21 Other Disorders of the Otic Capsule
Most of these disorders unlike otosclerosis will involve the otic capsule and other areas of the temporal bone. Furthermore, other bones of the human skeleton can be involved. It is interesting to know that they can present as conductive deafness and the audiometric configuration can resemble that of otosclerosis.
Osteogenesis Imperfecta
Osteogenesis imperfecta (OI) is a disease of connective tissue with the main feature of bone fractures after trivial trauma. It is accompanied by blue sclera and hearing loss. Hearing loss affects approximately 50% of the patients beginning in the second and third decades of life. Hearing loss initially starts as a conductive hearing loss and then progresses as a mixed hearing loss and further progresses as a sensorineural hearing loss. OI resembles otosclerosis in many ways. OI is a genetic disease involving connective tissue localized to chromosome 17 with both autosomal dominant and autosomal recessive inheritance. It is because of a mutation in genes that encode for procollagen.
Incidence
Its incidence varies between 2 and 15 per 100,000 births.1 It is a hereditary disorder of collagen synthesis and occurs in two main forms: osteogenesis imperfecta congenital and osteogenesis imperfecta tarda (OIT). In the congenital form, fractures occur in utero and the fetus dies in utero. In the tarda form, fractures often occur after minor trivial trauma during childhood. This however becomes less frequent with the onset of adolescence. Malalignment of the fractured bones leads to deformities and excessive callus formation. OIT has a dominant mode of inheritance with variable penetrance with asymptomatic carriers. Sporadic cases without a family history of OIT are known to occur.
Signs and Symptoms
The cardinal features of this disease are fractures that occur after relatively minor trivial often unrecognized trauma. Approximately 50 to 60% of these patients eventually develop a hearing loss. Many patients (approximately 85%) have blue sclera.2 However, blue sclerae are associated with collagen disorders such as Ehlers-Danlos syndrome and Marfan syndrome.
The syndrome in which multiple fractures, blue sclerae, and deafness occurs is known as Van der Hoeve-de Kleyn syndrome. However, it was also noticed that in some family members hearing impairment and blue sclerae presented without the tendency for fractures.
Altered collagen synthesis results in defective connective tissue with a tendency to hypermobility and laxity of joints, thin skin, and easy bruising in the subcutaneous tissues. The teeth of these patients are abnormal in approximately 15% of such patients. The dentine is abnormal; the enamel is cracked, resulting in yellow-stained irregular teeth. This was known as amelogenesis imperfecta.
The clinical course of OIT is variable. Sillence et al introduced a classification based on genetic and clinical criteria.3
OI has been classified into six different types according to severity discussed at the International Conference on OI Annecy, 2002.4
1. Type I A/B: mild to severe bone fragility, blue sclerae, and dentinogenesis imperfecta
2. Type II: lethal
3. Type III: severe bone fragility (long bones affected) and blue sclerae
4. Type IV A/B: bone fragility and mild to moderate deformity
5. Type V: hyperplastic callus formation and white sclerae
6. Type VI: vertebral fractures, bone fragility, and light blue sclerae
Types I and III are the most common. The typical features of this disease are as follows:
• Bone fragility
• Short stature
• Secondary deformities (bowed limbs and kyphoscoliosis)
• Other manifestations of collagen-containing tissue
• Blue sclerae
• Dentinogenesis imperfecta (fragility of teeth because of poor mineralization of dentine)
• Hearing loss (> 50% mostly in OI type I and type III)
• Vertigo
Otological Features
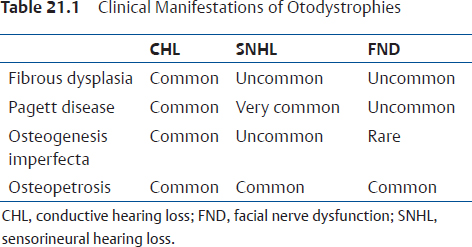
The otological features of OI are summarized in Table 21.1. Hearing loss has long been recognized as a common feature in OI. The figure in some publications could be taken to imply that with advancing age the number of patients suffering from OI could approach 100%. The typical feature of OI is hearing loss, which typically occurs in childhood and then rapidly progresses. The incidence of deafness in childhood is between 10 and 20%; by middle age approximately 50% of the patients suffering from OI will be suffering from deafness. The hearing loss may increase during pregnancy. The audiometric pattern of hearing loss is indistinguishable from that of otosclerosis. Typically the hearing loss commences at puberty when fractures become less frequent. A conductive hearing loss is present in nearly 80% of the cases. Very often a mixed hearing loss is present. On occasion, a purely sensorineural hearing loss may be present, and on rare occasions, profound irreversible sensorineural hearing loss may be present.5 Sensorineural hearing loss in OIT is believed to be because of encroachment of reparative vascular and fibrous tissue in and about the cochlea or as the result of microfractures and/or hemorrhages. Several studies have indicated that the incidence of hearing loss of both types rises with age as does the proportion of patients with mixed types. Some studies have implied that with advancing age the proportion of patients with hearing loss approaches 100%. In one study, 11 of 12 patients between 40 and 49 years of age were affected as were all 7 patients between 50 and 55 years of age.5
In a study involving 1394 patients with OI, the most common age of onset was from the second to the fourth decade of life.6 They found that at the age of 50 years, approximately 50% of the patients in their series had symptoms of hearing impairment.
Tympanometry shows increased compliance values. Stapes fixation is almost always associated with a conductive hearing loss. Hypermobility of the tympanic membrane can be seen simultaneously with fractures or aplasia of the crura of the stapes. Hypermobility of the tympanic membrane occurs because the tympanic membrane has the same embryological origin as the sclera. In patients who have fractures of the stapedial arch, high compliance values are seen on tympanometry. Carhart notches are not present; Schwartz sign is also not present. Usually the conductive hearing losses are not bilateral, but if and when bilateral conductive hearing losses are present they are not symmetrical. Vestibular symptoms are rare in OI. However, Johnsson et al described extensive bilateral endolymphatic hydrops in a patient who suffered from OI.7
Histology
Deposition of osteopenic immature bony tissue that is weak is characteristic of OI. Often, microfractures can be found. Histologically, the number of osteocytes is increased in both woven and lamellar bone accompanied by a relative reduction of matrix substance. The bone turnover rate is very high. OIT has multiorgan manifestations such as fragile bones, hearing loss, dentinogenesis imperfecta, loose joints, mitral valve prolapse, easy bruising, and growth deficiency. Histologically, while there are some similarities between otosclerosis and OI, both are separate and distinct entities with defects in the stapes as seen in OI being quite different from those seen in otosclerosis.8,9 Biochemical analysis of stapes sulfhydryl groups and various enzymes have clearly demonstrated different concentrations between both these diseases.10 In a majority of cases, stapedial fixation is because of a focal lesion in the footplate, which histologically resembles the early active stage of otosclerosis. On occasion, fixation of the stapedial footplate is the result of diffuse structural alteration of the entire footplate. The extensive degree of disorganization is more pronounced in OI than is seen in otosclerosis.11
Biochemical assays of serum calcium, phosphorous, and calciferol are normal. Alkaline phosphatase levels may occasionally be elevated. Photon absorptiometry has demonstrated that the cortical thickness of bone is reduced. This is not seen in otosclerosis.
Radiological Findings
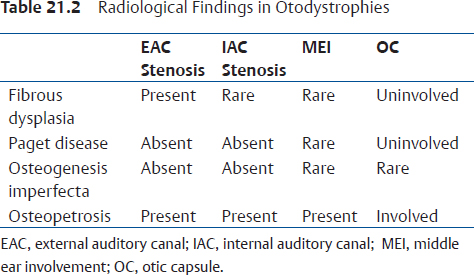
Temporal bone findings in OIT are nearly identical to those of otosclerosis (Table 21.2). Diffuse resorption of vast areas of the otic capsule is commonly seen in OIT. In advanced cases of OIT, the middle ear cleft can get narrowed by proliferative bone and the oval and round windows can get obliterated by the dysplastic process.
Treatment
At this time, there is no known cure for OIT. Treatment is directed at rehabilitation. Medical treatment for OIT remains elusive. Calcitonin, sodium fluoride, and vitamin D have all been found not to be very efficacious.
Role of Stapedectomy
Results of stapedectomy are generally satisfactory.12 Results of stapedectomy are similar to that of those in otosclerosis.13 However, stapedectomy should be delayed until well into adulthood.14 By then, it is expected that fractures in response to trivial trauma will have ceased.15 The findings of the middle ear include a very thick and soft footplate. The middle ear mucosa appears to be more vascular than normal. There is a high chance of floating footplate. The long process of the incus may be fragile and prone to fracture during crimping. Other findings include thin canal wall skin, brittle scutum, and fragile stapedial crura.
Paget Disease (Osteitis Deformans)
Paget disease is characterized by excessive remodeling of bone. This disorder typically affects the axial skeleton. Pathognomonic features of this disease are spreading osteolytic and osteoblastic changes that commonly affect the pelvis, lumbar spine, skull, femur, and tibia. The typical appearance of a patient suffering from Paget disease would be characterized by an enlarged skull, progressive kyphosis, bowed legs, and short stature.
Incidence
Males are four times more likely to be affected than females. The geographic distribution of Paget disease includes a large concentration of patients in the United Kingdom, Australia, and New Zealand.16
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


