and Mitrofanis Pavlidis2
(1)
Department of Ophthalmology, Uppsala University Hospital, Uppsala, Sweden
(2)
Augencentrum Köln, Cologne, Germany
2.2.2 Inflatable Pillow
2.2.4 Carboband
2.3 Devices
2.3.1 Light Source
2.4.1 Vitrectomy Set
2.4.2 Trocars (Fig. )
2.5.2 Endoillumination
2.5.3 Peeling Instruments
2.6 Miscellaneous
2.6.3 Laser Probe (Fig. )
2.6.4 Fragmatome (Fig. )
2.6.8 Dyes
2.6.9 Sutures
The A and O of a successful vitreoretinal surgery are optimal visualization, optimal instruments and optimal technique. This is different to phacoemulsification surgery. Visualization is also very important in cataract surgery as well as a good phaco machine, but instruments and the technique are of minor importance. Regarding instruments, even for an experienced surgeon, there is a significant difference when using different peeling forceps. Test all available forceps and find the one which is most suitable for you. The vast pathological spectrum from PVR detachment to dislocated IOL requires different instruments, the optimal instrument for the specific indication. The same applies to technique. Every pathology requires an optimal technique. You can operate a dark-brown nucleus with phacoemulsification. But the likelihood that you will encounter a posterior capsular rupture, zonular lysis or decompensated cornea is high. This is not the case, if you use the SICS (modified ECCE) technique. If you operate a difficult PDR with tractional membranes with monomanual vitrectomy, you will likely run into problems such as retinal tears or incomplete removal of the membranes. Insert a chandelier light and things are easy. If you operate an ora serrata dialysis with vitrectomy instead of episcleral buckling, then you made a risky choice because the success rate with buckling surgery is 100 %.
2.1 Optimal Visualization (Figs. 2.1, 2.2 and 2.3)

Fig. 2.1
The EVA vitrectomy machine from DORC. A laser device is integrated and a LED light for illumination. This vitrectomy together with the powerful TDC cutter enables a fast 27G surgery

Fig. 2.2
The Resight system from Zeiss can be only used with Zeiss microscopes. It is easy to use, two lenses (120D and 60D) can be rotated in and the view under air is excellent

Fig. 2.3
An external light source (Brightstar, DORC) gives much more light than an internal light source from a vitrectomy machine. This is especially the case for chandelier lights.
An essential condition for successful surgery is optimal visualization. Do everything to optimize visualization. Even an excellent surgeon cannot unfold his skills, if he does not see well. The main factors for optimal visualization are the BIOM and the endoillumination. The quality of microscopes is high with all manufacturers. Important is moreover the choice of BIOM. Test all available BIOMs in order to find the best suitable BIOM for you. It will directly translate into better surgical quality. Of importance are also the lens and an easy lens change. Many surgeons operate with a 90D lens, which is an excellent compromise lens. But you cannot visualize the periphery well with a 90D lens, which makes it a bad candidate for retinal detachment surgery. We prefer therefore 120D lenses in order to visualize the complete retina and then change to a 60D lens. A good alternative to a 60D lens is a one-way contact lens.
The next important factor for optimal visualization is endoillumination. Three points here are essential: (1) The resterilization of light pipes reduces their quality. Use new light pipes. (2) The usage of an external light source. An external light source such as Brightstar (Fig. 2.3) (DORC) or Photon (Alcon) provides more brightness than an internal light source. An alternative to an external light source is the internal light source of the newest generation of vitrectomy machines such as EVA (DORC), Stellaris PC (B&L) and Constellation (Alcon). The EVA machine has an integrated LED light (Fig. 2.1). Their internal light source is as powerful as an external light source. (3) Choice of chandelier light. The brightness of chandelier lights varies a lot. Test many different chandelier lights until you have found a satisfying solution.
One author (US) uses a Zeiss microscope with a Resight visualization system (Zeiss) (Fig. 2.2). The Resight is simple to use; two different lenses can be rotated into the light beam and the view under air is excellent. Regarding endoillumination he uses an external light source (Photon, Synergetics) or the internal light source from the vitrectomy machine (Constellation and EVA). He uses predominantly the 25G chandelier light Awh from Synergetics for eyes with vitreous body and 25G chandelier lights from DORC and Synergetics for eyes without vitreous body. The latter light probes are inserted with a trocar and are therefore suitable for soft globes. The second author (MP) uses a Zeiss microscope with a Resight visualization system (Zeiss). Regarding endoillumination he uses the internal light source from EVA with a twin light chandelier from DORC or the 29G twin light from Synergetics.
And again: It is worthwhile to set high standards regarding visualization because it influences the surgical quality and outcome directly.
2.2 Operating Room (Figs. 2.4, 2.5, 2.6, 2.7, 2.8, 2.9, 2.10 and 2.11)
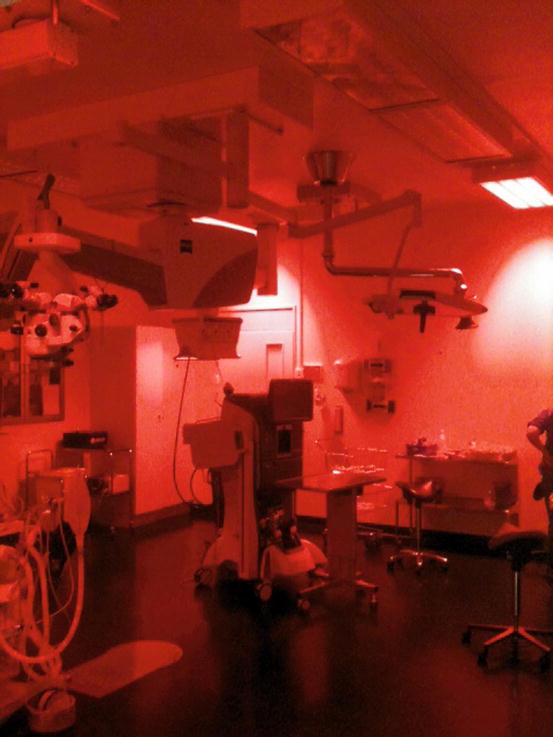
Fig. 2.4
We painted our neon tubes with red colour like in submarines. The red light gives sufficient light and causes much less glare than white light

Fig. 2.5
We use a vacuum pillow which provides a customized positioning and fixation of the patients head

Fig. 2.6
A foot pump is required to pump up the pillow. The complete procedure takes a few seconds (German, Sweden GE22393300000 55 × 30 cm)
Fig. 2.7
The set-up in our OR. We have no assistant and the surgeon indents on his own. There is a large TV screen behind the surgeon for visitors and scrub nurse. The surgeon has a view to a small TV screen on the other side

Fig. 2.8
A photograph of our OR. There is usually no assistant present
Fig. 2.9
The position of the vitrectomy machine, surgical table and scrub nurse varies from OR to OR. This is an alternative set-up with a separate surgical table in front of the surgeon. A vitreous cutter and light pipe are placed on this table. The tubes are fixated with a Velcro fibre tape. The advantage is that the surgeon can access these main instruments on his own
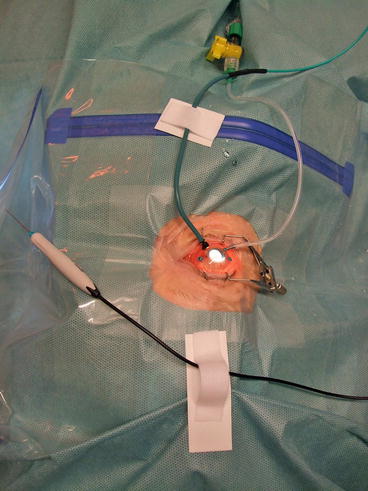
Fig. 2.10
We use a Velcro fibre tape to fasten the tubes of the instruments on the surgical table and on the surgical drape
Fig. 2.11
Package with details of a Velcro fibre tape
2.2.1 Red Lights in the Operating Room
We painted our neon tubes with a red colour like in submarines so that we have a good room illumination without disturbing the surgeon (Fig. 2.4).
2.2.2 Inflatable Pillow
2.2.3 Location of the Patient, Surgeon, Vitrectomy Machine and Scrub Nurse
There are many different set-ups of the patient’s bed, vitrectomy machine and surgical table. Figures 2.7 and 2.8 shows our specific set-up. The disadvantage of this set-up is that the touch screen of the vitrectomy machine is far to be reached for the scrub nurse.
Another possible set-up (Fig. 2.9) is the location of a second surgical table over the breast of the patient. Light pipe and vitreous cutter are placed here constantly, so that these instruments can be accessed by the surgeon.
2.3 Devices
2.3.1 Light Source
The light source is either external or is integrated into the vitrectomy machine. The recent generation of vitrectomy machines (Constellation, Stellaris PC, EVA) has a stronger internal light source which suffices for use of a chandelier light (Fig. 2.1). A good alternative is an external light source such as a photon light source (Synergetics) or a xenon light source (DORC and Alcon) (Fig. 2.3).
2.3.2 Binocular Indirect Ophthalmo Microscope (BIOM) Systems
We use a wide-angle lens (120D) for peripheral vitrectomy and scatter laser photocoagulation (Fig. 2.2). We use a 90D or 60D for peeling of fibrovascular membranes. If you do not have a 60D lens for your BIOM system, then use a plano concave contact lens (1284.DD, DORC). The contact lens provides an excellent zoom and depth perception.
2.4 Instruments for Vitrectomy (Figs. 2.12, 2.13, 2.14, 2.15, 2.16, 2.17, 2.18, 2.19, 2.20, 2.21, 2.22, 2.23, 2.24, 2.25, 2.26, 2.27, 2.28, 2.29, 2.30, 2.31, 2.32, 2.33, 2.34, 2.35, 2.36, 2.37, 2.38, 2.39, 2.40, 2.41, 2.42, 2.43, 2.44, 2.45, 2.46 and 2.47)