authors).
Appendix



