6 Otology, Neurotology, and Lateral Skull Base Surgery
Overview
1 | Describe the sensory innervation of the pinna and external auditory canal (EAC). | Sensation of the auricle is provided by the greater auricular and lesser occipital nerve (from the cervical plexus), as well as small sensory branches of the facial nerve and auriculotemporal nerve. The EAC is supplied by overlapping contributions from cranial nerves (CN) V, VII, IX, and X. |
2 | What is the foramen of Huschke? | The foramen of Huschke is a developmental defect resulting from incomplete fusion of the greater and lesser tympanic spines. When present, it creates a connection between the EAC and the parotid gland, glenoid fossa or infratemporal fossa. |
3 | What are the fissures of Santorini? | The fissures of Santorini are anatomical communications that allow lymphatic movement between the anterior cartilaginous EAC and the parotid gland and glenoid fossa. |
4 | What is the notch of Rivinus? | The notch of Rivinus is the deficient portion of the tympanic annulus where the pars flaccida attaches to the squamous portion of the temporal bone. |
5 | How are the pars flaccida and pars tensa of the tympanic membrane structurally different? | The pars flaccida is, as its name implies, more compliant than the pars tensa. The pars tensa is slightly thicker and contains a middle fibrous layer in addition to an outer skin layer and inner mucosal layer. |
6 | The tympanic membrane is formed by what embryonic layer(s)? | The outer epidermal layer from the first branchial cleft (ectodermal origin); middle fibrous layer from neural crest mesenchyme (mesodermal origin); inner mucosal layer from the first pharyngeal pouch (endodermal origin) |
7 | Where does the carotid artery lie in relation to the eustachian tube? | The carotid artery courses just medial to the more anterior cartilaginous portion of the eustachian tube. |
8 | In patients with cleft palate, dysfunction of which muscle is most strongly implicated in causing recurrent otitis media? | Tensor veli palatini |
9 | What is the most common intratemporal location of facial nerve dehiscence? | It occurs most commonly near the oval window, second most commonly at the second genu. |
10 | Describe the origin, insertion, and action of the tensor tympani muscle. | The tensor tympani originates from the greater wing of the sphenoid, cartilage of the eustachian tube, and the walls of the semicanal of the tensor tympani. Its tendon then wraps around the cochleariform process to insert onto the medial aspect of the neck and manubrium of the malleus. It functions to medialize the tympanic membrane and increase the impedance of the ossicular chain. |
11 | What landmarks may be used to help identify the facial nerve during middle ear surgery? | The Jacobson nerve, located on the cochlear promontory, can be followed superiorly to the cochleariform process. The facial nerve is immediately medial and superior to the cochleariform process and tensor tympani. The facial nerve can also be identified immediately superior to the oval window. |
Aside from the muscles of facial expression, what muscles does the facial nerve innervate? | In addition to the muscles of facial expression, the facial nerve innervates all the other muscles of the second branchial arch, specifically, the stapedius muscle, the stylohyoid, and the posterior belly of the digastric. | |
13 | What is the cog? | The cog is a coronally oriented bony septum located just anterior to the head of the malleus that seperates the anterior epitympanic recess (supratubal recess) from the attic. |
14 | When looking at the external surface of the mastoid cortex, what landmark can be used to approximate the level of the middle cranial fossa? | The temporal line, which represents the inferior insertion point of the temporalis muscle, can be used as a landmark. |
15 | Describe the boundaries of the Macewen triangle (suprameatal). | The suprameatal crest, posterior margin of the external auditory canal, and the tangential line from the posterior ear canal bisecting the suprameatal crest are the boundaries of the Macewen triangle, which approximates the antrum. |
16 | What is the Körner septum? | The Körner septum is a bony plate dividing the mastoid air cells superficial to the antrum. Embryologically, it is the junction between the petrous and squamous portions of the temporal bone and creates a “false bottom” during mastoidectomy. |
17 | Which cells are primarily responsible for transducing acoustic energy into neural signals? | Inner hair cells are the primary cells onto which afferent auditory neurons (spiral ganglion cells) synapse. The outer hair cells also contribute to transformation of acoustic energy into neural signal; however, they primarily play a role in “tuning” the cochlea to improve frequency selectivity and sensitivity. |
18 | What are the boundaries of the scala media? ( | In the cross-section of the cochlea, the scala media is separated from the scala vestibuli by the Reissner membrane. The basilar membrane and osseous spiral lamina separate the scala media and scala tympani. The boundaries of the outer periphery of the scala media are the stria vascularis and the spiral ligament. |

Fig. 6.1 Cross section of the cochlea and organ of Corti. (Used with permission from Thieme Atlas of Anatomy: Head and Neuroanatomy, © Thieme 2007, illustration by Karl Wesker.)
What two structures are connected by the perilymphatic (periotic) duct? | The perilymphatic duct, which runs in the bony canal of the cochlear aqueduct, connects the scala tympani of the cochlea and the subarachnoid space of the posterior cranial fossa. | |
20 | Which structures are innervated by the superior and inferior vestibular nerves, respectively? | Superior vestibular nerve innervates the superior and lateral semicircular canals and the utricle. Inferior vestibular nerve innervates the posterior semicircular canal, and the saccule. |
21 | Where is the primary auditory cortex located? | Brodmann areas 41 and 42 of the upper temporal lobe |
22 | Describe the geometric anatomy of the semicircular canals and the physiologic significance of this arrangement. | The three semicircular canals are located in three mutually perpendicular planes. This orientation provides the vestibular system with independent resolution of rotational movements in three different axes (pitch, roll, and yaw). |
23 | Describe the course and functions provided by the nervus intermedius. | The taste, secretory, and sensory fibers of the facial nerve are carried by the nervus intermedius. It exists as a distinct nerve in the cerebellopontine angle (CPA) and internal auditory canal (IAC), but on entering the meatal foramen, these fibers exist within the body of the facial nerve. |
24 | What cell bodies are located in the geniculate ganglion? | Cell bodies of the special sensory taste neurons carried by the chorda tympani nerve |
25 | What nerve fibers are carried by the greater superficial petrosal nerve? | Preganglionic parasympathetic fibers that synapse in the pterygopalatine ganglion, as well as afferent special sensory taste fibers that supply the soft palate |
26 | What percentage of temporal bone specimens demonstrate dehiscence of the geniculate ganglion on the floor of the middle fossa? | 16% |
27 | What is the prevalence of internal carotid artery dehiscence at the floor of the middle cranial fossa? | Approximately 20% |
28 | Describe the boundaries of the Glasscock triangle (posterolateral). | Greater superficial petrosal nerve, V3, line connecting foramen spinosum and arcuate eminence |
29 | Describe the boundaries of Kawase triangle (posteromedial). | V3, greater superficial petrosal nerve, arcuate eminence, superior petrosal sinus. It marks the boundaries of anterior petrosectomy for gaining access to the posterior fossa. |
30 | What extratemporal branches of the facial nerve arborize proximal to the pes anserinus? | The postauricular nerve, nerve to the stylohyoid, and nerve to the posterior belly of the digastric muscle |
31 | The external ear is formed by what mesodermal structures? ( | The six hillocks of His: • First Arch 1: Tragus 2: Helical crus 3: Helix • Second Arch 4: Antihelix 5: Antitragus 6: Lobule |
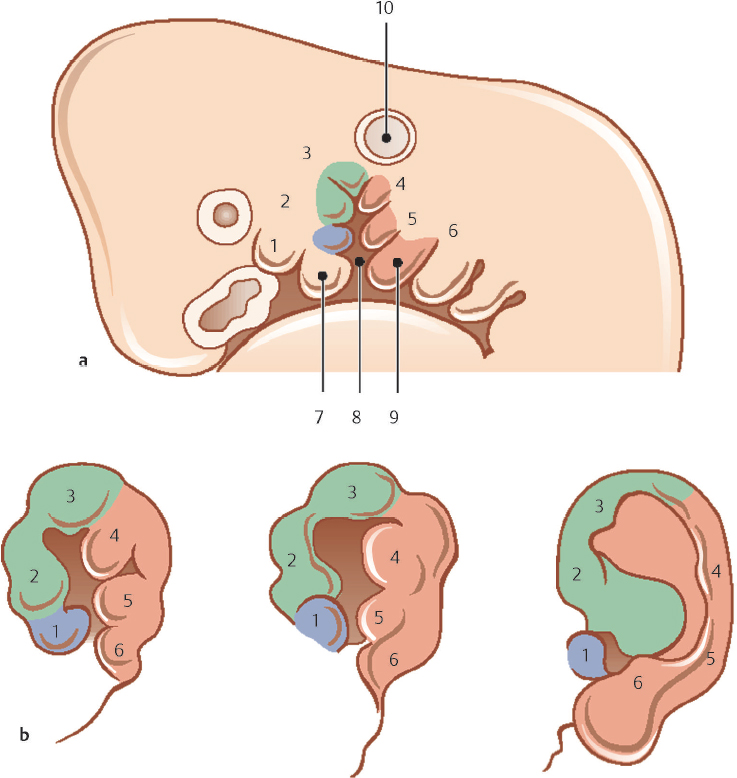
32 | Incomplete fusion or supernumerary development of the hillocks of His may lead to what conditions? | Preauricular cysts, pits, or tags |
33 | Describe the embryologic basis of a persistent stapedial artery. | The stapedial artery is derived from the second branchial arch. This is normally a transient structure, but in rare instances, it can persist into adulthood. |
34 | What skull base abnormality is classically seen with a persistent stapedial artery? | Lack of an ipsilateral foramen spinosum |
Describe the embryologic origin(s) of the ossicles. | The head and neck of the malleus, as well as the incus body and short process, are derived from the first branchial arch (Meckel cartilage). The manubrium of the malleus, long process and lenticular process of the incus, and the stapes superstructure are derived from the second branchial arch (Reichert cartilage). The vestibular half of the stapes footplate and annular ligmanent are thought by many authorities to be derived from the otic capsule. | |
36 | From which germ cell layers and branchial arch (es) does the otocyst arise? | First seen at the end of the 3rd week of development, the otic placode is a thickening of the ecdodermal surface of the first branchial groove. This invaginates into the underlying mesoderm, which it eventually becomes surrounded by to form the otocyst. This structure goes on to develop into the otic labyrinth. |
37 | List the primary acoustic functions of the external ear. | • Filter to reduce low-frequency background noise • Resonator to amplify mid frequency sounds (up to 20 dB) • Direction-dependent filter to augment spatial perception at high frequencies |
38 | Compared with adults, what anatomical characteristics of the eustachian tube in young children predisposes toward development of acute otitis media? | The eustachian tube is narrower, shorter, and oriented more in a horizontal plane in children, putting the middle ear at a higher risk for exposure to nasopharyngeal secretions and poor aeration. |
39 | Describe the acoustic transformer mechanism of the middle ear. | The three “levers” provide an average gain of 20 to 30 dB: • Catenary lever: Elastic properties of stretched tympanic membrane fibers directing sound to the centralized malleus • Ossicular lever: The length of the manubrium of the malleus divided by the length of the long process of the incus (1:3 ratio) • Hydraulic lever: A 22:1 ratio of the tympanic membrane to the oval window |
40 | Describe the electrolyte composition of the cochlear fluids. | Perilymph located in scala vestibul and scala tympani is similar to serum and cerebrospinal fluid (CSF) in electrolyte composition (high Na and low K concentration). Endolymph is located within the scala media and is similar to intracellular fluid in electrolyte composition (low Na and high K concentration). |
41 | How are movements of the oval window (stapes footplate) and the round window membrane related? | They are out of phase by 180 degrees. In other words, motion at the oval window into the vestibule leads to an outward movement of the round window membrane into the middle ear. If pressure is exerted on both the round window and oval window simultaneously and equally, phase cancellation occurs resulting in significant hearing loss. |
42 | Describe the tonotopic organization of the cochlea. | The cochlea (specifically the basilar membrane) is tonotopically “tuned,” such that the high frequency sounds are most effectively transduced at the basal cochlea, whereas low-frequency sounds are best transduced in the apical segments. |
43 | What effects do ampullopedal and ampullofugal displacement of the semicircular canal kinocilia have on the firing rates of the vestibular nerves? | Ampullopetal (toward the vestibule) displacement of the kinocilia of the horizontal canal and ampullofugal (away from the vestibule) displacement of the kinocilia of the superior and posterior canals increase vestibular nerve firing rates. |
Vestibular Evaluation
44 | Define first-degree, second-degree, and third-degree nystagmus. | • FIrst degree: Occurring when gazing in the direction of the fast component • Second degree: Occurring when gazing in the direction of the fast component or at midline • Third degree: Occurring when gazing in all directions |
45 | Describe Alexander’s law? | The amplitude of the nystagmus will intensify when the patient looks in the direction of the fast phase. Alexander’s law describes the pattern of nystagmus in a patient with a unilateral peripheral vestibular deficit. |
46 | Describe Ewald’s three laws? | 1. The axis of nystagmus parallels the anatomic axis of the semicircular canal that generated it. 2. In the lateral semicircular canals, ampullopetal endo-lymph movement causes greater stimulation than ampullofugal movement. 3. In the superior and posterior semicircular canals, the reverse is true. |
47 | Describe examination findings that help distinguish between central and peripheral vestibular deficits. | • Central deficits may occur in any direction (vertical, horizontal, or torsional), may alternate direction, do not suppress with visual fixation, do not fatigue, rarely are associated with hearing loss, often have other abnormal neurologic examination findings, have minimal latency with positional change, and often less severe. • Peripheral deficits are unidirectional; horizontal only (no vertical component), suppresses with visual fixation, often with concurrent hearing loss, otherwise normal neurological examination, positional nystagmus that often has a 2 + second latency, generally more severe. |
48 | Describe the direction of nystagmus with irritative and destructive vestibulopathy? | Irritative vestibulopathy is associated with a fast phase beating toward the affected ear, whereas destructive vestibulopathy is associated with a fast-phase beating away from the affected ear. |
49 | What is the purpose of Frenzel goggles? | • Frenzel goggles assist in evaluating for nystagmus. • Frenzel goggles magnify and illuminate the patient’s eyes and prevent gaze fixation. |
50 | What inner ear structure and nerve do thermal calorics testing interrogate? | Thermal calorics measure the responsiveness of the horizontal semicircular canal (and superior vestibular nerve) to thermal stimuli and is one of the few quantitative evaluations that can test the two ears independently. |
51 | Describe the effects of cold and warm irrigation during caloric testing. | Cold causes the fast phase of nystagmus to beat toward the opposite ear, whereas warm causes the fast phase to beat toward the ipsilateral ear. |
52 | How is electronystagmography (ENG) or videonystagmography (VNG) useful in the evaluation of the dizzy patient? | Nystagmography comes in several forms (ENG or VNG) and serves to quantitatively measure eye movements while performing positional testing or calorics. |
53 | What is computerized dynamic posturography? | This technique, used to quantify postural control in an upright (standing) position in either static or dynamic conditions, requires coordination of sensory input, motor output, and central integration. |
54 | What inner ear structure and cranial nerve does VEMP testing interrogate? | Saccule and inferior vestibular nerve |
55 | How is computerized dynamic posturography performed? | The patient is placed on a platform that is capable of performing various movements and sensing patient sway (oscillations). Additionally, a visual backdrop is placed in front of the patient and can be held stationary or can move. The patient is then subjected to six increasingly difficult tests. |
What pattern of results may be seen in a malingering patient during computerized dynamic posturography? | The patient has poor scores with easier tasks, but as the task difficulty increases, the patient may do disproportionately better. | |
57 | What does the dynamic visual acuity test evaluater? | It tests for impaired ability to preceive objects accurately during head movement. Normally, the vestibular ocular reflex maintains the direction of gaze on a fixed target by moving the eyes in the opposite direction of head movement. |
58 | Dysdiadochokinesia is a sign of dysfunction involving what structure? | Dysdiadochokinesia, the difficulty with performing rapid alternating movements, is considered a sign of cerebellar pathology. |
59 | How is the Fukuda test performed, and what does it evaluate? | The patient is asked to march in place with eyes closed for 50 steps. Rotation (> 30 degrees) may indicate asymmetrical labyrinthine function. Rotation generally occurs toward the side of the lesion. |
60 | What is purpose of the vestibulo-ocular reflex? | This reflex generates eye movements in response to head motions perceived by the peripheral vestibular system, permitting visual fixation on an object while the head is moving. |
61 | How do you perform a head-thrust test? | The patient is asked to fixate on the examiner’s nose while the head is passively and rapidly rotated in the excitatory direction of a semicircular canal. Normally, the patient will be able to maintain fixation on the examiner. |
62 | What constitutes a positive head-thrust test? | In the case of a left hypoactive labyrinth, the vestibuloocular-reflex will be impaired, and the head-thrust test toward the patient’s left side will be positive; the examiner will note the patient’s eyes to rotate with the head, and after a brief delay, a “catch-up saccade” toward the right will bring the gaze back toward the examiner. |
63 | Describe the Hennebert sign? | Induction of nystagmus or vertigo with changes in external auditory canal pressure (tragal pressure, pneumatic otoscopy) |
64 | What conditions are associated with a positive Hennebert sign? | Superior semicircular canal dehiscence, perilymphatic fistula, lateral semicircular canal fistula from chronic ear disease, or otosyphilis |
65 | Describe a positive Tullio phenomenon. | Tullio phenomenon is noise-induced activation of the vestibular system resulting in dizziness and/or nystagmus. Historically, it is associated with syphilis but may occur with inner ear fistula and/or dehiscence syndromes. |
66 | How is a Romberg test performed? | The patient stands with feet close together and arms at the sides. The clinician evaluates the relative amount of body sway with the patient’s eyes closed compared with when they are open. |
67 | What is a Romberg test evaluating? | Somatosensation and proprioception carried out by the cerebellum and dorsal column-medial lemniscus |
68 | In what clinical situations would rotary chair testing be useful? | Because rotatory chair testing evaluates bilateral semicircular canal function simultaneously (unlike caloric testing), it may be used for evaluating suspected bilateral vestibular loss (after meningitis, vestibulotoxic medications, etc.). |
69 | What symptom is classically associated with severe bilateral peripheral vestibular hypofunction? | Oscillopsia |
Vestibular and Balance Disorders
70 | Review the differential diagnosis of Ménière disease. | Perilymphatic fistula, vestibular migraine, Cogan syndrome, autoimmune hearing loss, syphilis, mumps, Mondini malformation |
71 | What percentage of patients with Ménière disease will develop bilateral involvement? | Approximately 30% |
72 | What medical treatments are most commonly used for symptomatic treatment of active Ménière disease? | • Vestibular suppressants (e.g., benzodiazepines promethazine) • Rest • Potentially corticosteroids |
73 | What are the two most commonly used surgical approaches for vestibular neurectomy? | • Middle fossa or the retrosigmoid approach • Retrolabyrinthine and transmeatal approaches have also been used. |
74 | How does the efficacy of endolymphatic shunt placement compare with endolymphatic sac decompression for treatment of Ménière disease? | No trials have clearly demonstrated superior results in one treatment over the other. |
75 | Review the clinical presentation of Ménière disease. | Low-frequency sensorineural hearing loss (SNHL, fluctuating and progressive), roaring tinnitus, aural fullness, and episodic vertigo generally lasting for hours |
76 | Describe Lermoyez syndrome. | Tinnitus and hearing loss that remit after an attack of vertigo |
77 | Define possible, probable, definite and certain Ménière disease. | • Possible: Episodic vertigo without documented hearing loss or SNHL (fluctuating or fixed) with dysequilibrium but without definitive vertigo episodes; other causes excluded • Probable: One definitive episode of vertigo, audiometrically documented hearing loss on at least one occasion, tinnitus or aural fullness in the treated ear; other causes excluded • Definite: Two or more definitive spontaneous episodes of vertigo lasting 20 minutes or longer, audiometrically documented hearing loss on at least one occasion, tinnitus or aural fullness in the treated ear, other causes excluded • Certain: Definite Ménière disease plus histopathologic confirmation |
78 | Describe diet modifications for treatment of Ménière disease. | • Avoidance of alcohol, caffeine, tobacco and monosodium glutamate • Adherence to a low-sodium diet (less than 1 to 2 g/day) |
79 | How is electrocochleography used in the diagnosis of Ménière disease? | If the ratio of the summating potential, generated by the organ of Corti, and the action potential, generated by the auditory nerve, is elevated, diagnosis is indicated. A value of 0.5 or greater is considered suggestive of Ménière disease. |
80 | How is electrocochleography performed? | Neural responses to presented sounds are recorded through an electrode in the middle ear (transtympanic needle electrode), on the tympanic membrane, or on a gold foil-wrapped earplug. |
81 | What is the role of intratympanic injections of gentamicin in the treatment of Ménière disease? | • Selectively vestibulotoxic ablative treatment for unilateral Ménière disease, often pursued after failure of more conservative measures such as low-salt diet, caffeine avoidance, diuretic therapy, and intratympanic steroid injection • Carries a 5 to 20% chance of significant SNHL |
What is the role of intratympanic injections of corticosteroids in the treatment of Ménière disease? | These injections are onsidered a nonablative adjunct to medical therapy that carries little risk of inducing hearing loss. Subjects may experience a brief episode of vertigo with injection if the steroid is not body temperature and a low risk for persistent tympanic membrane perforation. | |
83 | When is a patient considered a candidate for endolymphatic sac surgery? | Frequent vertiginous spells despite conservative treatment in patients who are not candidates for ablative procedures (bilateral disease, good residual hearing, contralateral vestibular hypofunction) |
84 | What is the Donaldson line? | The Donaldson line is an imaginary line running parallel to the plane of the lateral semicircular canal, extending posteriorly and inferiorly through the center of the posterior semicircular canal. The endolymphatic sac lies just inferior to this line on the posterior fossa dura. |
85 | What pure tone audiometric findings can be seen in patients with superior semicircular canal dehiscence? | Conductive hyperacusis is sometimes seen, with bone conductive thresholds occasionally less than 0-dB hearing loss. This can lead to an air-bone gap even when air conductive thresholds are within the normal range. |
86 | Describe the third window phenomenon. | The third window refers to a third opening in the inner ear, in addition to the round and oval windows, that permits pathological movement of perilymph within the labyrinth, which may induce vertigo. |
87 | Describe the clinical presentation of superior semicircular canal dehiscence syndrome. | Aural fullness, autophony, hearing loss (generally with an air-bone gap and often supranormal bone conduction), and dizziness often associated with loud sounds, exertion or straining |
88 | How can one differentiate otosclerosis from superior semicircular canal dehiscence syndrome? | Patients with otosclerosis often have type AS tympanograms, diphasic or absent stapedial reflexes, and elevated to absent cervical vestibular evoked myogenic potentials. Patients with superior semicircular canal dehiscence will usually have normal stapedial reflexes, type A tympanograms, and diminished vestibular evoked myogenic potential thresholds (often < 70 dB). |
89 | How do you perform and interpret the DixHallpike test? | With the patient sitting, rotate the patient’s head by approximately 45 degrees to the left or the right. The patient then lies flat with the head slightly extended (~ 20 degrees). The eyes are then observed for ~ 45 seconds looking for rotary nystagmus. If rotatory nystagmus occurs, the test is positive. The direction of the fast phase reveals the side that is affected. |
90 | Describe the clinical manifestation of benign paroxysmal positional vertigo? | Short-lived (less than 60 seconds), room-spinning vertigo provoked by head turn |
91 | Which semicircular canal is most commonly involved in benign paroxysmal positional vertigo? | Posterior canal. Five percent involve the horizontal canal and the superior canal is the least common. |
92 | What anatomical structure is the source of otoconia in benign paroxysmal positional vertigo? | The utricle |
93 | What are risk factors for the development of benign paroxysmal positional vertigo? | • Advanced age, head trauma, surgery, migraine • Most patients do not have an identifiable cause (idiopathic). |
94 | Describe the mechanism of singular neurectomy in the treatment of benign paroxysmal positional vertigo. | The singular nerve innervates the posterior semicircular canal, which is the most commonly affected canal in benign paroxysmal positional vertigo. Division of this nerve may lead to symptom relief in refractory disease. |
What conservative treatment options are available for benign paroxysmal positional vertigo? | • Reassurance and education about the nature of the condition • No effective pharmacologic therapy is available • Canalith repositioning maneuvers involve taking a patient through a series of positions that are designed to return dislodged otoconia to the vestibule and are the most effective nonsurgical treatment. | |
96 | What test(s) should be ordered when vertebrobasilar insufficiency is suspected? | • MRI and magnetic resonance angiography (MRA) provide the best information regarding acute and chronic infarcts, as well as the location and severity of vascular occlusions in the head and neck. • Patients who cannot undergo MRI should be evaluated with CT and CT angiography (CTA). • Duplex ultrasound can also provide information regarding proximal vertebral arteries. |
97 | What symptoms may accompany episodic vertigo associated with vertebrobasilar insufficiency? | Diplopia, decrease in visual acuity, ataxia, dysarthria, dysphagia, and other focal neurologic symptoms |
98 | Describe the symptoms of Wallenberg syndrome. | • Loss of pain and temperature sensation on the ipsilateral face and contralateral body, dysphagia, dysarthria, ataxia, vertigo, Horner syndrome, diplopia • Caused by a lateral medullary infarct supplied by the posterior inferior cerebellar artery |
99 | What are typical initial symptoms of vestibular neuronitis? | • Sudden onset of severe vertigo, nausea, and vomiting lasting days to weeks, often preceded by a viral upper respiratory tract infection • Unlike labyrinthitis, hearing should remain stable. |
100 | What are the mainstays of treatment for vestibular neuronitis? | High-dose corticosteroids, vestibular suppressants in the acute period, antiemetics, and bed rest as needed |
101 | What are the diagnostic criteria for chronic subjective dizziness? | • Subjective unsteadiness or nonvertiginous dizziness that is present for 3 + months and is present most days • Hypersensitivity to one’s own motion and to the movement of objects in the environment • Visual dizziness marked by exacerbation of symptoms in settings with complex visual stimuli (grocery stores) or when performing precision visual tasks (reading or working on the computer) |
102 | What are the treatment options for chronic subjective dizziness? | First-line pharmacologic therapy includes selective serotonin reuptake inhibitors. For patients with concurrent migraine, selective serotonin norepinephrine reuptake inhibitors or tricyclic antidepressants may be used. Behavioral intervention and psychoeducation serve as complementing therapies. |
103 | Describe the typical presentation of mal de débarquement syndrome. | The sensation of rocking or swaying back and forth without vertigo, difficulty concentrating, and fatigue. It most commonly occurs in middle-aged women after a week-long cruise. The mean duration of symptoms is 3.5 years. |
104 | What is the mechanism of motion sickness? | Disagreement between vestibular cues and visual and somatosensory input |
105 | Excluding benign paroxysmal positional vertigo, what is the most common cause of vertigo in the general population? | Vestibular migraine, or migraine-associated vertigo, is estimated to have a prevalence of ~ 1% in the general population. |
106 | What are the diagnostic criteria for vestibular migraine? | Definite vestibular migraine • Recurrent episodic vestibular symptoms of at least moderate severity • Current or previous history of migraine • Migrainous symptoms during ≥ 2 vertiginous attacks • Other causes ruled out by appropriate investigations Probable vestibular migraine • Recurrent episodic vestibular symptoms of at least moderate severity • One of the following:
|
107 | Describe the relationship between vestibular migraine and Ménière disease. | There is substantial overlap between groups. Approximately one-fourth of patients with Ménière disease also fulfill diagnostic criteria for vestibular migraine. |
108 | Describe the clinical features of basilar migraine. | • Similar symptoms to vertebrobasilar insufficiency with headache • Most patients experience dizziness but may also experience ataxia, hearing loss, tinnitus, dysarthria, diplopia, and syncope. • It most commonly involves young females. |
109 | Describe the common neurotologic examination findings in patients with multiple sclerosis. | Abnormalities of smooth pursuit (96%), saccadic eye movements (76%), optokinetic nystagmus (53%), and defective visual suppression of nystagmus (43%) |
110 | What is the Charcot triad? | Nystagmus, scanning speech, and intention tremor; associated symptoms of multiple sclerosis |
111 | Define balance retraining therapy. | Specialized form of physical therapy focusing on the improvement of static and dynamic balance and gait, and promoting central vestibular compensation by taking advantage of the inherent plasticity of central balance pathways |
112 | What are the two phases of vestibular recovery after an acute vestibular insult? | • Static recovery (initial phase) occurs through a central adaptive process that rebalances tonic neural activity between vestibular nuclei • Dynamic reco very (second phase) involves recalibrating brain and cerebellar reflex pathways in response to sensory conflicts occurring with head and eye movements. |
113 | Describe the clinical findings during static compensation and dynamic compensation. | During static compensation, patients will often have marked spontaneous nystagmus and vertigo lasting from days to weeks. During dynamic compensation, patients may experience general imbalance and unsteadiness with quick head turn. |
114 | With regard to vestibular rehabilitation, describe the strategy of adaptation. | Exercises aimed at improving vestibule-ocular response (VOR) gain. Initially, the patient is asked to view a stationary object while moving the head back and forth. The same exercise can be repeated but with the object moving in the opposite direction of head turn. This will strengthen gaze stability through improvement of the VOR response. |
115 | With regard to vestibular rehabilitation, describe the strategy of habituation. | Patients may be exposed to repetitive visual, vestibular, or motor exercises that are designed to provoke episodes of imbalance. With repetitive exposure, there is an attenuation or modification of the response. |
With regard to vestibular rehabilitation, describe the strategy of substitution. | Exercises designed to take advantage of alternate intact balance mechanisms (remaining vestibular function, visual input, somatosensory input) to compensate for specific balance system deficits | |
117 | Describe the ideal candidate for vestibular rehabilitation. | Patient with stable unilateral vestibular hypofunction who continues to feel general imbalance that is worsened by quick head movements |
118 | What patients are not good candidates for vestibular rehabilitation? | Central compensation requires consistent and predictable peripheral vestibular input; therefore, patients with unstable vestibular deficits (e.g., active Ménière disease, acute viral labyrinthitis) should not enter vestibular rehabilitation until their condition has stabilized. |
119 | Name several conditions that negatively influence the outcome of vestibular rehabilitation. | Coexisting conditions that affect balance may result in less optimal outcomes than in patients with isolated stable vestibular hypofunction. Examples include central nervous system disorders (stroke, multiple sclerosis, Parkinson disease), sensory neuropathy (diabetes, peripheral vascular disease), motor dysfunction, and patients with vestibular migraine, to name a few. |
120 | Which medications potentially retard progress during vestibular rehabilitation? | Anticonvulsants and sedating medications may prolong vestibular rehabilitation. Additionally, vestibular suppressive medications hinder initial static compensation. |
121 | To what does presbystasis refer? | Presbystasis refers to the general balance difficulties of elderly patients that is related to cumulative age-related decline in vestibular response, visual acuity, proprioception, and motor control. |
 Current or previous history of migraine
Current or previous history of migraine Migrainous symptoms during ≥ 2 attacks of vertigo
Migrainous symptoms during ≥ 2 attacks of vertigo Migraine precipitants before vertigo in more than 50% of attacks
Migraine precipitants before vertigo in more than 50% of attacks Response to migraine medications in more than 50% of attacks
Response to migraine medications in more than 50% of attacks Other causes are ruled out by appropriate investigations.
Other causes are ruled out by appropriate investigations.Hearing Loss Evaluation
122 | Name the four different subclasses of presbycusis. | • Sensory: Loss of sensory hair cells of the basal turn, resulting in a precipitous high-frequency SNHL and preserved speech discrimination • Neural: Loss of VIII nerve fibers where speech discrimination may be disproportionately affected • Metabolic: Caused by atrophy of the stria vascularis affecting all frequencies (flat audiogram); speech discrimination is frequently preserved • Mechanical: Caused by stiffening of the basilar membrane, resulting in a gradual down sloping SNHL with proportional loss of speech discrimination |
123 | Define mild, moderate, severe, and profound hearing loss. | • Mild = 26 to 40 dB • Moderate = 41 to 55 dB • Moderately severe = 56 to 70 dB • Severe = 71 to 90 dB • Profound > 90 dB |
124 | At what air-bone gap range is Rinne testing (512-Hz tuning fork) most reliable at detecting a conductive hearing loss? | Between 17 and 30 dB; any value lower or higher is more likely to produce a false negative result. |
125 | What is the usual air-bone gap seen with a maximal conductive hearing loss? | Roughly 60 dB |
126 | What is the interaural decibel difference required for a Weber examination to lateralize? | Sound should lateralize to the ear with the largest conductive loss or the side with the “better nerve”; a minimum of a 5 dB difference is needed. |
127 | Describe the reliability of bedside hearing screening. ( | Finger rub, watch-tick, whispered speech, Rinne test, and Weber test all carry a relatively good specificity (60 to 100%), but they have low sensitivity (< 50%). |
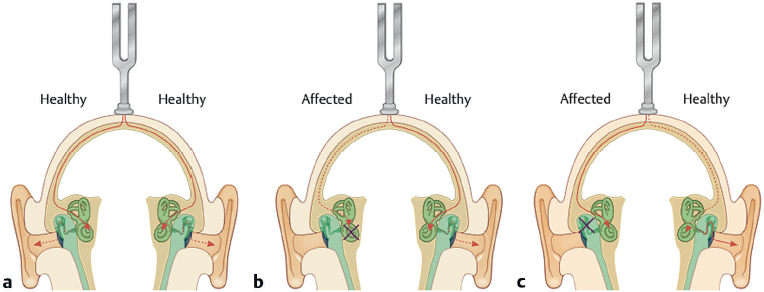
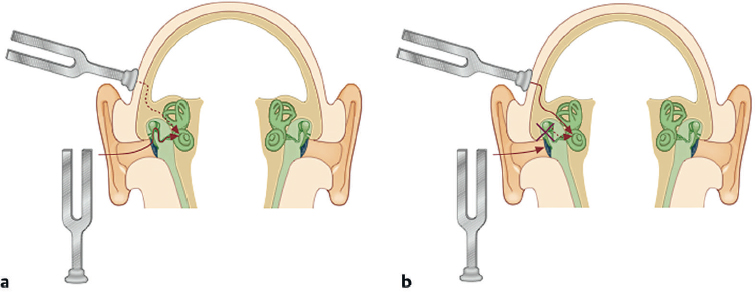
Fig. 6.4 The Rinne test. Using a vibrating tuning fork, air and bone conduction thresholds are compared in the same ear. (a) Without conductive hearing loss, air conduction is perceived louder than bone conduction. (b) With conductive hearing loss (usually greater than a 20 dB air-bone gap), bone conduction is perceived louder than air conduction. (Used with permission from Probst R, Grevers G, Iro H. Basic Otorhinolaryngology: A Step-by-Step Learning Guide. New York, NY: Thieme; 2006.)
128 | Define hearing level as it relates to measurement of sound intensity. | Hearing level is a measurement (in decibels) relative to reference data from normal-hearing ears. Normal sensitivitiy is defined as decibels of hearing level, which varies in absolute intensity at different frequencies because of different frequency sensitivities of the average healthy human ear. |
129 | Describe the anticipated test-retest variability seen with pure tone audiometry. | Test-retest variability should be 10 dB or less. |
Define asymmetric hearing loss. | Interaural differences of greater than 15 dB in two or more pure-tone thresholds or a difference of greater than 15% on speech discrimination testing | |
131 | What are the advantages of binaural hearing? | Horizontal plane sound localization and improved speech understanding in noise from summation, squelch, and head shadow effect |
132 | Describe two mechanisms that permit sound localization from an “off-center” source in the horizontal plane (left- or right-sided). | • Interaural time difference: Sound will reach the closest ear first (low-frequency dominated). • Interaural intensity difference: The intensity of sound in the ear farthest from the source will be attenuated by the head shadow effect (high-frequency dominated). |
133 | Why is masking used during audiometric testing? | If sounds presented to the test ear are sufficiently loud, they can cross over to the non-test ear. Interaural attenuation is the loss of intensity that occurs before arriving at the non-test ear. If sounds are loud enough to be perceived after interaural attenuation, masking is necessary to obtain an accurate test. Interaural attenuation for air conduction and bone conduction is roughly 40 dB and 0 dB, respectively. |
134 | In audiometric testing, what is meant by the term masking dilemma? | A masking dilemma occurs when the required masking level is loud enough to cross over to the test ear. This most commonly occurs in patients with significant bilateral conductive hearing loss. |
135 | Describe the phenomenon of recruitment. | Recruitment is characterized by minimal difficulty with quiet sounds but having a disproportionately severe noise sensitivity at higher sound levels. |
136 | Describe the phenomenon of rollover. | Rollover is characterized by a paradoxical decrease in speech recognition with increasing sound presentation levels and is associated with retrocochlear lesions. |
137 | What are appropriate ages to administer the different methods of behavioral audiometric testing in children? | • 0 to 5 months: Behavioral observation audiometry • 5 months to 2 years: Visual reinforcement audiometry • 2 to 5 years: Conditioned play audiometry • 5 + years: Conventional audiometry |
138 | Describe how behavioral observation audiometry is performed. | The tester evaluates for changes in patient behavior (e.g., quieting, eye widening, startle) after presentation of unconditioned sound. |
139 | Describe how visual reinforcement audiometry is performed. | The participant is conditioned to provide a specific response when he or she is able to hear a sound. For example, a child turns the head toward the sound source and a toy lights up to reward the behavior. |
140 | Describe how conditioned play audiometry is performed. | The participant is conditioned to perform a play activity (e.g., throw a ball, drop a block) when he or she is able to hear a sound. After the child has demonstrated that he or she understands the “game,” sound is presented at varying levels to determine frequency specific hearing thresholds and speech reponse threshold. |
141 | What physiologic process generates the auditory brainstem response? | Synchronized responses of specific neuron populations within the auditory pathway, with later waves corresponding to neuron groups farther down the transmission pathway: • Wave 1: Distal (lateral) auditory nerve • Wave 2: Proximal (medial) auditory nerve • Wave 3: Cochlear nucleus • Wave 4: Superior olivary complex • Wave 5: Lateral lemniscus/inferior colliculus |
Why is ABR testing useful in evaluating for retrocochlear pathology? | Abnormally long delays between waves (interpeak latency of Wave 1–5) suggest pathology, such as vestibular schwannoma, that is affecting the conductivity of the neurons that connect structures in the auditory pathway. | |
143 | What types of audiometry can be used for evaluation of congenital hearing loss in a 2-month-old infant? | Behavioral observation audiometry, ABR, and otoacoustic emissions |
144 | What are otoacoustic emissions? | Otoacoustic em issions are sound generated by outer hair cells, either spontaneously or evoked by an auditory stimulus, that can be detected by a microphone. They are considered a form of objective audiometry because they do not rely on patient participation. Generally, this type of testing is capable of detecting losses greater than 30 to 40 dB. |
145 | What is the advantage of distortion product otoacoustic emissions over transient evoked otoacoustic emissions? | They are capable of providing frequency specific information. |
146 | What ABR pattern is expected in children with auditory neuropathy? | Severely abnormal or absent ABR with a present cochlear microphonic and otoacoustic emission response |
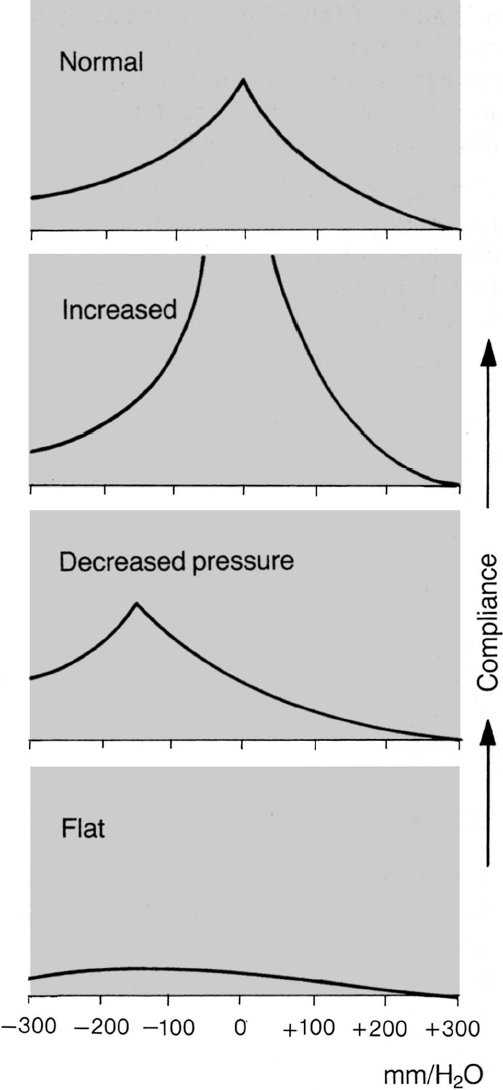
147 | Describe the following tympanometry patterns (modified Jerger classification): As, A, Ad, B, and C. ( | Tympanometry tests tympanic membrane (TM) compliance (admittance vs middle ear pressure). • Type A: Normal • Type As (shallow): Stiffened or hypomobile TM, ossicular fixation (e.g., otosclerosis, tympanosclerosis, malleus fixation), or “glue ear” • Type Ad (deep): Flaccid or hypermobile TM, ossicular discontinuity, or flaccid TM • Type B: Flat tracing with no compliance peak. Must combine with canal volume (normal child-adult 0.5 to 1.5 ml) • Type B (large volume): TM perforation or patent tympanostomy tube • Type B (normal volume): Middle ear fluid • Type B (small volume): Cerumen occlusion or probe against side wall of EAC • Type C: Left shift in peak (negative middle ear pressure) associated with eustachian tube dysfunction |
Describe how stapedial reflex testing is performed. | Tympanometry of the ipsilateral and contralateral tympanic membrane is measured when sound, typically between 80 to 110 dB hearing level, is applied to the ear at different frequencies (500, 1,000, 2,000, and 4,000 Hz). A stapedial reflex is measured as a decrease in compliance, resulting from stapedial muscle contraction. | |
149 | Describe conditions that may result in an absent or abnormal stapedial reflex. | Conductive hearing loss (e.g., otosclerosis, middle ear disease), severe SNHL, eighth nerve pathology (e.g., vestibular schwannoma), ipsilateral seventh nerve pathology (e.g., Bell palsy) |
150 | Describe the pattern of stapedial reflex testing seen with right-sided retrocochlear pathology. | • The reflexes are always absent when stimulated in the ipsilateral ear. • Left-sided stimulus: Left response present, right response present • Right-sided stimulus: Left response absent/elevated, right response absent/elevated |
151 | Describe the stapedial reflex pattern seen with a thick mucoid effusion in the right ear (type B tympanogram) causing a large conductive hearing loss. | • Middle ear effusion can result in dampening of the incoming auditory signal. Also, stapedial reflex detection can be impaired from decreased tympanic membrane compliance. • Left-sided stimulus: Left response present, right response absent/elevated • Right-sided stimulus: Left response absent/elevated, right response absent/elevated |
152 | Describe the stapedial reflex pattern seen with bilateral thick middle ear mucoid effusions (type B tympanogram) causing significant conductive hearing loss. |



