Orbital Fracture
Direct trauma to the eye may transmit force to the floor of the orbit causing multiple fractures in the floor while the orbital rim remains intact. Herniation of fat and muscle through the bony defect may cause a restriction of upward gaze and resultant diplopia. It is necessary to have a high index of suspicion of orbital injury in children as they can often present white-eyed. Specifically, they may not have significant ecchymosis, edema, orbital rim step-off, or conjunctival hemorrhage.
Surgery should be performed within 48 hours and can lead to improvement of associated nausea, vomiting, and bradycardia, which is mediated by the oculocardiac reflex.
40-1 Treatment of Orbital Floor Fractures
Indications
Presence of an orbital floor fracture with enophthalmos and/or restriction of ocular mobility are indications for surgical exploration. Large floor defects > 1 cm2 or 50% or more of the orbital floor are also an indication for repair as they will likely result in enophthalmos if uncorrected.
Medial orbital wall and orbital roof fractures are less common than orbital floor fractures but more proportionately common in children due to underpneumatized sinuses. These can be observed as long as entrapment, diplopia, enophthalmos, and a cerebrospinal fluid leak are not present.
Preoperative Evaluation
A careful examination of the eye to rule out ocular injury (e.g., hyphema) is essential. Plain radiographs may demonstrate the herniated orbital contents extending through the fracture into the maxillary sinus. However, pediatric low-dose radiation computed tomography (CT) provides the best definition of the fracture. Ophthalmology consultation is indicated prior to surgical intervention for evaluating visual acuity and trauma to the globe.
Operative Technique
1. Orbital floor fractures are best reduced utilizing general anesthesia.
2. Corneal protection must be employed by performing a tarsorrhaphy suture with a 6-0 nylon or Prolene suture (Ethicon) through the gray line of the lid margins.
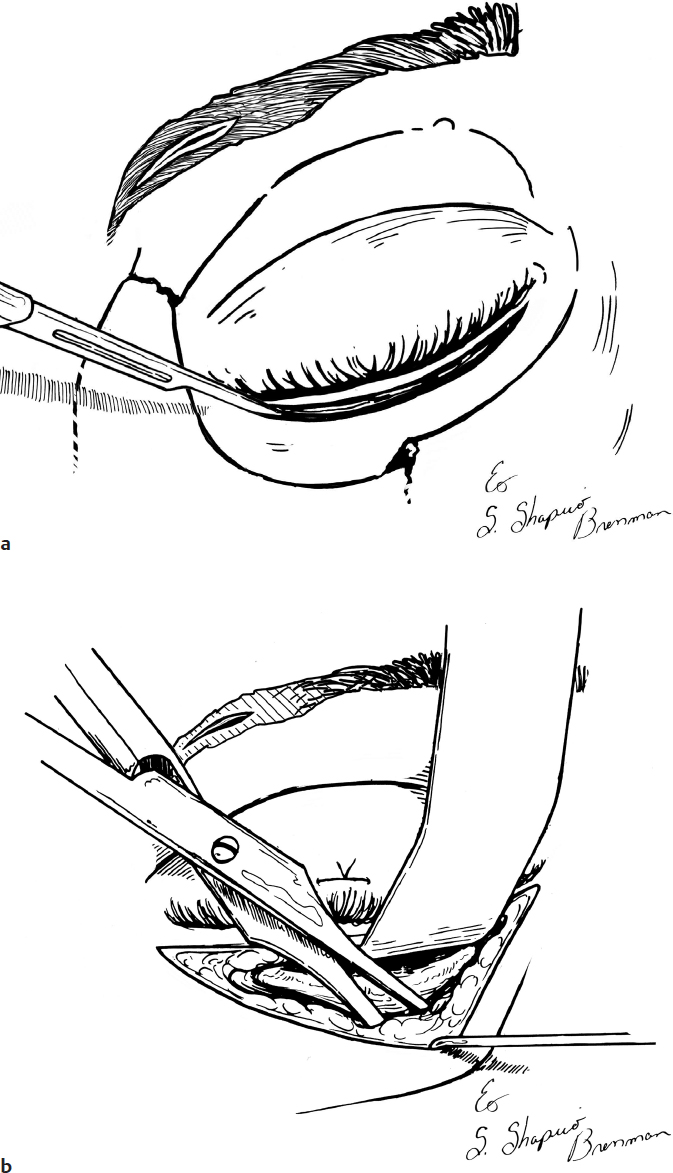
3. For a subciliary approach, an incision is made through the skin just below the lash line after 1% lidocaine with 1:100,000 epinephrine is injected at the incision site to aid in hemostasis (Fig. 40.1a).
4. A dissection plane is developed with scissors inferior from the incision between the skin and the pretarsal portion of the orbicularis oculi just deep to it. This exposes the pretarsal and then the preseptal portions of the orbicularis oculi muscle (Fig. 40.1b).
5. Between the pretarsal and the preseptal portions of the muscle, a plane is dissected and carried inferiorly deep to the preseptal portion of the orbicularis oculi muscle. This dissection plane is between the preseptal portion of the orbicularis oculi muscle and the orbital septum. This is followed down onto the infraorbital rim (Fig. 40.1c).
6. Once the infraorbital rim is identified, the periosteum over the infraorbital rim can be incised sharply and the fracture can be visualized (Fig. 40.1d).
7. Alternatively, a transconjunctival approach can be performed instead of a subciliary approach (not shown).
8. Orbital fat and muscle entrapped in the fracture are released with an elevator (Fig. 40.1e).
9. The depressed fracture fragments are lifted with an elevator (Fig. 40.1f).
10. A bone graft, titanium mesh, resorbable sheets, or highdensity porous polyethylene implant is inserted along the orbital floor to protect the fractures and prevent reherniation of orbital contents (Fig. 40.1g).
11. Following repair, forced duction test should be performed to ensure that the implant is not causing any entrapment.
12. The incision is closed with 4-0 or 5-0 interrupted Vicryl sutures in the periosteum. The subciliary skin incision is closed with a 5-0 or 6-0 interrupted or running fast-absorbing gut suture (Fig. 40.1h).
Complications
1. Persistent diplopia
2. Enophthalmos
3. Wound infection
4. Hardware failure
5. Osteomyelitis
6. Ectropion/entropion