(1)
Department of Pathology, Duke University Medical Center, Durham, NC, USA
Abstract
The orbit is home to a diverse spectrum of general and subspecialized surgical pathology. A wide variety of benign and malignant neoplasms, inflammatory, and nonneoplastic conditions occur within the orbit.
The orbit helps protect the eye, and in an adult human measures approximately 40 mm in height, 45 mm in depth, and has a volume of 30 ml. A model showing the optic foramen and superior orbital fissure (Fig. 7.1) and globe (Fig. 7.2) is shown.
The orbital components include the lacrimal gland; the smooth muscle; the blood vessels; the fibroadipose tissue; the peripheral nerves; the ciliary ganglion of the oculomotor nerve (Fig. 7.3); the seven bones of the skull, face, and nose; the extraocular muscles, the optic nerve and its meninges, the globe; and the cartilaginous trochlea. The trochlea functions as a “sling” for the superior oblique muscle (Figs. 7.4, 7.5).
It is important to know the normal histology and components of the orbit. For example, knowing that the ciliary ganglion resides within the orbit explains the finding of the rare primary orbital paraganglioma. You do not necessarily need any special eye pathology training to recognize this, since orbital paragangliomas resemble nonorbital paragangliomas. You just need to be aware that paragangliomas can occur in the orbit.
The extraocular muscles are skeletal muscles, and their involvement in mitochondrial disorders and inflammatory lesions will be discussed here. The optic nerve and meninges are discussed in Chap. 8.
Overview of Orbital Pathology
The orbit is home to a diverse spectrum of general and subspecialized surgical pathology. A wide variety of benign and malignant neoplasms, inflammatory, and nonneoplastic conditions occur within the orbit.
The orbit helps protect the eye, and in an adult human measures approximately 40 mm in height, 45 mm in depth, and has a volume of 30 ml. A model of the skull/orbit shows the optic foramen and superior orbital fissure (Fig.7.1) and globe (Fig. 7.2).
The orbital components include the lacrimal gland; smooth muscle; blood vessels; fibroadipose tissue; peripheral nerves; the ciliary ganglion of the oculomotor nerve (Fig. 7.3 ); seven bones of the skull, face, and nose; the extraocular muscles, the optic nerve and its meninges, the globe; and the cartilaginous trochlea. The trochlea functions as a “sling” for the superior oblique muscle (Figs. 7.4,7.5).
It is important to know the normal histology and components of the orbit. For example, knowing that the ciliary ganglion resides within the orbit explains the finding of the rare primary orbital paraganglioma. You do not necessarily need any special eye pathology training to recognize this, since orbital paragangliomas resemble nonorbital paraganglioma. You just need to be aware that paragangliomas, albeit rarely, can occur in the orbit.
The Wills Eye Hospital Oncology Service in Philadelphia reviewed 1,264 consecutive patients with a space-occupying orbital lesion over a 30-year period and reported the following findings:


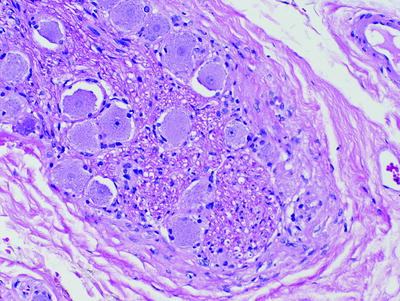
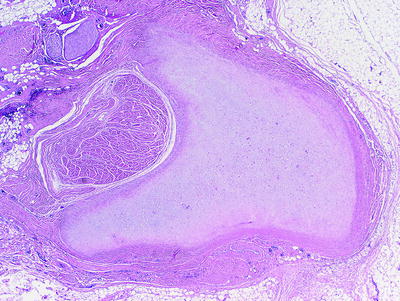
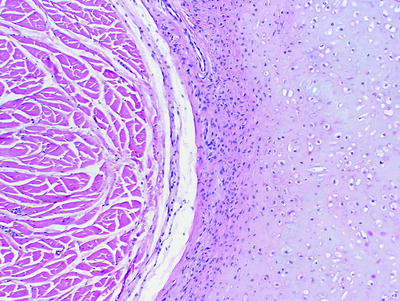
Fig. 7.1
Model of the human skull showing the orbit with the superior orbital fissure and the optic nerve foramen medial to it
Fig. 7.2
Model of the human skull showing the orbit with the globe
Fig. 7.3
Ciliary ganglion within the orbit showing ganglion cells with Nissl substance and visible nucleoli
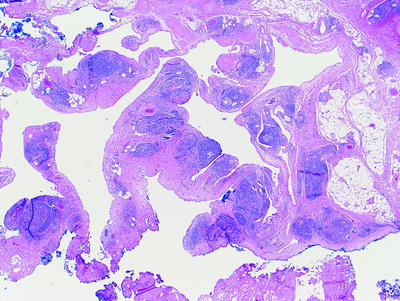
Fig. 7.4
Fortuitous section from an orbital exenteration specimen showing the trochlea, the only cartilaginous tissue within the eye
Fig. 7.5
Higher magnification of Fig. 7.4 showing the cartilaginous trochlea on the right and the superior oblique muscle on the left
810 (64%) of the lesions were benign.
454 (36%) of the lesions were malignant.
Regarding primary orbital tumors:
Rhabdomyosarcoma is the most common orbital malignancy in children (median age 7 years).
Lymphoma is the most common orbital malignancy in older adults (median age 71 years).
Epithelial tumors of the lacrimal gland are more common in middle-aged patients (median age 40 years).
The general categories of orbital tumors are listed here. The top four will be expanded below, and some diagnoses for the other categories are mentioned:




Lacrimal gland tumors
Secondary tumors
Inflammatory lesions
Lymphoid tumors and leukemias
Cartilaginous and osseous tumors:
Chondroma (association with the cartilaginous trochlea)
Giant cell tumor of bone
Mesenchymal chondrosarcoma
Vascular tumors:
Perivascular tumors:
Hemangiopericytoma/solitary fibrous tumor
Primary melanocytic tumors:
Malignant melanoma (arise from nevus of Ota/melanosis oculi)
Peripheral nerve tumors:
Neurofibroma
Schwannoma
Malignant peripheral nerve sheath tumor
Myogenic tumors:
Rhabdomyosarcoma
Fibrous tumors:
Fibrous histiocytoma
Giant cell angiofibroma
Lipomatous and myxomatous tumors:
Lipoma. Pitfall: Do not misdiagnose prolapsed orbital fat – which can resemble pleomorphic lipoma – as a lipomatous tumor. Again, knowing the clinical situation is very important.
Liposarcoma.
Myxoma.
Histiocytic tumors:
Langerhans cell histiocytosis (eosinophilic granuloma)
Non-Langerhans cell histiocytosis (Rosai-Dorfman disease)
Germ cell tumors:
Seminomatous and nonseminomatous tumors
Teratomas
Optic nerve, meningeal, and other neural tumors (see Chap. 8 “Optic Nerve”):
Ectopic brain tissue may rarely be the etiology of an orbital mass lesion (Figs. 7.8, 7.9, 7.10).
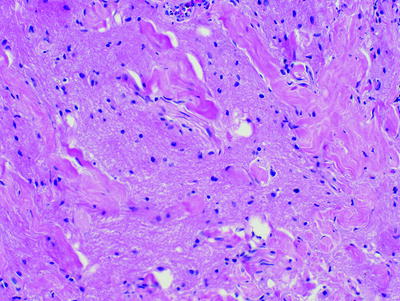
Fig. 7.8
Ectopic brain tissue in the orbit. This is rarely the etiology of an orbital mass lesion
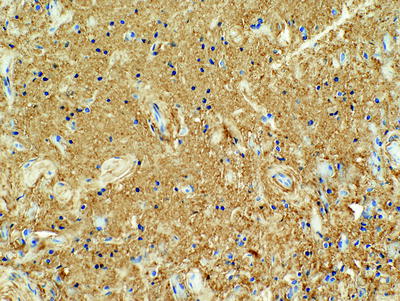
Fig. 7.9
Ectopic brain tissue in the orbit showing immunoreactivity for glial fibrillary acidic protein (GFAP)
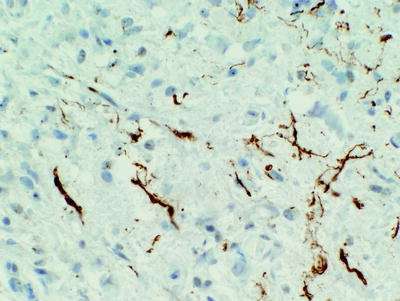
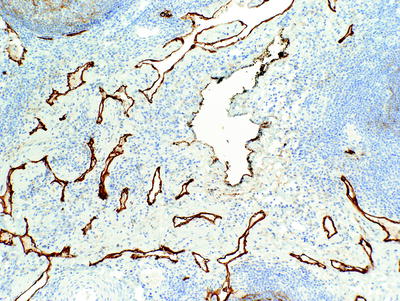
Fig. 7.10
Ectopic brain tissue in the orbit. A neurofilament protein immunohistochemical stain highlights axons
Tumors of uncertain histogenesis such as alveolar soft parts sarcoma have been reported in the orbit; in summary, almost anything is possible in the orbit.< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
