Purpose
To evaluate proton beam therapy (PBT) as a means to preserve the eye and spare some vision while not deteriorating survival in patients with large choroidal melanomas.
Design
This is a retrospective, consecutive cohort study of patients with T3-4 choroidal melanomas according to the 7th edition of the American Joint Cancer Classification treated with PBT over a 24-year period.
Results
A total of 492 patients were included. Mean (range) tumor thickness and diameter were 8.77 (2–15) mm and 14.91 (7–24.1) mm, respectively. Mean macular and optic disc distance were 4.56 (0–19.9) mm and 4.59 (0–22.1) mm, respectively. Mean follow-up was 61.9 months. Rates of neovascular glaucoma (NVG) and enucleation (mainly for local recurrence or NVG) were 27.0% and 19.5%, respectively. Enucleation rates decreased over time. The 5-year local control was 94%. Mean baseline visual acuity was 20/63, and visual acuity ≥20/200 was preserved in 20% of patients. At 5 years, 25% of T3 patients presented with metastasis; overall and specific survival rates were 65% and 75%, respectively.
Conclusion
Local control after PBT remained good with increasingly manageable complications and fewer secondary enucleations over time for these large melanomas. As PBT does not seem to deteriorate survival in these patients having a high risk of metastasis, PBT may be considered as a safe and efficient alternative to enucleation in patients with large choroidal melanoma, and may help to spare some vision.
Uveal melanoma has an incidence of 5–6 cases per million per year. It is the most common primary intraocular malignancy and it is also the most common noncutaneous melanoma. Historically, enucleation has been the gold standard in the treatment of malignant intraocular tumors. Starting in the seventies, conservative approaches, such as ophthalmic plaque brachytherapy, have been developed for small to medium-sized melanomas. Further, a prospective and Collaborative Ocular Melanoma Study (COMS) suggested, in 2006, that small to medium-sized choroidal melanomas could be treated by enucleation or conservative treatment using brachytherapy, with similar survival and metastasis-free survival rates with the 2 treatment modalities. A that time, the American Brachytherapy Society declared that patients with a clinical diagnosis of medium-sized choroidal melanoma (between 2.5 and 10 mm in height and <16 mm basal diameter) were candidates for episcleral plaques. However, with plaque radiotherapy, the higher the tumor, the higher the scleral dose, with difficulties to deliver a sufficient dose to the apex of the tumor for high tumors, depending or the radionuclide used. Moreover, treating tumors close to the optic nerve can also be challenging with plaque brachytherapy.
Another conservative approach uses proton beam therapy (PBT). A COMS trial compared external beam radiotherapy followed by enucleation with enucleation alone for patients with large choroidal melanomas and found similar 5- and 10-year survival rates. Additionally, the use of PBT has some advantages compared to brachytherapy. PBT allows for the treatment of even higher tumors and tumors closer from the optic nerve than brachytherapy, using a spread-out Bragg peak, which results in a steep distal dose fall-off beyond the tumor. While PBT may be associated with more anterior segment complications, preliminary experiences have shown interesting eye retention rates following PBT. Moreover, despite less favorable selection biases in irradiated vs enucleated patients, a retrospective and comparative study corroborated these findings in showing that cumulative all-cause mortality, melanoma-related mortality, and metastasis-free survival were not statistically different between the two. Also, eye retention and best-corrected visual acuity (BCVA) over 20/200 were obtained in about 75% of patients.
One particular challenge relates to large uveal tumors, as they may be associated with an increased risk of local failure with conservative therapies. Additionally, large irradiated volumes at very high doses are at higher risk for complications that may ultimately result in secondary enucleation. Another area of concern is the intrinsically high risk of liver metastasis in this population. Altogether, the management of large uveal melanomas is challenging.
In consideration of the trend toward using PBT for ever larger uveal melanomas, we evaluated its validity in treating T3-T4 uveal melanomas with respect to survival, metastasis-free survival, local complications, and enucleation.
Methods
This is an observational monocentric consecutive cohort study with national review board–approved prospective data collection for patients with a large choroidal melanoma treated by proton beam therapy at the cyclotron of the Centre Antoine Lacassagne cancer center (Nice, France) from June 1991 to June 2015.
The 2009 edition of the American Joint Committee on Cancer (AJCC) defines ciliochoroidal melanoma T stage by tumor height, basal diameter, extension to the ciliary body, and/or presence of extrascleral extent. Patients with AJCC tumor (T) stage 3–4 were included according to national guidelines if they had tumors smaller than 18 mm in maximum diameter and thickness inferior to 12 mm, extrascleral extension inferior to 2 mm, tumor/eyeball volume below 40%, and absence of unmanageable glaucoma.
The patient database included data on demographics, laterality (right or left), location of the tumor (pre-equatorial, equatorial, or retroequatorial), tumor measurements, distance between posterior tumor margins to the optic disc and macula (mm), presence of inflammation, increased intraocular pressure, intravitreal hemorrhage, retinal detachment, iris root involvement, extrascleral extension, vorticose vein involvement, and BCVA at baseline and on follow-up. BCVA was assessed in the Snellen system and converted into a logMAR scale using the formula −log (visual acuity) for statistical analysis. No light perception, light perception only, hand motion, and count fingers were considered as 3, 2.5, 2.3, and 1.9 logMAR, respectively. Tumor basal diameter and thickness were measured by ultrasonography and indirect ophthalmoscopy with fundus photographs, peroperative eye transillumination, and fluorescein angiography were also performed for accurate tumor characterization. Optical coherence tomography and ultrabiomicroscopy were performed based on tumor location and the ophthalmologist’s appreciation. Metastatic diagnostic evaluation consisted of liver ultrasonography or computed tomography (CT) scan and liver function. All patients were informed of the risks and potential benefits related to proton therapy and enucleation. We evaluated the complications of PBT such as cataract, neovascular glaucoma (NVG), retinopathy, neuropathy, intravitreal hemorrhage, retinal detachment, and enucleation.
Proton Beam Therapy Planning
The method has been described elsewhere. In brief, the method involved surgical insertion of 4 tantalum fiducials, sewed onto the sclera around the transilluminated tumor by the onco-ophthalmologist under a short general anesthesia. The dimensions of the tumor were noted, along with the tantalum fiducial–limbus and interfiducial distances. CT-based PBT planning was performed 2 weeks later. Tridimensional eye modeling and tumor/organs at risk delineation was generated using the eye-dedicated treatment planning system, according to the information provided by fiducial placement, retinography, and angiographies. The total dose delivered was 60 cobalt gray equivalent in 4 fractions, which is the usual protocol used in Europe.
Patient Follow-up
Patients were regularly followed by their onco-ophthalmologist every 6 months for 2 years, and yearly thereafter. A retinal photography or angiography, measurement of visual acuity, and ultrasound B for the evaluation of tumor regression were performed. Patients had an initial monthly follow-up by their local ophthalmologist to assess complications. Patients were addressed to the onco-ophthalmologist in case of occurrence of any radiation-related ocular events. After the first year, patients underwent interval biannual visits with their local ophthalmologist. Metastatic screening was performed every 6 months for 5 years with liver ultrasound and liver function tests.
Statistics
Statistical analyses were performed using SPSS 22.0 (SPSS Inc, Chicago, Illinois, USA) statistical package for Macintosh. Continuous data are presented as the mean ± standard deviation (SD) while categorical variables were presented as frequencies and percentages. Continuous variables were compared using Student t test while categorical variables were compared using the χ 2 test. Univariate and multivariate Cox proportional hazards regression analyses were performed to relate clinical and ultrasound parameters to the occurrence of NVG, enucleation, overall and specific survival, and occurrence of metastasis. Event rates for the overall, specific, and free-of-NVG survival were plotted in Kaplan-Meier curves, and the log-rank test was used to compare overall and specific survival across T3 and T4 stages. All statistical tests were 2-sided, and a P value of <.05 was considered statistically significant.
Results
Description of Patient Population
During a 24-year accrual period, 492 out of 1460 patients (33.7%) have been treated by proton beam therapy for a large choroidal melanoma. Of these, 416 patients were classified as T3 (84.6%) and 75 as T4 (15.2%). Mean follow-up was 61.9 months (SD 47.8 months). Qualitative and quantitative tumor characteristics are shown in Tables 1 and 2 .
| Number | (%) | |
|---|---|---|
| Sex | ||
| Male | 258 | (52.8) |
| Female | 234 | (47.6) |
| Eye | ||
| Right | 238 | (48.4) |
| Left | 253 | (51.4) |
| Pre-existing nevus | 2 | (0.4) |
| Tumor location | ||
| Pre-equatorial | 107 | (21.7) |
| Equatorial | 274 | (55.7) |
| Retroequatorial | 108 | (22.0) |
| Initial inflammation | 59 | (12.0) |
| Initial intravitreal hemorrhage | 61 | (12.4) |
| Initial presence of metastasis | 8 | (1.6) |
| Extrascleral extension | 22 | (4.5) |
| Vorticose vein involvement | 30 | (6.1) |
| Ciliary body involvement | 205 | (41.7) |
| Iris root involvement | 38 | (7.7) |
| T stage | ||
| T3 | 416 | (84.6) |
| T4 | 75 | (15.2) |
| Mean | Range | |
| Age (y) | 62.4 | 19–89 |
| BCVA before treatment (Snellen scale) | 20/63 | 20/1000–20/20 |
| Tumor thickness (mm) | 8.77 | 2–15 |
| Tumor diameter (mm) | 14.91 | 7–24.1 |
| Tumor volume (cc) | 0.92 | 0.01–19 |
| Tumor Location | T3 (N = 416) Number (%) | T4 (N = 75) Number (%) | P (χ 2 ) |
|---|---|---|---|
| Juxtapapillary | 77 (18.5%) | 15 (20%) | .35 |
| Parapapillary | 174 (41.8%) | 29 (38.7%) | .25 |
| Ciliary body involvement | 153 (36.8%) | 52 (69.3%) | <.001 |
| Macular involvement | 96 (23.2%) | 19 (25.3%) | .08 |
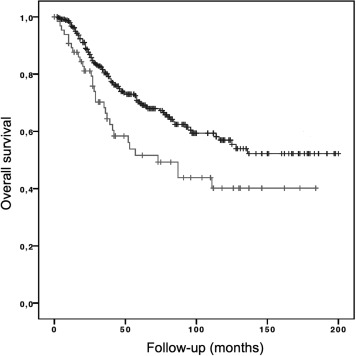
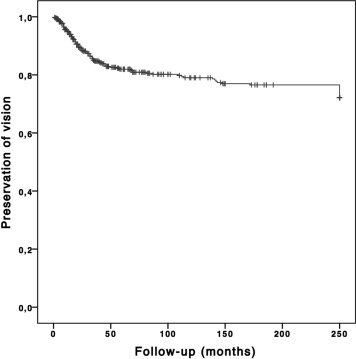
Two hundred and fifty-eight patients were male (52.4%) and 234 were female (47.6%). Mean age at diagnosis was 62.4 years (19–89). Both eyes were equally involved (48.5% in the right eye and 51.5% in the left eye). Mean tumor thickness and diameter were 8.77 (2–15) mm and 14.91 (7–24.1) mm, respectively. Mean tumor volume was 0.92 cc (0.01–19). Mean macular and optic disc distance were 4.56 (0–19.9) mm and 4.59 (0–22.1) mm, respectively. Tumor location was pre-equatorial in 21.7%, equatorial in 55.7%, and retro-equatorial in 22.0%. Mean BCVA on the Snellen scale was 20/63 before treatment and 20/160 at last follow-up visit. At last visit, BCVA was inferior to 20/200 for 80.2% of the patients and superior to 20/40 in 8.5%. Among the nonenucleated patients, 76.3% of patients could at least experience light perception ( Figure 1 ). Comparing final to baseline BCVA, 91.4% of patients had lost ≥0.3 logMAR of visual acuity and 8.6% had steady or better visual acuity. Of those patients losing VA, 30.4%, 56%, 72.2%, and 91.4% had lost more than 0.3 logMAR of VA within the first 2 years, between 2 and 5 years, between 5 and 10 years, and between 10 and 20 years, respectively ( Figure 2 ). Of the 492 large choroidal melanoma patients, 12.4% had an intravitreal hemorrhage, 62.8% had a retinal detachment, 4.5% had an extrascleral extension, 41.7% had a ciliary body extension, and 7.7 % had iris root involvement at baseline. Of these, 1.6% had liver metastasis at diagnosis of ocular disease.
Events During Follow-up
Anterior and posterior segment complications after proton beam therapy are displayed in Table 3 . In this T3-T4 population, 27.0% (119 T3 and 14 T4) of the patients had NVG. Of these, 40.6% patients were enucleated. The mean delay between proton beam therapy and NVG was 21.65 months (SD 26.13 months). Risk factors for NVG by univariate and multivariate Cox proportional hazard regression analyses were ( Table 4 ) distance to the optic disc ( P < .01) and macula ( P < .01), presence of a retinal detachment at last visit ( P < .01), initial tumor thickness ( P < .01), initial tumor diameter ( P = .01), initial presence of an intravitreal hemorrhage ( P < .01), and local recurrence ( P < .01). Overall, 19.5% of the patients were enucleated. Reasons for enucleation were NVG (30.2%), phthisis (12.5%), relapse (32.3%), and unreliable surveillance (24.8%). The mean delay between proton beam therapy and enucleation was 35.9 months (SD 43.9 months). Risk factors for enucleation on univariate and multivariate analyses ( Table 5 ) were local recurrence ( P < .01), NVG ( P < .01), radiation-induced retinopathy ( P = .02), presence of a retinal detachment after treatment ( P = .03), TNM stage ( P < .01), and initial tumor thickness ( P < .01). Owing to changes in the management of complications with the use of intravitreal VEGF inhibitors in 2008, we evaluated NGV and enucleation rates before and after 2008. The NVG rate increased from 21.6% to 36.7% while enucleation rates decreased from 38.2% to 20.0% during the same periods of time ( P < .01), regardless of tumor size.
| Complications | Total N (%) | T3 (N = 416) N (%) | T4 (N = 75) N (%) |
|---|---|---|---|
| Cataract | 196 (39.8) | 164 (39.4) | 32 (42.7) |
| Neovascular glaucoma | 133 (27.0) | 119 (28.6) | 14 (18.7) |
| Retinopathy | 115 (23.4) | 102 (24.5) | 13 (17.3) |
| Neuropathy | 41 (8.3) | 38 (9.1) | 3 (4.0) |
| Intravitreal hemorrhage | 84 (17.1) | 78 (18.8) | 6 (8.0) |
| Lipidid exudation | 57 (11.6) | 52 (12.5) | 5 (6.7) |
| Dry eye syndrome | 73 (14.8) | 65 (15.6) | 8 (10.7) |
| Lacrimal stenosis | 16 (3.3) | 16 (3.8) | 0 (0.0) |
| Alopecia | 53 (10.8) | 48 (11.5) | 5 (6.7) |
| Dermatitis | 29 (5.9) | 24 (5.8) | 5 (6.7) |
| Enucleation | 96 (19.5) | 74 (17.8) | 22 (29.3) |
| Retinal detachment | Before Treatment N (%) | After Treatment N (%) | |
| 0 = none | 0 | 183 (37.2) | 276 (56.1) |
| 1 = peritumoral | 1 | 87 (17.7) | 26 (5.3) |
| 2 = 1 or 2 quadrants | 2 | 204 (41.5) | 56 (11.4) |
| 3 = 3 or 4 quadrants | 3 | 13 (2.6) | 23 (4.7) |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | P Value | HR | 95% CI | P Value | |
| Tumor thickness | 1.15 | 1.07–1.24 | <.01 | 1.16 | 1.06–1.26 | <.01 |
| Local recurrence | 1.31 | 1.08–1.58 | <.01 | 1.33 | 1.06–1.66 | .02 |
| Retinal detachment after treatment | 1.57 | 1.42–1.73 | <.01 | 1.46 | 1.31–1.63 | <.01 |
| Initial intravitreal hemorrhage | 2.99 | 2.10–4.29 | <.01 | 2.31 | 1.57–3.39 | <.01 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | P Value | HR | 95% CI | P Value | |
| Stage T of 7th TNM | 1.88 | 1.17–3.02 | .01 | 2.27 | 1.29–3.99 | <.01 |
| Tumor thickness | 1.35 | 1.23–1.50 | <.01 | 1.28 | 1.15–1.53 | <.01 |
| Local recurrence | 1.48 | 1.25–1.77 | <.01 | 1.74 | 1.45–2.08 | <.01 |
| Neovascular glaucoma | 14.84 | 4.24–51.92 | <.01 | 28.54 | 3.30–246.72 | <.01 |
| Radiation-induced retinopathy | 3.37 | 1.75–6.50 | <.01 | 2.52 | 1.13–5.63 | .02 |
| Retinal detachment after treatment | 11.35 | 3.29–39.14 | <.01 | 10.17 | 1.19–87.33 | .03 |
In our population, 39.8% developed cataract, 23.4% presented with a radiation retinopathy, 8.3% had a radiation neuropathy, and 17.1% had an intravitreal hemorrhage following proton beam therapy. Other complications included dry eye syndrome (14.8%), lacrimal stenosis (3.3%), dermatitis (5.9%), and alopecia (10.8%).
Local Tumor Control
Local control was achieved in 94% of the patients at year 5. Mean time to local relapse was 29.0 months (SD 27.40). Local relapses were treated with proton reirradiation (24.1%), enucleation (65.5%), or laser (10.3%). Initial tumor thickness ( P < .01) was a risk factor for local relapse on univariate and multivariate analyses.
Survival and Metastasis
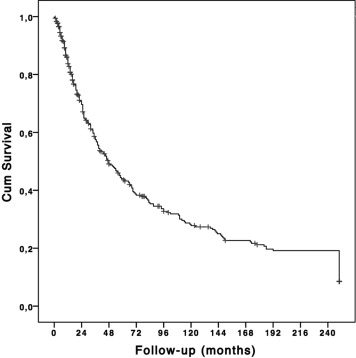
Median overall survival in the combined T3 and T4 population was 126.6 months (range 116.7–136.4 months for the patients who experienced the event). The Kaplan-Meier estimate for overall survival was 68% and 52% at 5 years and 54% and 40% at 10 years in the T3 and T4 patients, respectively ( Figure 3 and P = .01). The Kaplan-Meier estimate for specific survival was 77% and 62% at 5 years and 71% and 59% at 10 years in the T3 and T4 patients, respectively ( Figure 4 and P = .02). In multivariate analysis, risk factors for poorer overall survival ( Table 6 ) were an older age ( P < .01), juxtapapillary location (tumor abutting the optic disc) ( P = .02), and occurrence of metastasis during follow-up ( P < .01). Using Kaplan-Meier estimates, metastases were detected in 25.0% of the patients at 5 years, 25.0%, 10 years, and 30.0% at 15 years in T3 patients, and 35.0% at 5 or 10 years and 43.0% at 15 years in T4 patients. The mean time to metastasis was 33.3 months (SD 36.5). Risk factors for the development of metastases were juxtapapillary location ( P < .01), extrascleral extension ( P = .046), and ciliary body extension ( P < .01) ( Table 7 ). Genomics are not available, as they have only been performed since 2013.