Purpose
To evaluate the efficacy of oral mucosal graft to correct not only lid margin keratinization and trichiasis or distichiasis, but also incomplete closure in severe cicatricial ocular surface diseases.
Design
Retrospective, noncomparative, interventional case series.
Methods
Twenty-two eyes (39 eyelids) of 19 patients received an oral mucosal graft during lid margin reconstruction from September 2007 through February 2010. Relief of symptoms, conjunctival inflammation, corneal epithelial abnormalities, and visual acuity were compared before and after surgeries as outcome measures.
Results
Among 22 eyes, 10 eyes (45.5%) had lid margin keratinization, trichiasis or distichiasis, or both, resulting in blink-related microtrauma. The oral mucosal graft resulted in successful correction in 6 eyes; in the remaining eyes, trichiasis in 3 eyes and distichiasis in 1 eye were away from the corneal surface. Incomplete closure present in 12 (54.5%) eyes was completely corrected in 9 eyes and was much improved in the remaining 3 eyes. During a mean follow-up of 16.2 months, reports of foreign body sensation, photophobia, pain, burning, tearing, and discharge were relieved significantly in 17 (77.3%) of 22 eyes. The visual acuity was improved in 13 eyes (59.1%) and was maintained in 8 eyes. Conjunctival inflammation was reduced markedly in 19 eyes (86.4%). Corneal epithelial defect and superficial punctate keratopathy were healed rapidly or improved in 14 eyes, and regression of superficial vascularization was noted in 1 eye.
Conclusions
Oral mucosal graft can reduce not only blink-related microtrauma caused by lid margin keratinization and trichiasis or distichiasis, but also exposure caused by cicatricially induced incomplete closure, thus preventing further deterioration of the ocular surface.
Cicatricial ocular surface diseases such as Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis, ocular cicatricial pemphigoid, and chemical burns encompass a myriad of ocular complications leading to significant visual morbidity. Scarring in the lid margin, the tarsus, and the fornix may lead to keratinization, trichiasis, distichiasis, and entropion. These lid margin and lash abnormalities invariably cause chronic blink-related microtrauma to the ocular surface, and recently have been shown to be significantly correlated with persistent ocular surface inflammation and subsequent corneal blindness. In contrast, these cicatricial complications also can cause incomplete blinking or closure and interfere with the Bell phenomenon, resulting in unwanted exposure of the ocular surface. Such an exposure problem may occur not only during the day when the eye is open, but also during sleep, resulting in lagophthalmos. Cumulative insults from both blink-related microtrauma and chronic exposure further deteriorate the ocular surface and contribute to higher failure rates when ocular surface reconstructive procedures are contemplated.
For these 2 pathogenic elements, that is, blink-related microtrauma and incomplete closure, large-diameter contact lenses and specialty scleral lens do protect the cornea to a certain extent. However, lens fitting can be a problem in eyes with significant symblepharon, and compliance is particularly poor in these cicatricial diseases. The long-term use of bandage contact lenses and scleral lenses is not without complications, especially in eyes with sicca. So, the definitive solution often is surgical reconstruction.
Oral mucosal graft is commonly used during oculoplastic surgeries to replace the ocular (corneal and conjunctival) surface as well as for reconstruction of the eyelid, the fornix, and the socket. For reconstruction of the lid margin, oral mucosal graft can correct trichiasis and entropion. Recently, Iyer and associates used mucous membrane grafting for correcting lid margin keratinization in SJS to reduce ocular surface inflammation and to improve patient comfort and visual acuity. However, their study excluded severe cases with extensive symblepharon, entropion, ocular surface cicatrization, and severe dry eye. Herein, we demonstrate that oral mucosal graft can be used not only for correcting distichiasis causing blink-related microtrauma, but also for incomplete closures that frequently are found in severe cicatricial ocular surface diseases.
Methods
Patients
The medical records were reviewed retrospectively of 19 consecutive patients (22 eyes, 39 eyelids) who underwent lid margin reconstruction with oral mucosal graft by 1 surgeon (S.C.G.T.) at the Ocular Surface Center, Miami, Florida, from September 2007 through February 2010. The inflammatory activity of all 4 patients with ocular cicatricial pemphigoid had been controlled before surgery, and no systemic immunosuppression was needed before or after enrollment in this study. For patients with either chemical burns or SJS/toxic epidermal necrolysis, their insults were remote and there was no active inflammation, either. As a routine practice at the Ocular Surface Center, all patients underwent photographic documentation at all preoperative and postoperative visits and digital recordings of their surgical procedures. For this study, all eligible patients should have completed at least 6 months of follow-up after surgery. The clinical data concerning demographic information, preoperative diagnosis, previous managements, surgical procedures, visual acuity, outcome of surgery, and complications were retrieved ( Table ).
| Patient No. | Sex/Age (y) | Eye | Causes | Previous Management and Surgeries | Lids Operated | Intraoperative and Postoperative Management | Follow-up (mos) | Outcome | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Symptoms (Preoperative/Postoperative) | VA (Preoperative; Postoperative) | Lid Margin and Lash Abnormalities (Preoperative/Postoperative) | Conjunctival Inflammation (Preoperative/Postoperative) | Corneal Epithelial Abnormalities (Preoperative/Postoperative) | ||||||||
| 1 | F/38 | Right | SJS | SL, BCL | U | FR | 6 | FB/− | 20/400 | K/− | ++/+ | – |
| 2 | M/77 | Right | OCP | BCL | L | 7 | FB/− | 20/20 | Tri/− | ++/− | – | |
| 3 | F/47 | Right | SJS | SL, BCL | U, L | BCL | 16 | FB, P, Ph/− | 20/200; 20/40 | K, Dis/− | +++/+ | PED/− |
| Left | SJS | SL, BCL | U a , L | BCL | 15 | FB, P, Ph/FB | 20/25; 20/20 | K, Dis/Dis | ++/++ | SPK/SPK | ||
| 4 | M/77 | Right | OCP | BCL | U a , L | 11 | FB, Ph/FB | 20/60; 20/40 | K, Tri/Tri | ++/+ | SPK/− | |
| Left | OCP | BCL | U, L | 11 | FB, Ph/− | 20/100; 20/50 | K, Tri/− | +++/+ | PED/− | |||
| 5 | F/11 | Right | SJS | SL | U, L | FR | 21 | B/B | HM; CF | K, Tri, Dis/Tri | +++/+ | – |
| 6 | F/29 | Right | SJS | BCL, FR | U | BCL | 8 | FB/− | HM; 20/400 | K, Tri, Dis/− | ++/− | – |
| 7 | F/49 | Left | SJS | LR, FR | U, L | 26 | Ph, D/− | 20/400; 20/100 | K, Dis/− | ++/++ | PED/− | |
| 8 | M/16 | Left | SJS | BCL | U, L | BCL | 15 | FB/− | 20/40 | K, Tri/Tri | ++/− | – |
| 9 | M/72 | Left | PS | BCL, LR, FR | L | 29 | Ph, D/− | 20/200; 20/70 | I/− | +++/+ | PED/SPK | |
| 10 | M/75 | Right | PS | BCL, TA | U, L | TA | 24 | FB/− | NLP | I/− | +++/+ | SPK/− |
| 11 | F/80 | Right | PS | BCL, PKP, FR, TA | U, L | TA | 28 | P/− | HM | I/I | +++/+ | PED/− |
| 12 | M/24 | Right | CB | BCL, PKP, FR, TA | U, L | FR | 13 | B/− | LP; HM | I/I | +++/+ | PED/− |
| 13 | F/70 | Left | OCP | BCL, PKP, FR | L | PKP | 13 | B,T/− | CF; 20/200 | K, I/− | +++/++ | PED/− |
| 14 | M/6 | Right | TEN | FR | U, L | TA | 13 | FB/− | HM; CF | K, I/I | +++/+ | PED/− |
| 15 | M/46 | Right | CB | BCL, KLAL, PKP, TA, LR | U, L | BCL | 26 | FB/− | 20/100; 20/70 | Tri, I/− | +/− | PED/− |
| 16 | M/57 | Right | CB | FR | U, L | TA | 9 | FB, Ph/B,D | LP | Tri, I/Tri | +++/++ | PED/− |
| 17 | F/10 | Right | SJS | BCL,LR | U, L | 23 | Ph, D/− | 20/200 | K, Tri, I/− | +/− | Vascularization/− | |
| 18 | F/70 | Right | SJS | BCL, FR | U a , L a | BCL | 15 | FB, B, Ph/FB | CF; HM | K, Dis, I/− | +++/++ | SPK/− |
| Left | SJS | BCL | U, L | BCL | 15 | FB, B, Ph/Ph | CF | K, Dis, I/Dis | +++/+++ | – | ||
| 19 | M/15 | Left | SJS | U a , L | 12 | Ph, D/− | CF; 20/400 | K, Tri, I/− | +++/+ | – | ||
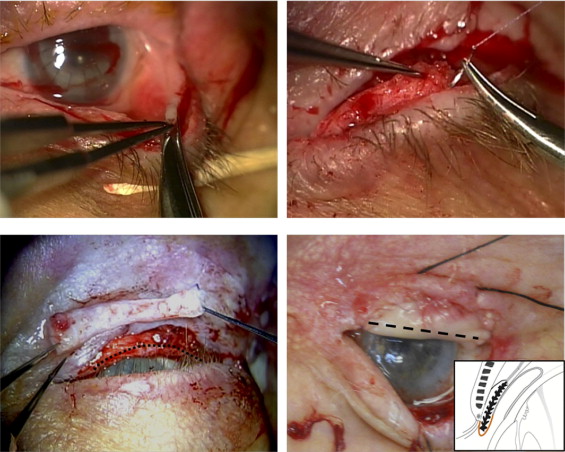
Surgical Techniques
The surgery was carried out under general anesthesia with the endotracheal tube secured to one side of the mouth so as to allow adequate exposure of the oral mucosa on the other side (usually corresponding to the same side of the eye to be operated on) and using a surgical microscope so that the detailed excision described below could be executed precisely. The lids were opened with a 4-0 black silk suture placed at the upper and lower lid margin to evert the lid so as to reveal the lid margin and the tarsus. If symblepharon was noted, its conjunctival edge was lifted up and recessed to an area where the cicatricial tension was released. The denuded surface was covered by a sheet of cryopreserved amniotic membrane (Bio-Tissue, Inc, Miami, Florida, USA) using fibrin glue (Tisseel; Baxter, Irvine, California, USA). Then, the anterior lamella was split from the grey line, and the lid margin keratinization and tarsal scar were dissected and excised ( Figure 1 , Top left). The skin–muscle flap along with the marginal lashes were recessed and fixated 3 to 4 mm posterior to the tarsal margin onto the anterior tarsal surface using 3 or 4 8-0 Vicryl (Ethicon; Johnson & Johnson, Somerville, New Jersey, USA) mattress sutures ( Figure 1 , Top right). The distichiasis coming from the meibomian gland orifice was removed selectively by scissor excision only to amputate the lash root without damaging the remaining tarsal plate. The defect was measured using a caliber. Then, the attention was directed to the inferior labial surface of the mouth, where submucosal injection of 2% lidocaine with 1:1000 epinephrine (Hospira, Inc, Lakes Forest, Illinois, USA) was given. A free oral mucosal graft a little larger than the defect was harvested by demarcating the border with a super blade followed by scissor dissection. The donor site of the oral cavity was covered by Gelfoam (Pharmacia & Upjohn, Kalamazoo, Michigan, USA) soaked with 1000 U/mL thrombin (Gentrac, Inc, Middleton, Wisconsin, USA). For eyes with incomplete closure, the oral mucosal graft was obtained intentionally with more stromal fat ( Figure 1 , Bottom left) so that the tarsal height could be lengthened ( Figure 1 , Bottom right). Otherwise, the excess fat was cleared from the stromal surface of the graft. A continuous 8-0 Vicryl suture was used to secure the stromal edge of the graft to the border of the tarsal defect. Then, the remaining graft was draped over the denuded tarsal edge and was secured tightly to the skin surface of the recessed lid margin using the same running suture and to the orbicularis muscle surface if the skin was scarred by thermal or chemical burns. As a result, the graft adhered tightly to the bed crossover of the eyelid margin ( Figure 1 , Bottom right, inset). The procedure was performed to both upper and lower lids if necessary. Finally, the eye was patched with eye ointment containing 0.3% tobramycin and 0.1% dexamethasone (Alcon Laboratories, Fort Worth, Texas, USA) overnight.