Pathology affecting the orbit and orbital apex is diverse and heterogeneous. Many of the differential pathologies require management in a multidisciplinary team involving both otolaryngology and ophthalmology. This article discusses the differential pathologies. Emphasis has been placed on Graves orbitopathy, traumatic optic neuropathy, and the indications for decompression in each. The differential diagnosis for a lesion within the orbit and orbital apex is diverse. The presentation, investigation, and appropriate management of these conditions is discussed with emphasis on traumatic optic neuropathy and Graves orbitopathy.
| EBM Question | Level of Evidence | Grade of Recommendation |
|---|---|---|
| Does vision improve following decompression of traumatic and tumor pathology? | 2b | B |
| What is optimal timing of endoscopic decompression? | 4 | C |
Pathology affecting the orbit and orbital apex is diverse and heterogeneous. Many of the differential pathologies require management in a multidisciplinary team involving both otolaryngology and ophthalmology. This article discusses the differential pathologies. Emphasis has been placed on Graves orbitopathy (GO), traumatic optic neuropathy (TON), and the indications for decompression in each. The differential diagnosis for a lesion within the orbit and orbital apex is diverse ( Box 1 ). The presentation, investigation, and appropriate management of these conditions is discussed with emphasis on TON and GO.
- •
Infectious
- ○
Bacterial
- ○
Fungal
- ○
- •
Inflammatory
- ○
GO
- ○
Idiopathic orbital inflammation
- ○
Granulomatous
- ○
- •
Traumatic
- •
Neoplastic benign
- ○
Vascular
- ○
Neural
- ○
Fibro-osseous
- ○
- •
Neoplastic malignant
- ○
Lymphoma
- ○
Epithelial
- ○
Nonepithelial
- ○
Secondary
- ○
Infectious sinusitis
Bacterial
Bacterial infections of the orbit are classified by the Chandler classification. Any infection that is Chandler classification 4 or more, which is within the orbit, requires prompt surgical drainage. The treatment for Chandler classification 3, which is a subperiosteal abscess, is more controversial with some investigators advocating a trial of medical therapy before offering surgery.
Investigations
All patients with a suspected subperiosteal abscess should have a CT scan with contrast of their paranasal sinuses to confirm the diagnosis and to visualize the anatomy of the sinuses. If it is suspected the patient has intracranial complications, they should proceed to having an MRI scan.
Organisms most commonly found in subperiosteal abscess are Streptococci , Staphylococci , and Bacteroides .
Treatment
All patients with an orbital complication of sinusitis require antibiotics. The authors propose the use of a third-generation cephalosporin and an antistaphylococcal agent. The controversial decision is whether the patient needs to have surgical drainage of their abscess and the proposed timing of surgery.
The authors use Garcia and Harris criteria for a trial of nonsurgical management. The criteria that must be satisfied are:
- •
Age of patient less than 9 years old
- •
No visual compromise
- •
Medial abscess of modest or small size
- •
No intracranial or frontal sinus involvement.
If these criteria are not met, the patient requires drainage with endoscopic as the preferred method. The use of age as a requirement for consideration for drainage is because patients over age 9 years have an increased incidence of infections that are refractory to antibiotics.
The authors advocate that if an endonasal approach to medial subperiosteal abscess is not possible, drainage should be performed using a transcaruncular approach rather than a Lynch incision. This approach is typically performed by an ophthalmologist with oculoplastic training. It has the advantage over the Lynch incision of gaining more linearly direct access to the medial subperiosteal space, avoiding a skin incision and resulting scar, as well as avoiding injury to the adjacent trochlear and superior oblique attachment.
If the patient worsens clinically, they are given prompt surgical drainage.
Fungal Sinusitis
Fungal sinusitis can be subdivided into invasive and noninvasive fungal sinusitis. Invasive fungal sinusitis requires prompt aggressive surgical debridement. Noninvasive fungal sinusitis that has developed an orbital complication can be initially treated medically before surgical drainage. The details of the diagnosis and treatment modalities of fungal sinusitis are beyond the scope of this paper.
Inflammatory diseases of the orbit
GO
GO is the most common extrathyroidal manifestation of Graves disease. Although GO occurs in Graves disease, it may also manifest in patients who have no history of Graves disease, patients who are euthyroid, or in patients who have autoimmune thyroiditis. Approximately 20% of patients who have GO are euthyroid.
Pathogenesis
The exact pathogenesis of GO is incompletely understood. GO is an autoimmune disease that macroscopically has evidence of an increase in the volume of extraocular muscles, increased orbital fat volume due to adipogenesis, and inflammation of orbital connective tissue with a varying degree of cicatrisation of the orbital contents. Histopathological changes include an infiltration of T lymphocytes and macrophages in the orbital tissue as well as increased production of hydrophilic glycosaminoglycans. The most likely explanation for these findings in GO is an antigen shared between the thyroid and the orbital tissue. This antigen is most likely the thyrotropin receptor antigen; however, there are several other antigens that may potentially be associated with GO. Regardless of what the antigenic stimuli is, T cells recognize the antigen and initiate an inflammatory response.
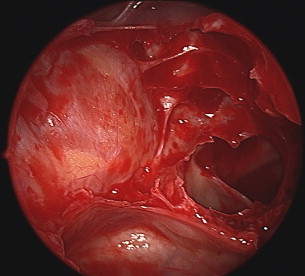
Multiple mechanisms may increase in intraconal volume in GO. The first and most common finding in patients with GO is increased extraocular muscle mass and an increase in orbital fat mass ( Fig. 1 ). The second possible finding is an increase in muscle mass without an increase in the fat mass. The third possibility and rarest finding is of a normal muscle mass and increased fat mass.
The orbit is bounded posteriorly by its bony canal and anteriorly by the tarsoligamentous diaphragm. Therefore, any increase in intraconal volume results in a rise in intraorbital pressure. The rise in pressure at the apex leads to decreased venous drainage resulting in chemosis and periorbital edema, causing further enlargement of the orbital volume.
Epidemiology
Approximately 50% of patients who have Graves disease will develop orbital manifestations. There is a genetic predisposition to the development of GO; family members of patients with GO have a higher chance of manifesting the disease.
Graves disease is more common in females and, therefore, GO is more common in females. However, when GO is present in a male it is usually more severe and progressive than in a female. GO is rare in the pediatric population.
There is a strong relationship between the development of GO and smoking. Smokers develop GO more frequently and the disease is more severe in smokers with the active phase of the disease having a longer time course. Development of GO in smokers is dose dependant. Smokers have a sevenfold increased risk of developing extraocular muscle fibrosis in GO.
Natural history
GO has two distinct phases: active and inactive. Active disease lasts for 6 months to 3 years. During the active phase inflammation, fibrosis and adipogenesis occur resulting in changing signs on physical examination. Inactive disease is defined as the period of the disease where the signs do not progress during a 6 month period. The signs and symptoms of GO can also regress without treatment in up to two-thirds of cases.
In general, medical treatment is offered during the active phase, surgical treatment is offered during the inactive phase.
Clinical features of GO
The most common clinical signs that are apparent are
- •
Eyelid retraction, present in 90% of cases
- •
Proptosis, present in 60% of cases
- •
Extraocular muscle dysfunction, present in 40% of cases.
Other features that commonly occur are
- •
Eyelid and periorbital edema
- •
Conjunctival injection and chemosis
- •
Corneal erosions and superior limbic keratitis.
Optic neuropathy is a less common but very important feature of GO, occurring in 2% to 8% of cases. Optic neuropathy should be suspected when there is decreased best-corrected visual acuity and diagnosed when associated with constricted visual field, red desaturation, and a relative afferent pupillary defect.
The authors consider GO to be severe when vision is at risk. Visual loss in GO occurs in these scenarios:
- 1.
Optic neuropathy. Most commonly secondary to pressure on the nerve due to increased intraorbital volume. It is important to note that fibrosis of the annulus of Zinn and enlargement of the extraocular muscles at the orbital apex can result in optic neuropathy without significant proptosis. More uncommonly, optic neuropathy can be the result of stretch on the optic nerve rather than pressure. On imaging, the posterior sclera is seen to tent at an angle of 90 degrees.
- 2.
Corneal exposure and scarring. Proptosis combined with lid retraction causes poor lid closure or lagophthalmos. This can lead to corneal ulceration, corneal scarring, or perforation of the globe.
Investigations
All patients who are being considered for active surgical intervention should have a CT scan of their paranasal sinuses. Signs that may be apparent on CT scan include excess retroorbital fat, enlargement of the extraocular muscles, and crowding of the orbital apex. As an adjunct to a CT scan, MRI allows for more accurate visualization of the optic nerve and extraocular muscles, as well as potential determination of disease activity. Although imaging is not required in all cases of GO, it should be strongly considered when intervention is being planned.
Treatment
Given the high natural resolution rate of GO and the high degree of cases that remain static, the clinician needs to be mindful that a significant proportion of patients will not require treatment.
Medical treatment
Steroids are a proven treatment for GO and are especially efficacious during the active phase of the disease. Steroids are effective for reducing the extraocular muscle dysfunction and for reducing the optic neuropathy. However, they are not as effective when it comes to reduction in proptosis. Recurrence of the disease both when the steroid is tapered and during steroid therapy is a problem in GO. The major drawback of steroid therapy is that it is often required for several months with associated long-term effects of steroid use.
External beam radiotherapy delivered to the orbital tissue is also a proven treatment modality in patients with active GO. The rationale for the use of radiotherapy in GO is the antiinflammatory effect that it has, as well as the radiosensitivity of the lymphocytes in the orbital tissue. With the exception of extraocular muscle involvement and proptosis, most of the manifestations of GO respond well to radiotherapy. Patients who have severe hypertension or diabetic retinopathy should not be offered radiotherapy due to their risk of developing microvascular abnormalities associated with the treatment.
Multiple immunotherapy drugs, such as tumor necrosis factor inhibitor, are under investigation for their treatment effect in GO. Once their treatment effect has been established, they may become part of the medical treatment for GO.
Surgery
In GO, there is often a mismatch between the volume of the orbit contents and the volume of the bony cavity. This can be addressed surgically by a fat decompression or a bony decompression of one or multiple orbital walls. Bony decompression is applicable across a wider range of GO patients, so orbital fat decompression will not be discussed further.
The indications recommend for bony orbital decompression in GO are
- •
Optic neuropathy
- •
Contraindication to or inability to tolerate medical treatment of optic neuropathy
- •
Clinically severe proptosis that causes exposure keratopathy or is cosmetically unacceptable.
The authors recommend endoscopic medial wall decompression, without exposing the optic nerve in the sphenoid sinus and with teasing out of orbital fat, combined with a balanced decompression of the lateral wall with excision of a portion of the inferolateral fat pad. Once the bone is removed, the periorbita is opened to allow the fat to prolapse.
The most common risk of this operation is diplopia. The diplopia may be transient or require strabismus surgery. According to the literature, the risk of diplopia varies—ranging from 10% to as high as 60%. Multiple techniques have been examined to reduce the postoperative diplopia; however, there is no one technique that has demonstrated consistently superior results. Significant decompression of the orbital floor is associated with the highest rate of postoperative diplopia.
When there is evidence of optic neuropathy, the authors recommend medial wall decompression with exposure of the optic nerve in the sphenoid sinus and without optic nerve sheath fenestration. There is a higher degree of postoperative diplopia in patients who have intervention for optic neuropathy associated with GO than in patients who do not have intervention.
In some cases of GO, there is progression of symptoms after surgery. In these instances, prior surgery is not a contraindication to further decompression and can be associated with an improvement in outcome.
Measures of treatment success
The measurement of proptosis as a marker of success with an exophthalmometer is widely used preoperatively and postoperatively. The degree of reduction that can be obtained via an endoscopic technique alone is 3.5 mm, on average. When external approaches are used or combined with endoscopic approaches, the average reduction in proptosis is 7.4 mm. However, when correlating the degree of proptosis reduction with the visual acuity outcomes or diplopia outcomes, there appears to be little correlation.
After surgical decompression, visual acuity improves. However, given the heterogeneity of the surgical indications, it is difficult to give an accurate number for the expected degree of improvement. In cases of GO-associated optic neuropathy, the improvement that is seen in visual acuity postoperatively is as high as 89%. Analyzing success in patients who have the procedure performed for cosmetic or reconstructive reasons is difficult given the lack of comparability between studies. The authors consider the chance of success in an appropriately selected patient to be very high from a cosmetic or reconstructive point of view.
Idiopathic Orbital Inflammation
Idiopathic orbital inflammation comprises about 10% of orbital lesions. The exact cause of this condition is unknown. It is a diagnosis of exclusion, with lymphoma being the most important differential to exclude.
Idiopathic orbital inflammation is otherwise known as orbital pseudotumor. It is further divided into acute and sclerosing subtypes.
Clinical
Patients present with a variety of symptoms and signs, including:
- •
Proptosis
- •
Diplopia
- •
Pain
- •
Lid swelling
- •
Ptosis
- •
Chemosis.
Investigations
Imaging of the orbit is required in the form of CT scan and/or MRI. The appearance of orbital pseudotumor is a nonspecific orbital mass.
The authors advocate a low threshold to biopsy idiopathic orbital inflammation, especially if there is a doubt as to the diagnosis or the clinical course is not typical for the disease. Twenty-five percent of patients that are appropriately treated with steroids will recur and these patients require biopsy. When there is isolated lacrimal gland involvement, the authors advocate for a low threshold for biopsy to exclude malignancy, which can have a similar presentation in the lacrimal gland.
Treatment
Idiopathic orbital inflammation is a medical condition that is most commonly treated with and is acutely sensitive to oral steroids. Radiotherapy, chemotherapy, or immunosuppression may be appropriate for the treatment of either refractory acute or sclerosing idiopathic orbital inflammation.
This should be done by a multidisciplinary team involving an ophthalmologist and immunologist. Surgery for treatment of idiopathic orbital inflammation should only be considered in the establishment of the diagnosis or when there is an apical mass causing optic neuropathy. In this instance, an apical decompression is used as temporizing measure while awaiting the effect of medical treatment.
Granulomatous
Granulomatous diseases can present in the orbit. These include Wegener granulomatosis, sarcoidosis, and, less commonly, Churg-Strauss disease and xanthogranuloma.
The presentation of granulomatous diseases of the orbit is of a nonspecific orbital inflammation and involvement. The diagnosis is made by a combination of inflammatory markers, imaging, and a biopsy if there is doubt as to the diagnosis.
Once diagnosis for these lesions has been made, it is managed by a multidisciplinary team using immunosuppression. Again, in the scenario of progressive optic neuropathy, an apical decompression is occasionally needed to temporize while awaiting the effect of medical treatment.
Inflammatory diseases of the orbit
GO
GO is the most common extrathyroidal manifestation of Graves disease. Although GO occurs in Graves disease, it may also manifest in patients who have no history of Graves disease, patients who are euthyroid, or in patients who have autoimmune thyroiditis. Approximately 20% of patients who have GO are euthyroid.
Pathogenesis
The exact pathogenesis of GO is incompletely understood. GO is an autoimmune disease that macroscopically has evidence of an increase in the volume of extraocular muscles, increased orbital fat volume due to adipogenesis, and inflammation of orbital connective tissue with a varying degree of cicatrisation of the orbital contents. Histopathological changes include an infiltration of T lymphocytes and macrophages in the orbital tissue as well as increased production of hydrophilic glycosaminoglycans. The most likely explanation for these findings in GO is an antigen shared between the thyroid and the orbital tissue. This antigen is most likely the thyrotropin receptor antigen; however, there are several other antigens that may potentially be associated with GO. Regardless of what the antigenic stimuli is, T cells recognize the antigen and initiate an inflammatory response.
Multiple mechanisms may increase in intraconal volume in GO. The first and most common finding in patients with GO is increased extraocular muscle mass and an increase in orbital fat mass ( Fig. 1 ). The second possible finding is an increase in muscle mass without an increase in the fat mass. The third possibility and rarest finding is of a normal muscle mass and increased fat mass.
The orbit is bounded posteriorly by its bony canal and anteriorly by the tarsoligamentous diaphragm. Therefore, any increase in intraconal volume results in a rise in intraorbital pressure. The rise in pressure at the apex leads to decreased venous drainage resulting in chemosis and periorbital edema, causing further enlargement of the orbital volume.
Epidemiology
Approximately 50% of patients who have Graves disease will develop orbital manifestations. There is a genetic predisposition to the development of GO; family members of patients with GO have a higher chance of manifesting the disease.
Graves disease is more common in females and, therefore, GO is more common in females. However, when GO is present in a male it is usually more severe and progressive than in a female. GO is rare in the pediatric population.
There is a strong relationship between the development of GO and smoking. Smokers develop GO more frequently and the disease is more severe in smokers with the active phase of the disease having a longer time course. Development of GO in smokers is dose dependant. Smokers have a sevenfold increased risk of developing extraocular muscle fibrosis in GO.
Natural history
GO has two distinct phases: active and inactive. Active disease lasts for 6 months to 3 years. During the active phase inflammation, fibrosis and adipogenesis occur resulting in changing signs on physical examination. Inactive disease is defined as the period of the disease where the signs do not progress during a 6 month period. The signs and symptoms of GO can also regress without treatment in up to two-thirds of cases.
In general, medical treatment is offered during the active phase, surgical treatment is offered during the inactive phase.
Clinical features of GO
The most common clinical signs that are apparent are
- •
Eyelid retraction, present in 90% of cases
- •
Proptosis, present in 60% of cases
- •
Extraocular muscle dysfunction, present in 40% of cases.
Other features that commonly occur are
- •
Eyelid and periorbital edema
- •
Conjunctival injection and chemosis
- •
Corneal erosions and superior limbic keratitis.
Optic neuropathy is a less common but very important feature of GO, occurring in 2% to 8% of cases. Optic neuropathy should be suspected when there is decreased best-corrected visual acuity and diagnosed when associated with constricted visual field, red desaturation, and a relative afferent pupillary defect.
The authors consider GO to be severe when vision is at risk. Visual loss in GO occurs in these scenarios:
- 1.
Optic neuropathy. Most commonly secondary to pressure on the nerve due to increased intraorbital volume. It is important to note that fibrosis of the annulus of Zinn and enlargement of the extraocular muscles at the orbital apex can result in optic neuropathy without significant proptosis. More uncommonly, optic neuropathy can be the result of stretch on the optic nerve rather than pressure. On imaging, the posterior sclera is seen to tent at an angle of 90 degrees.
- 2.
Corneal exposure and scarring. Proptosis combined with lid retraction causes poor lid closure or lagophthalmos. This can lead to corneal ulceration, corneal scarring, or perforation of the globe.
Investigations
All patients who are being considered for active surgical intervention should have a CT scan of their paranasal sinuses. Signs that may be apparent on CT scan include excess retroorbital fat, enlargement of the extraocular muscles, and crowding of the orbital apex. As an adjunct to a CT scan, MRI allows for more accurate visualization of the optic nerve and extraocular muscles, as well as potential determination of disease activity. Although imaging is not required in all cases of GO, it should be strongly considered when intervention is being planned.
Treatment
Given the high natural resolution rate of GO and the high degree of cases that remain static, the clinician needs to be mindful that a significant proportion of patients will not require treatment.
Medical treatment
Steroids are a proven treatment for GO and are especially efficacious during the active phase of the disease. Steroids are effective for reducing the extraocular muscle dysfunction and for reducing the optic neuropathy. However, they are not as effective when it comes to reduction in proptosis. Recurrence of the disease both when the steroid is tapered and during steroid therapy is a problem in GO. The major drawback of steroid therapy is that it is often required for several months with associated long-term effects of steroid use.
External beam radiotherapy delivered to the orbital tissue is also a proven treatment modality in patients with active GO. The rationale for the use of radiotherapy in GO is the antiinflammatory effect that it has, as well as the radiosensitivity of the lymphocytes in the orbital tissue. With the exception of extraocular muscle involvement and proptosis, most of the manifestations of GO respond well to radiotherapy. Patients who have severe hypertension or diabetic retinopathy should not be offered radiotherapy due to their risk of developing microvascular abnormalities associated with the treatment.
Multiple immunotherapy drugs, such as tumor necrosis factor inhibitor, are under investigation for their treatment effect in GO. Once their treatment effect has been established, they may become part of the medical treatment for GO.
Surgery
In GO, there is often a mismatch between the volume of the orbit contents and the volume of the bony cavity. This can be addressed surgically by a fat decompression or a bony decompression of one or multiple orbital walls. Bony decompression is applicable across a wider range of GO patients, so orbital fat decompression will not be discussed further.
The indications recommend for bony orbital decompression in GO are
- •
Optic neuropathy
- •
Contraindication to or inability to tolerate medical treatment of optic neuropathy
- •
Clinically severe proptosis that causes exposure keratopathy or is cosmetically unacceptable.
The authors recommend endoscopic medial wall decompression, without exposing the optic nerve in the sphenoid sinus and with teasing out of orbital fat, combined with a balanced decompression of the lateral wall with excision of a portion of the inferolateral fat pad. Once the bone is removed, the periorbita is opened to allow the fat to prolapse.
The most common risk of this operation is diplopia. The diplopia may be transient or require strabismus surgery. According to the literature, the risk of diplopia varies—ranging from 10% to as high as 60%. Multiple techniques have been examined to reduce the postoperative diplopia; however, there is no one technique that has demonstrated consistently superior results. Significant decompression of the orbital floor is associated with the highest rate of postoperative diplopia.
When there is evidence of optic neuropathy, the authors recommend medial wall decompression with exposure of the optic nerve in the sphenoid sinus and without optic nerve sheath fenestration. There is a higher degree of postoperative diplopia in patients who have intervention for optic neuropathy associated with GO than in patients who do not have intervention.
In some cases of GO, there is progression of symptoms after surgery. In these instances, prior surgery is not a contraindication to further decompression and can be associated with an improvement in outcome.
Measures of treatment success
The measurement of proptosis as a marker of success with an exophthalmometer is widely used preoperatively and postoperatively. The degree of reduction that can be obtained via an endoscopic technique alone is 3.5 mm, on average. When external approaches are used or combined with endoscopic approaches, the average reduction in proptosis is 7.4 mm. However, when correlating the degree of proptosis reduction with the visual acuity outcomes or diplopia outcomes, there appears to be little correlation.
After surgical decompression, visual acuity improves. However, given the heterogeneity of the surgical indications, it is difficult to give an accurate number for the expected degree of improvement. In cases of GO-associated optic neuropathy, the improvement that is seen in visual acuity postoperatively is as high as 89%. Analyzing success in patients who have the procedure performed for cosmetic or reconstructive reasons is difficult given the lack of comparability between studies. The authors consider the chance of success in an appropriately selected patient to be very high from a cosmetic or reconstructive point of view.
Idiopathic Orbital Inflammation
Idiopathic orbital inflammation comprises about 10% of orbital lesions. The exact cause of this condition is unknown. It is a diagnosis of exclusion, with lymphoma being the most important differential to exclude.
Idiopathic orbital inflammation is otherwise known as orbital pseudotumor. It is further divided into acute and sclerosing subtypes.
Clinical
Patients present with a variety of symptoms and signs, including:
- •
Proptosis
- •
Diplopia
- •
Pain
- •
Lid swelling
- •
Ptosis
- •
Chemosis.
Investigations
Imaging of the orbit is required in the form of CT scan and/or MRI. The appearance of orbital pseudotumor is a nonspecific orbital mass.
The authors advocate a low threshold to biopsy idiopathic orbital inflammation, especially if there is a doubt as to the diagnosis or the clinical course is not typical for the disease. Twenty-five percent of patients that are appropriately treated with steroids will recur and these patients require biopsy. When there is isolated lacrimal gland involvement, the authors advocate for a low threshold for biopsy to exclude malignancy, which can have a similar presentation in the lacrimal gland.
Treatment
Idiopathic orbital inflammation is a medical condition that is most commonly treated with and is acutely sensitive to oral steroids. Radiotherapy, chemotherapy, or immunosuppression may be appropriate for the treatment of either refractory acute or sclerosing idiopathic orbital inflammation.
This should be done by a multidisciplinary team involving an ophthalmologist and immunologist. Surgery for treatment of idiopathic orbital inflammation should only be considered in the establishment of the diagnosis or when there is an apical mass causing optic neuropathy. In this instance, an apical decompression is used as temporizing measure while awaiting the effect of medical treatment.
Granulomatous
Granulomatous diseases can present in the orbit. These include Wegener granulomatosis, sarcoidosis, and, less commonly, Churg-Strauss disease and xanthogranuloma.
The presentation of granulomatous diseases of the orbit is of a nonspecific orbital inflammation and involvement. The diagnosis is made by a combination of inflammatory markers, imaging, and a biopsy if there is doubt as to the diagnosis.
Once diagnosis for these lesions has been made, it is managed by a multidisciplinary team using immunosuppression. Again, in the scenario of progressive optic neuropathy, an apical decompression is occasionally needed to temporize while awaiting the effect of medical treatment.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


