Key points
- •
Orbital injuries are rare but potentially catastrophic complications of sinus surgery.
- •
Sinus surgeons must be able to recognize anatomy and disease predisposing to orbital injury and learn how to avoid them.
- •
The eye must always be included in the surgical field and frequently inspected and palpated.
- •
Sinus surgeons should be able to recognize orbital complications early and be able capable of emergent medical and surgical management of orbital hemorrhage.
- •
Sinus surgeons must become facile with performing lateral canthotomy-cantholysis and endoscopic orbital decompression for emergent management of an expanding retrobulbar hematoma.
| AEA | Anterior ethmoidal artery |
| APD | Afferent pupillary defect |
| CRS | Chronic rhinosinusitis |
| CT | Computed tomographic |
| EOM | Extraocular muscle |
| ESS | Endoscopic sinus surgery |
| IGS | Image guidance systems |
| IOP | Intraocular pressure |
| NLD | Nasolacrimal duct |
| PEA | Posterior ethmoidal artery |
Introduction
Although rare, catastrophic orbital complications can result from interventions to treat chronic rhinosinusitis (CRS). The orbit, orbital apex, and optic canal lie in intimate relationship to the maxillary, ethmoidal, frontal, and sphenoid sinuses and are vulnerable to injury during endoscopic sinus surgery (ESS). The lamina papyracea, orbital floor and roof, orbital fat, extraocular muscles (EOMs), anterior ethmoidal artery (AEA) and posterior ethmoidal artery (PEA), lacrimal drainage system, and the infraorbital nerve can be injured during ESS, resulting in blindness, diplopia, orbital hemorrhage, retro-orbital hematoma, enophthalmos, orbital emphysema, nasolacrimal duct (NLD) injury, and infraorbital nerve numbness.
This article reviews strategies in the prevention and management of orbital complications from ESS. The authors focus on the relevant orbital anatomy and pathophysiologic mechanisms of injury and offer practical advice on management. A succinct summary of orbital complications resulting from medical therapy for CRS is also presented.
Introduction
Although rare, catastrophic orbital complications can result from interventions to treat chronic rhinosinusitis (CRS). The orbit, orbital apex, and optic canal lie in intimate relationship to the maxillary, ethmoidal, frontal, and sphenoid sinuses and are vulnerable to injury during endoscopic sinus surgery (ESS). The lamina papyracea, orbital floor and roof, orbital fat, extraocular muscles (EOMs), anterior ethmoidal artery (AEA) and posterior ethmoidal artery (PEA), lacrimal drainage system, and the infraorbital nerve can be injured during ESS, resulting in blindness, diplopia, orbital hemorrhage, retro-orbital hematoma, enophthalmos, orbital emphysema, nasolacrimal duct (NLD) injury, and infraorbital nerve numbness.
This article reviews strategies in the prevention and management of orbital complications from ESS. The authors focus on the relevant orbital anatomy and pathophysiologic mechanisms of injury and offer practical advice on management. A succinct summary of orbital complications resulting from medical therapy for CRS is also presented.
Incidence of orbital complications in endoscopic sinus surgery
A recent database analysis of nearly 80,000 patients found orbital complications to occur in 0.23% of primary ESS and 0.29% of revision ESS procedures. The rate of orbital complications was not significantly different between primary and revision ESS. A previous nationwide database study on 62,823 patients who underwent ESS in the United States between 2003 and 2007 found orbital injury to occur in 0.07% of patients. Orbital injury was more likely to occur in children younger than 12 years ( P <.001). Orbital hematoma occurred in 0.15%, orbital penetration and fat exposure in 2.1%, and diplopia (either temporary or permanent) in 0.3%. These studies looked for reports of diplopia, paralytic strabismus, optic nerve injury, epiphora, orbital hemorrhage, or blindness/visual disturbance. In addition, a patient was considered to have an orbital complication if canthotomy/canthoplasty, strabismus surgery, or orbital decompression was performed in the same time frame. In both studies, it was noted that the incidence of reported orbital injuries declined when compared with that in earlier decades. In their recent publication, Stankiewicz and colleagues reviewed their patients who underwent ESS in the past 25 years and found an orbital complication rate of 0.7% in 3402 patients.
Avoidance of orbital complications
Preoperative Planning
It is extremely important that the ESS surgeon conduct a thorough review of the patient’s anatomy and pathology before undertaking surgery. The patient’s history of prior ESS and facial trauma should be elicited, because these may be associated with anatomic abnormalities. The medication profile and other potential risks of hemorrhage should be ascertained. The endoscopic examination should carefully judge whether the disease or prior surgery could potentially compromise visualization of landmarks during ESS. The sinus computed tomographic (CT) scan should be carefully studied, and this scan must always be available for intraoperative review. The surgeon should schedule surgery only if it is in the planned surgical procedure and if they have the tools required for such procedure such as image guidance systems (IGS) and powered and handheld instrumentation. Surgeons should be aware of the limitations of their expertise and technology. For example, although IGS been advocated for those with complex anatomy, polyps, tumors, frontal and sphenoid sinusotomy, and revision surgery, its use may not necessarily prevent orbital complications. Novice surgeons must be carefully proctored; they must practice dissection on cadaver specimens first, because ESS has a steep learning curve. However, constant vigilance by even the experienced sinus surgeon is mandated.
Intraoperative Considerations
The eyes must always be draped into the field and should not be covered but taped with a paper or transparent tape. Intraoperatively, the surgeon should consistently inspect and palpate the eyeball, especially when working close to the lamina papyracea or skull base. Assistants should be educated and encouraged to communicate urgently should they notice any orbital proptosis while the surgeon’s view is focused on the endoscopic monitor. Surgery should be terminated if visualization is unsatisfactory and bleeding cannot be controlled. The surgeon should be familiar with the higher risk of orbital injury associated with powered instrumentation. Powered instrumentation such as microdebriders should be used only when the cutting edge can be clearly visualized endoscopically. These instruments should be used parallel to the lamina papyracea and not push toward the orbit. Intraoperative image guidance should be carefully calibrated, and adjustments to errors of calibration should be constantly made during ESS in conjunction with the surgeon’s understanding of the relevant anatomy.
Computed Tomographic Review
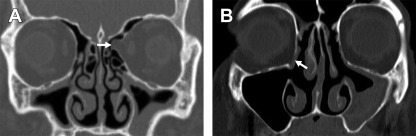
The surgeon must develop a systematic manner of reviewing CT scans to identify those with higher risk of orbital injury. The authors provide a suggested checklist ( Table 1 ). Orbital anatomy in relationship to the paranasal sinuses must be conducted in all 3 planes. Subtle protrusion of the orbit or orbital contents into the ethmoidal space may be better recognized on axial scans. Any dehiscence or thinning of the lamina papyracea must prompt closer evaluation because prolapsed orbital contents may be mistaken for a polyp or inflammatory sinus mucosa ( Fig. 1 ). Presence of pathologic conditions such as mucocele or polyposis expanding or eroding into the orbit must be identified.
| CT Finding | Clinical Implications for Orbital Safety |
|---|---|
| Sinus disease | Pansinusitis: need for more extensive dissection during ESS |
| Nasal polyposis: anatomy obscured because of disease and prior surgery | |
| Mucocele: erosion into the orbit is likely | |
| |
| |
| Lamina papyracea |
|
| |
| Skull base |
|
| Maxillary sinus |
|
| Ethmoidal sinus | Hypoplasia: lamina papyracea is more medial and at risk of injury |
| Infraorbital (Haller) cell: infraorbital nerve at risk at dissection | |
| Sphenoethmoid (Onodi) cell: optic nerve, internal carotid artery at risk | |
| |
| Sphenoid sinus |
|
The maxillary ostium usually lies in the same parasagittal plane of the medial wall of the orbit, but when the lamina papyracea is positioned medial to the maxillary ostium owing to hypoplasia of the ethmoidal cells, there is higher risk of orbital penetration during ESS ( Fig. 2 ). When the maxillary sinus is hypoplastic, the uncinate is usually hypoplastic or laterally displaced over the orbit, predisposing the patient to orbital penetration during ESS. A similar situation exists in those with the silent sinus syndrome when both the lamina papyracea and the orbital floor are at risk of injury ( Fig. 3 ). In this situation, one should be prepared to use handheld instruments as opposed to powered microdebriders. Retrograde uncinectomy technique here may be safer compared with anterograde uncinectomy with a sickle knife.
The position of the AEA and the PEA must be located on the scans. These arteries are branches of the ophthalmic artery and leave the orbit between the medial rectus and superior oblique muscles within the ethmoidal skull base. The AEA travels within a bony mesentery below the level of the skull base in up to 36% of cases, with a dehiscence rate ranging from 6% to 66%. A long lateral lamella or the presence of supraorbital pneumatization is associated with a low-hanging AEA. The AEA is considered to be the posterior boundary of the frontal recess and lies close to the attachment of the middle turbinate basal lamella at the skull base, whereas the PEA lies in the ethmoidal skull base just anterior to the face of the sphenoid sinus ( Fig. 4 ). An injured ethmoidal artery may retract into the orbital cavity and cause a rapidly expanding retrobulbar hematoma that can result in blindness if not quickly recognized.
In addition, one must recognize and be familiar with implications of variations of ethmoidal pneumatization. The sphenoethmoidal (Onodi) cell may be related to the optic nerve and even the internal carotid artery in its lateral wall. The surgeon therefore encounters these structures during ethmoidectomy, before undertaking sphenoidotomy. Not recognizing this variation may thus result in catastrophic injury, especially when extensive disease or polyposis obscures the anatomy. The optic nerve may be dehiscent in the lateral sphenoid sinus or lie in the Onodi cells in approximately 3.4% to 14% of cases ( Fig. 5 ). The optic canal can travel through a well-pneumatized sphenoid in 3% cases and may be mistaken for a partition if the CT is not carefully reviewed ( Fig. 6 ). The infraorbital nerve lies just lateral to an infraorbital (Haller) cell and may be injured while addressing this cell ( Fig. 7 ). Higher frontoethmoid dissection in the presence of Type 3 or Type 4 frontal cells may also place at risk the superior orbital contents, including the superior oblique muscle.
Postoperative Considerations
All patients must be counseled to watch and report immediately any changes in vision, color vision, double vision, eye pain, watering from the eye, bruising, and emphysema. Should any orbital injury during surgery be recognized, the patients should be advised of it and be placed on the appropriate therapeutic interventions as discussed in the following section.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


