Osteomata of the frontal and ethmoid sinuses have traditionally been surgically removed via external approaches. However, endoscopic techniques have increasingly been used for the surgical management of selected cases. Advances in visualization and instrumentation, as well as the excellent access provided by the Draf type 3 procedure, expanded the reach of endoscopes. We describe current limits of endoscopic approaches in the removal of osteomata from the frontal sinus and our algorithms for their management. We believe that the vast majority of frontal sinus osteomata can be managed endoscopically, änd that only significant anterior or extreme infero-lateral extension constitute major limiting factors.
| EBM Question | Level of Evidence | Grade of Recommendation |
|---|---|---|
| What are the limits of the endoscopic approach? | 4 | C |
Osteoma is a benign, slow-growing bone tumor consisting primarily of well-differentiated mature, compact, or cancellous bone. Osteoma is the most common benign tumor of the paranasal sinuses with a point prevalence of 3%, as demonstrated in 2 computed tomography (CT) radiological studies of 1500 and 1889 patients respectively.
Age and sex
Osteomas occur more often in men, with a variable male-to-female ratio of 1.3:1.0 to 1.5:1.0. Their peak incidence is between the fourth and sixth decades, with an average age at presentation of 50 years.
Location
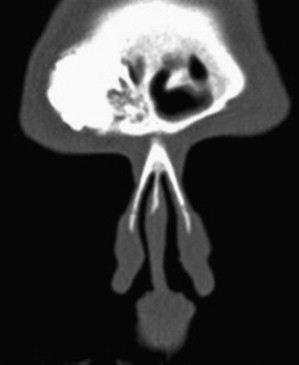
Most osteomas (58% to 68% ) involve the frontal sinus (37% arise in the immediate vicinity of the nasofrontal duct and 21% above and lateral to the frontal ostium). The ethmoid sinus is the second most common area to be involved, whereas maxillary sinuses are affected in about 20% of cases, and sphenoid sinuses are rarely involved. Osteomas can occur in conjunction with Gardner syndrome (familial adenomatous polyposis) ( Fig. 1 ), an autosomal dominant condition consisting of multiple osteomas, soft tissue tumors (including skin cysts and desmoid tumors), and colon polyps with a high propensity toward malignant transformation. As osteomas tend to appear an average of 17 years before the colon polyps, early gastroenterology referral is strongly advised.

Location
Most osteomas (58% to 68% ) involve the frontal sinus (37% arise in the immediate vicinity of the nasofrontal duct and 21% above and lateral to the frontal ostium). The ethmoid sinus is the second most common area to be involved, whereas maxillary sinuses are affected in about 20% of cases, and sphenoid sinuses are rarely involved. Osteomas can occur in conjunction with Gardner syndrome (familial adenomatous polyposis) ( Fig. 1 ), an autosomal dominant condition consisting of multiple osteomas, soft tissue tumors (including skin cysts and desmoid tumors), and colon polyps with a high propensity toward malignant transformation. As osteomas tend to appear an average of 17 years before the colon polyps, early gastroenterology referral is strongly advised.

Etiology of osteoma
There are 3 main pathogenetic theories regarding the etiology of osteomas: developmental, traumatic, and infective. According to the developmental theory, as proposed by Cohnheim, osteomas arise from stem cells of the junctional area between the frontal and ethmoid bone. This is supported by the fact that osteomas frequently occur at the fontoethmoid suture line where the frontal sinus (membranous bone) borders the ethmoid labyrinth (endochondral ossification). However, this theory does not explain osteomas found in other locations. The traumatic theory, as proposed by Gerber, suggests that osteomas arise as an abnormal proliferative response to trauma and is supported by both the higher incidence of osteomas in men and the development of osteomas during puberty, when the rate of skeletal development is at its peak. However, most osteomas are detected later in life and the great majority of patients do not report any history of trauma, whereas an increased incidence of osteomata in patients undergoing multiple endoscopic sinus surgery procedures has never been documented. Alternatively, it has been suggested that osteomas may arise as a result of infection stimulating osteoblasts within the mucoperiosteal lining of the sinus, which in turn may become secondarily calcified. Although there is an association between osteoma and sinusitis, the cause-and-effect relationship is not clear, and in up to 63% of cases, osteomas arise in healthy sinuses. Other less substantiated theories suggest that osteomas may be osteodysplastic lesions, osteogenic hamartomas, embryonic bone rests, or the result of ossification of sinus polyps. However, none of these hypotheses have been proven.
Histology of osteoma
Macroscopically, osteomas are round or oval, hard, ivory-white, bosselated, well-circumscribed lesions attached to the underlying bone by a broad base or occasionally by a small stalk and covered by a thin layer of fibrous periosteum. Histologically, osteomas can be classified into 3 types: ivory or compact, mature or cancellous, or spongiotic and mixed. Ivory osteomas usually have a sessile base and are characterized by hard bone with a thick matrix containing only a small amount of fibrous tissue and minimal marrow. Cancellous osteomas often have a pedunculated base and are composed of cancellous bone with intertrabecular hematopoietic bone marrow or fat, whereas mixed osteomas share characteristics from both types ( Fig. 2 ).

Growth
In a study of 13 osteomas with serial radiographs, the average growth rate was 1.61 mm per year, ranging from 0.44 to 6.00 mm per year. It has been shown that most osteomas recur infrequently even after incomplete removal. However, given enough time, osteomas can recur, and indeed accelerated regrowth following incomplete removal has been documented. Malignant transformation of an osteoma has never been described, and osteomas should not be considered neoplastic lesions.
Clinical characteristics of osteoma
Most osteomata are asymptomatic, slow-growing lesions diagnosed incidentally in imaging studies. Only 4% to 10% of all osteomas produce clinical symptoms, with osteomas of the frontoethmoidal region tending to be associated with earlier symptoms. Such symptoms are most commonly frontal pressure or headache, either directly resulting from the lesion or indirectly from impaired drainage of the frontal sinus with or without concomitant chronic rhinosinusitis. The incidence of headache in various osteoma series varies between 52% and 100% ( Table 1 ).
| Study, Year, Journal | Cases | Presenting Symptoms | Location | Tumor Grade | Procedure | Outcome | Complications | Follow-Up (Months) |
|---|---|---|---|---|---|---|---|---|
| Brodish et al | 9 | Headache | 9 frontoethmoidal | nr | 9 end | 0 | 2 CSF leaks | 40 |
| Schick et al | 34 | Headache | 23 frontal sinus 11 ethmoid | nr | 23 end 11 open | 3 residuals (end) | 0 | 1–32 |
| Chiu et al | 9 | Headache 88% Sinusitis 66% | 9 frontal sinus | I: 1 II: 2 III: 4 IV: 2 | 3 end 5 combined 1 open | nr | 0 | 7.4 |
| Dubin and Kuhn | 12 | Headache 100% | 12 frontal sinus | I: 3 III: 8 IV: 1 | 8 end 4 combined | 2 residuals (open) 1 residuals (end) | 1 frontal stenosis (open) | 19.2 |
| Bignami et al | 26 | Headache 63% Nasal obstr 38% | 26 frontal sinus | nr | 11 end 13 combined 2 open | 0 recurrences | 0 | 40 |
| Castelnuovo et al | 48 | Headache 52% | 18 frontal sinus 13 frontoethmoid 9 ethmoid 8 other | nr | 22 end 26 open | nr | 0 | 53 (end) 35 (open) |
| Seiberling et al | 23 | Headache 62.5% Sinusitis 56.5% | 18 frontal sinus 5 frontal recess | I: 5 II: 4 III: 6 IV: 8 | 2 combined 21 end | 4 residuals | 1 frontal stenosis (end) | 33 |
| Ledderose et al | 24 | Headache 83% Sinusitis 87% | 7 frontal sinus 7 frontal recess | I: 3 II: 5 III: 10 IV: 6 | 12 combined 8 end 4 open | 95% satisfied a 1 pain increase | 1 bleeding (combined) 1 bleeding (open) | nr |
Complete obstruction of a sinus ostium by an osteoma may lead to secondary formation of mucocele. When an osteoma extends beyond the confines of the sinuses, it may produce an external deformity ( Fig. 3 ). Orbital extension may lead to proptosis and periorbital pain, as well as chemosis and diplopia if the oculomotor muscles are affected or epiphora if the nasolacrimal duct is compressed ( Fig. 4 ) and rarely decreased visual acuity in cases of optic nerve compression. Intracranial extension of the lesion can lead to intracranial mucocele with meningitis, cerebral abscess, or even tension pneumocephalus ( Fig. 5 ). In our experience, headache is the sole presenting symptom of osteomas in the vast majority of cases, whereas the slow growth of an osteoma usually precludes eye symptoms, even in cases of significant orbital extension, unless a concomitant mucocele is present.

Imaging
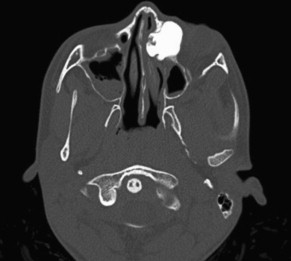
Although osteomata can be seen in simple sinus radiographs, the imaging modality of choice is thin-slice CT. This allows the precise estimation of the size and the location of the osteoma, as well as concurrent sinus pathology. Osteomata appear as well-circumscribed masses of heterogeneous consistency on CT, with hyperostotic (high signal) and spongiotic (lower signal) components ( Fig. 6 ). The lower signal components may be confused with associated mucoceles. In such patients, magnetic resonance imaging is useful to assess the extent of the tumor as well as the presence of complications (mucoceles, orbital or intracranial extension).

Indications
Although it is generally agreed that symptomatic osteomas (unless there are serious contraindications) should be surgically excised, management of asymptomatic osteomata is controversial. In the case of small, uncomplicated osteomata, watchful waiting with interval radiologic imaging is usually advised. Savić and Djerić recommend surgical removal of enlarging frontal sinus osteomas, those extending beyond the boundaries of the sinus, localized adjacent to the nasofrontal duct, associated with chronic sinusitis, or in patients complaining of headaches when all other causes have been excluded, as well as osteomas in the ethmoid sinuses, irrespective of their size. Smith and Calcaterra recommend surgery if the osteoma occupies more than 50% of the frontal sinus. Our policy is to treat the following:
- •
Osteomas associated with symptoms (usually headache) after all other explanations for the symptoms have been excluded
- •
Large (extending to more than 50% of the frontal sinus) or growing osteomas, as seen on serial CTs
- •
Osteomas associated with current (mucocele, orbital symptoms, neurologic symptoms, external deformity), imminent (complete obstruction of the frontal recess, intraorbital or intracranial extension) complications.
We do not operate small ethmoid osteomas, which, more often than not, are incidental CT findings with no clinical significance.
Lynch Procedure
One of the first methods used to treat symptomatic frontal or frontoethmoid osteomas was the external frontoethmoidectomy approach (Lynch procedure). This has been used for small, medially or inferiorly situated tumors. However, it can lead to an unsightly scar, does not provide adequate access laterally, and has a high rate of frontal recess stenosis.
Osteoplastic Flap Procedures
The osteoplastic approach, as popularized by Goodale and Montgomery, has been the most widely used technique for frontal sinus osteomas. It provides excellent visualization and wide access to the frontal sinus, including its superior, posterior, and lateral aspects, although the nasofrontal duct and ethmoids may not always be adequately visualized. The osteoplastic flap procedure is well established, being in use for more than 40 years, and is technically accessible to most otolaryngologists. Nevertheless, it is an invasive procedure, with significant morbidity, including blood loss, impaired cosmesis, postoperative frontal pain, paresthesia, or anesthesia from supraorbital nerve damage and (rarely) in the case of intracranial entry, potentially devastating complications including cerebrospinal fluid (CSF) leak and meningitis. If the frontal sinus is obliterated, then the added morbidity of an abdominal incision for fat harvesting is introduced, as well as the risk of late mucocele formation, which can be as high as 9% after 2 years.
Endoscopic Procedures
Endoscopic approaches to the nose and paranasal sinuses were introduced in the 1980s, and by the early 1990s the first cases of endoscopic management of ethmoid osteoma were published. The accumulation of experience with endoscopic sinus surgery, technological advances, including the development of dedicated instruments (malleable forceps; 40-degree, 55-degree, and 70-degree curved diamond and cutting drills; straight high-speed neurosurgical drill; and dedicated bipolar intranasal diathermy forceps), improved endoscopes, and the introduction of CT navigation, expanded the limits of endoscopic approaches. On the other hand, the work of Draf, in systematizing the approaches to the frontal sinus, laid the foundations of modern endoscopic frontal sinus surgery. Importantly, he described the type 3 (“Draf 3”) procedure (endoscopic modified lothrop, bilateral frontal sinus drillout, median drainage procedure ) as a way to establish the widest possible transnasal access to the frontal sinus.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


