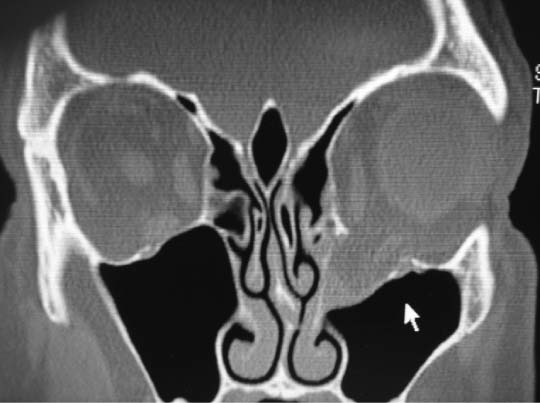
82 The patient is a 45-year-old man involved in a motor vehicle collision who presents with double vision and pain with eye movements. He reported that he was struck in the left peri-orbital area. He denied loss of consciousness. Subjectively, he had no difficulty seeing out of the eye but noted that his cheek was numb on the left side. He was otherwise healthy, with no medical or ocular history. Physical examination showed a healthy-appearing man with periorbital ecchymosis. Pupil examination and vision were normal in both eyes. Significant diplopia was present in upgaze, and he complained of mild pain with eye movements. On the left, motility was limited in upgaze only and enophthalmos was present. The left eye also appeared lower compared with the right (Figs. 82.1 and 82.2). Fig. 82.1 A 45-year-old man with restriction of superior gaze following left periorbital trauma. 1. When evaluating patients with orbital and facial trauma, the more serious injuries need to be ruled out first, such as airway, breathing, circulation intracranial injury, and vision-threatening problems. The patient had no loss of consciousness with the injury and had a normal neurologic examination. The other major concern would be ruling out an injury to the globe. Fig. 82.2 Coronal computed tomography scan showing left orbital floor fracture and prolapse of orbital soft tissue. 2. The entire injury appears to be localized to the periorbital area, and the extent of the injury cannot be fully determined on external appearance alone. The motility examination indicates that extraocular muscles may be impinged or paretic, possibly from an orbital fracture. Also, the globe is sunken down and back relative to the right eye, which is consistent with a significant floor fracture. It is important to consider the surrounding facial structures for injury when an orbital fracture is present, namely, a zygomatic complex fracture or other facial fractures. The orbital rims should be palpated for tenderness and step-offs, as should the malar eminence. Any malpositions or depressions in comparison to the normal side by the supra vertex and submental views should be noted. 3. Cheek and lip numbness can also indicate that an orbital floor fracture is present given that the infraorbital nerve runs along the floor. It is often involved and may be the only sign of a fracture on the examination. These should be evaluated and documented in trauma patients. 4. A significant eye injury occurs in one third of patients with orbital fractures, and a dilated fundoscopic examination by an ophthalmologist is recommended. A vital diagnostic test is a thorough ophthalmic evaluation to rule out globe injury. Corneal abrasions, hyphema, lens dislocation, retinal detachment, and rupture of the globe are among the injuries that should be ruled out with dilated examination. Delay in diagnosing severe eye problems may result in loss of vision; thus ophthalmologic consultation in a timely fashion is recommended. High-resolution computed tomography (CT) imaging (axial and coronal views) provides the best information for evaluating orbital bones in relation to the soft tissues and orbital fat. When fractures are identified, herniation of orbital contents into the surrounding sinuses can lead to extraocular muscle entrapment within or below the bony fragments. In this case there was an isolated orbital floor blowout fracture and the surrounding bones were intact, but the inferior rectus muscle was adjacent to the edge of the fracture. An important part of the examination in patients with orbital fractures is forced duction testing. If it is unclear whether the muscle is entrapped, the insertion of the muscle can be grasped with a fine forceps with the aid of a topical anesthetic, and the globe is rotated. Severe restriction indicates that the muscle is entrapped and needs to be released surgically. This patient had limited upgaze but normal forced duction testing, and thus the limited motility was likely as a result of edema and hemorrhage.
Orbital Blowout Fracture
History

Differential Diagnosis—Key Points
Test Interpretation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


