Otitis Media with Effusion
Otitis media with effusion (OME) is one of the most common chronic conditions of childhood. The primary complications of OME are (1) conductive hearing loss; (2) recurrent acute otitis media; and (3) middle ear atelectasis and cholesteatoma formation.
1-1 Myringotomy and Tube Placement
Indications
Myringotomy and tube placement is indicated (1) when fluid has been present for 8 to 12 weeks, despite medical therapy, causing a significant conductive hearing loss; (2) when recurrent acute otitis is debilitating by its frequency and severity; or (3) when tympanic membrane retraction is present to a degree that one suspects potentially imminent development of ossicular erosion, cholesteatoma, or atelectasis.
Preoperative Evaluation
The preoperative evaluation requires a complete pneumatic otoscopic examination and audiologic evaluation. Radiography is rarely, if ever, helpful.
Operative Technique
1. General anesthesia is usually administered by mask. The head is turned to the side opposite the ear being operated upon.
2. The largest speculum that will fit in the external meatus is placed in the ear. Wax is cleared from the external meatus to provide visualization of the entire tympanic membrane.
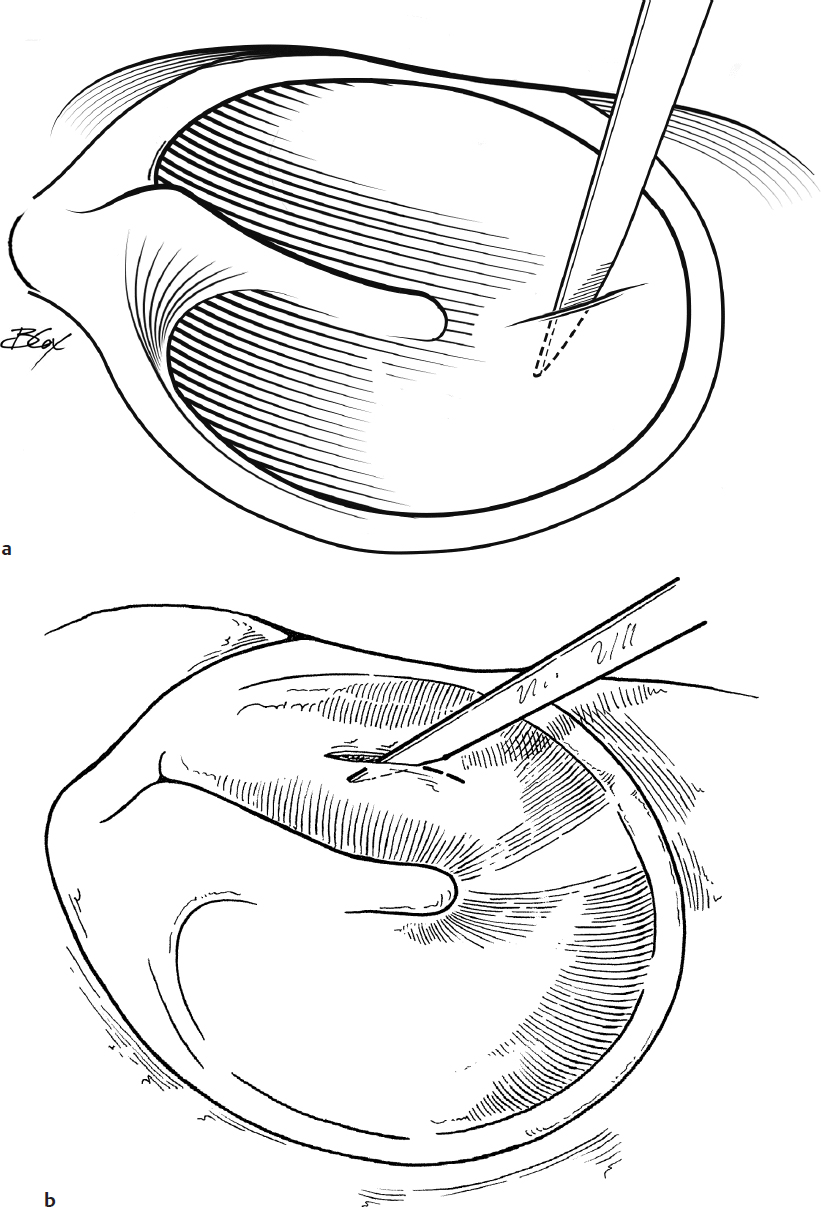
3. A radial (Fig. 1.1a) or circumferential (Fig. 1.1b) incision is made through the ear drum. Choice and site of incisions depend on surgeon preference and exposure obtained. For example, if there is a prominent anterior bony ear canal, a radial incision placed in the inferior quadrant is more easily performed.
4. Fluid is aspirated from the middle ear with a 5-French suction cannula, preferably without touching the tympanic membrane.
5. The anterior medial flange of the tube is inserted in the incision, and the posterior flange is rotated into the incision with an alligator forceps or suction tip (Fig. 1.1c,d,e).
6. The lumen and area around the tube are aspirated free of blood. Oxymetazoline or antibiotic-containing ear (or eye) drops can be placed in the ear to prevent reaccumulation of blood and subsequent plugging of the tube.
7. Large-flanged or T tubes are used in patients in whom standard tubes extrude prematurely or in those instances where it is felt that a child will need 3 to 5 years of middle ear ventilation. These tubes can be placed in a fashion similar to that used when inserting standard tubes, except that they require a larger myringotomy incision (Fig. 1.1f,g). Some surgeons prefer subannular tube placement in order to facilitate long-term ventilation. In this technique, a tympanomeatal flap is elevated after incising the ear canal approximately 5 mm lateral to the annulus and lifting the posterior inferior annulus from the tympanic ring (Fig. 1.1h,i). A T tube is placed through the incision taking care to avoid the ossicles with its two legs, and the flap is placed over the tube (Fig. 1.1j). The flap can be held in position with a small amount of Gelfoam (Pfizer) (or antibiotic-containing ointment).
Complications
1. Purulent otorrhea
2. Early extrusion
3. Permanent perforation
4. Granuloma
5. Tympanosclerosis
6. Cholesteatoma