Purpose
To evaluate corneal higher-order aberrations (HOAs) and backscattered light before and after Descemet membrane endothelial keratoplasty (DMEK) and their correlation with visual outcome.
Design
Retrospective study.
Methods
In a total of 118 consecutive eyes of 118 patients who underwent uneventful DMEK for Fuchs endothelial dystrophy at a tertiary referral center, best spectacle-corrected visual acuity (BSCVA), corneal HOAs, and backscattered light were evaluated preoperatively and at 6 months postoperatively. Outcome data were compared to an age-matched control group with uncomplicated eyes (n = 27).
Results
Compared to the control group, Fuchs endothelial dystrophy eyes, before as well as 6 months after DMEK, showed higher values of anterior and posterior HOAs and backscattered light ( P < .033). Postoperative anterior HOAs and backscattered light (0–2 mm) were associated with lower 6-month BSCVA (positively related with logMAR BSCVA) ( P ≤ .020). Anterior corneal HOAs did not change from preoperative to 6 months after DMEK ( P = .649), while total posterior HOAs (RMS third to sixth Zernike order) and haze decreased ( P < .001).
Conclusions
Anterior and posterior corneal HOAs, as well as backscattered light from the cornea, were elevated in eyes suffering from Fuchs endothelial dystrophy and remained higher throughout 6 months after DMEK. If present, anterior surface irregularities and anterior corneal haze may be the most important limiting factors in visual rehabilitation after DMEK.
In the last decade, we have introduced various techniques for endothelial keratoplasty (EK), popularized as “deep lamellar endothelial keratoplasty” (DLEK), “Descemet stripping (automated) endothelial keratoplasty” (DSEK/DSAEK), and “Descemet membrane endothelial keratoplasty” (DMEK) for the management of corneal endothelial disease. By replacing only the inner layers of the cornea, the anterior corneal surface is not compromised, minimizing the risk of surgery-induced anterior corneal surface irregularities and providing faster and more complete visual rehabilitation.
However, it has been shown that, also after EK, the final visual outcome may be limited by corneal irregularities or light scatter deriving from the cornea. In DSEK/DSAEK, subnormal visual acuities of 20/30 (0.6) or less are frequently encountered, and have been mentioned to result from irregularities at the stroma-to-stroma interface, haze, or the presence of donor posterior stroma itself. Furthermore, anterior corneal surface irregularities in the posterior EK cornea have been recognized as a potential cause of incomplete visual recovery.
With DMEK, only an isolated Descemet membrane (DM) and its endothelium is transplanted, apparently resulting in near-normal anatomic corneal restoration and visual outcomes up to 20/17 (1.2) or even 20/13 (1.5). If so, a transplanted DMEK cornea may approach the optical quality of a virgin cornea. The purpose of our study was to find evidence for near-normal recovery of optical quality after DMEK by evaluating higher-order aberrations (HOAs) and backscattered light before and after DMEK in a large group of eyes operated on for Fuchs endothelial dystrophy. These parameters were compared to those in virgin corneas to determine to what extent donor-to-host interface irregularities or other postoperative corneal abnormalities may affect the final visual outcome after DMEK.
Methods
Subjects
From a total of 192 consecutive eyes of 165 patients without clinically significant graft detachment or delayed corneal clearance after DMEK surgery for Fuchs endothelial dystrophy (stage 2–4), 118 eyes were included in our retrospective study. In case of a bilateral DMEK (n = 27), only the initial DMEK eye was included. Eyes with visual impairment attributable to maculopathy (n = 14), optic neuropathy (n = 2), or amblyopia (n = 1) were excluded. Also, preexisting corneal scarring (n = 2) and posterior capsular opacities (n = 2) at the 6-month follow-up were exclusion criteria. Furthermore, eyes with incomplete postoperative follow-up data (n = 16) or Pentacam (Oculus, Wetzlar, Germany) measurements not meeting acceptable criteria according to the Pentacam software indications (n = 10) were excluded. Of the 118 eyes of 118 patients (53 male, 65 female), 30 were phakic and 88 pseudophakic. Mean age was 66 (±12) years (range, 33–89 years). An age-matched control group of 27 eyes (23 phakic, 4 pseudophakic) of 27 participants (average age 64 [± 14] years [ P = .434]; 12 male and 15 female) with no history of ocular disease or surgery, except for phacoemulsification in 4 eyes, was recruited for comparison ( Table 1 ).
| DMEK Eyes | Control Eyes | P Value (DMEK-Controls) | |
|---|---|---|---|
| n | 118 | 27 | |
| Male/female | 53/65 | 12/15 | |
| Mean (±SD) age (y) | 66 (±12) | 64 (±14) | .434 |
| Age range (y) | 33–89 | 38–86 | |
| Phakic/pseudophakic | 30/88 | 23/4 |
All participants signed an informed consent for research participation, conducted in compliance with the Institutional Review Board (Dutch “METC” board) and informed consent requirements; this retrospective study of prospectively collected data was conducted according to the Declaration of Helsinki and registered at www.clinicaltrials.gov (study registration NCT00521898 ).
Surgical Procedure
All DMEK surgeries were conducted as previously described. In short, from corneoscleral buttons stored by organ culture at 31°C for 1 week, DM was stripped off, so that a 9.5-mm-diameter flap of posterior DM with its endothelial monolayer was obtained. Owing to the elastic properties of the membrane, a “Descemet roll” formed spontaneously with the endothelium at the outer side. Each Descemet roll was then stored “free-floating” in organ culture medium until the time of transplantation.
In all eyes, a yttrium-aluminum-garnet laser peripheral iridotomy was made at 12 o’clock, 1–2 weeks before surgery (because patients were requested to lie in a supine position for several hours, Bell’s phenomenon may render an iridotomy at the 6-o’clock position ineffective). After the eyes were anesthetized with retrobulbar injection (4 mL 1% ropivacaine hydrochloride with 150 IU Hyason, Riemser Pharma GmbH, Greifswald, Germany), ocular massage, oculopressure with a Honan balloon for 10 minutes, and patient positioning in the anti-Trendelenburg position were done. Three side ports were made, the anterior chamber was filled with air, and a circular portion of DM was scored and stripped from the posterior stroma with a reversed Sinskey hook (D.O.R.C. International, Zuidland, The Netherlands), thereby performing a 9.0-mm-diameter “descemetorhexis”. A 3.0 mm tunnel incision was made at the limbus for insertion of the graft.
The donor Descemet roll was stained with 0.06% trypan blue solution (VisionBlue; D.O.R.C. International) and sucked into a custom-made injector (D.O.R.C. International). The donor Descemet roll was inserted into the anterior chamber and the graft was oriented endothelial side down (donor DM facing recipient posterior stroma). The graft was centered, unfolded, and lifted onto the recipient posterior stroma by careful, indirect manipulation of the tissue with air and fluid. The anterior chamber was completely filled with air for at least 60 minutes, followed by an air-liquid exchange to pressurize the eye.
Examinations
All eyes of participants underwent complete ophthalmologic evaluation and Pentacam rotating Scheimpflug imaging examination. DMEK eyes were examined before and at 1, 3, and 6 months after surgery. Best spectacle-corrected visual acuity (BSCVA) and Pentacam measurements of the preoperative and 6-months-postoperative examinations were used for evaluation. During Pentacam examination, the automatic release mode was used to eliminate operator-induced errors. Only good-quality images of the front and back corneal surfaces were used for analysis.
BSCVA was measured using a forced choice test with a 100% contrast Snellen projection letter chart at 6 meters in mesopic lighting conditions, and was based on the Snellen letter size for which at least 4 out of 5 optotypes were recognized. After converting BSCVA values to logMAR, calculations were performed.
Corneal HOAs were calculated using the Pentacam software (software version 1.17) for Zernike analysis based on height data only, with an ellipsoid fixed eccentricity as a reference, which was from before the release of the Pentacam software providing HOAs based on wavefront data. The software allowed evaluation of HOAs of both anterior and posterior corneal surfaces. The different refractive indices for air, corneal tissue, and aqueous did not have any effect on the data of the Zernike coefficients. The HOAs in the central 6-mm area up to the sixth Zernike order were analyzed. For each pair of Zernike terms, 1 value for its contribution was calculated by Zernike vector analysis. Combinations of individual Zernike terms and total HOAs for each Zernike order were defined as the root mean square (RMS).
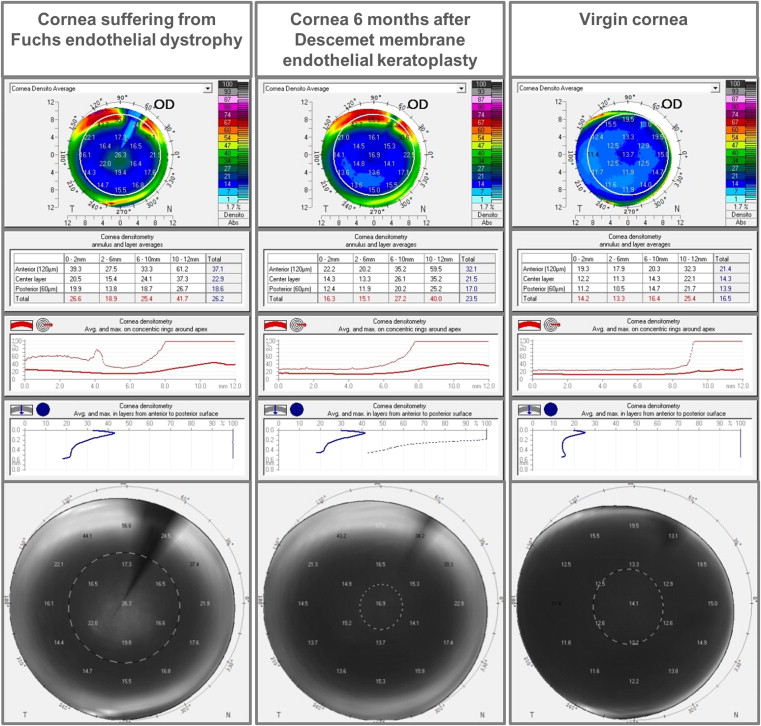
Backscattered light was examined in different layers and zones throughout the cornea with the Pentacam “corneal densitometry” display ( Figure 1 ). To standardize ambient light conditions, all measurements were performed in a windowless clinical assessment room with a uniform ambient light level of 4 lux as measured by a luxmeter (Voltcraft BL-10 L Luxmeter; Conrad Electronic SE, Hirschau, Germany). Additionally, it was analyzed whether the “background” gray scale outside the cornea of the pre-examinations and Pentacam examinations was stable over time for randomly selected cases. Corneal density was quantified on a scale from 0 (no obscuring) to 100 (completely opaque). The software allowed for comparison of the corneal densitometry (backscattered light) in 3 different fixed corneal layers (anterior layer [anterior 120 μm], central layer, posterior layer [posterior 60 μm]), as well as in fixed corneal concentric rings around the apex (central 0–2 mm, 2–6 mm, 6–10 mm, 10–12 mm). For the analysis, the total corneal densitometry was evaluated (backscattered light), as well as the 3 different fixed layers in the 0–2 and 2–6 mm zone.
Statistical Analysis
Statistical analyses were performed using SPSS Statistics 20 and R 2.15.1.
Paired t tests were used to compare preoperative and postoperative measures of HOAs and backscatter for the DMEK group. Because of the high volume of tests performed, alpha inflation and power loss were minimized by controlling the false discovery rate using the method by Benjamini and Hochberg. A P value of <.05 after correction was considered statistically significant.
For comparison between the DMEK and control group, a multivariate analysis of covariance (MANCOVA analysis) was performed with age as a covariate to correct for this parameter. Pearson correlations were obtained to assess relationships between BSCVA, HOAs, and backscattered light. To determine the unique relation of each parameter with postoperative BSCVA and to analyze all parameters simultaneously, a ridge regression analysis (which was necessary owing to the high correlations between the optical quality parameters, which leads to unstable regression weights) was carried out for DMEK eyes vs controls with 6-months-postoperative logMAR BSCVA as a dependent variable and HOAs and backscattered light, along with preoperative logMAR BSCVA and patient demographics, as predictor variables. The relative importance of each predictor is presented as scaled estimate, representing a small, medium, or large effect (values of 0.10, 0.31, or 0.58, respectively). The outcomes of this analysis were corrected for the other included parameters.
Results
In the DMEK group, average logMAR BSCVA improved from 0.42 (±0.24) preoperatively to 0.08 (±0.13) at 6 months postoperatively ( P < .001), representing an improvement in Snellen equivalent of 20/50 (0.4) before to 20/25 (0.8) after DMEK ( Table 2 ). Average logMAR BSCVA in the control group was −0.02 (±0.08) (20/20 [1.0] Snellen equivalent), which differed from BSCVA in preoperative as well as postoperative DMEK eyes ( P < .001) ( Table 2 ).
| DMEK Eyes (n = 118) | |||||
|---|---|---|---|---|---|
| Preoperative, Mean (±SD) | 6 Months FU, Mean (±SD) | Control Eyes (n = 27) Mean (±SD) | DMEK Eyes Preoperative – 6 Months FU P Value a | 6 Months FU DMEK – Control Eyes P Value b | |
| BSCVA (logMAR) | 0.42 (±0.24) | 0.08 (±0.13) | −0.02 (±0.08) | .000 | .000 |
| Central corneal thickness (μm) | 660 (±79) | 519 (±38) | 554 (±33) | .000 | .000 |
| HOAs in central 6 mm (μm) | |||||
| Anterior (RMS 3rd to 6th order) | 0.50 (±0.20) | 0.51 (±0.18) | 0.42 (±0.10) | .649 | .032 |
| Posterior (RMS 3rd to 6th order) | 1.63 (±0.92) | 1.17 (±0.57) | 0.73 (±0.13) | .000 | .001 |
| Densitometry | |||||
| Anterior 0–2 mm | 39.0 (±13.2) | 27.0 (±7.0) | 21.1 (±3.5) | .000 | .001 |
| Anterior 2–6 mm | 31.6 (±8.7) | 25.2 (±6.2) | 20.7 (±4.7) | .000 | .001 |
| Central 0–2 mm | 20.1 (±4.7) | 15.9 (±2.5) | 14.0 (±2.2) | .000 | .001 |
| Central 2–6 mm | 17.7 (±3.9) | 15.7 (±3.1) | 14.0 (±3.3) | .000 | .022 |
| Posterior 0–2 mm | 21.2 (±4.6) | 14.8 (±2.3) | 13.0 (±2.1) | .000 | .001 |
| Posterior 2–6 mm | 17.9 (±4.0) | 15.4 (±3.1) | 12.9 (±2.7) | .000 | .001 |
b MANCOVA (multivariate analysis of covariance) analyses (corrected for age).
From preoperative to 6 months postoperatively, anterior HOAs did not change in DMEK eyes ( P > .1) ( Figure 2 and Table 2 ). All posterior HOAs decreased ( P < .025), except for trefoil and RMS fifth and sixth order ( P > .3) ( Figure 2 and Table 2 ). All densitometry (backscattered light) values improved from preoperative to 6 months postoperatively ( P < .001) ( Figure 1 and Table 2 ).
Compared to the control eyes, DMEK eyes showed higher values of anterior and posterior HOAs (RMS third to sixth Zernike order) and backscattered light ( P < .033) before and 6 months after surgery ( Figures 1 and 2 and Table 2 ).
With Pearson analysis, most optical quality parameters showed a positive correlation with postoperative logMAR BSCVA (ie, negatively affecting Snellen BSCVA), and backscattered light parameters correlated with HOAs ( Table 3 ). Regression analysis showed that the most important predictors for postoperative BSCVA were preoperative BSCVA and patient age ( P < .001) ( Table 4 ). In addition, anterior backscattered light (0–2 mm zone) and anterior HOAs showed a significant positive relation with postoperative logMAR BSCVA, that is, negatively affecting Snellen BSCVA ( P = .015 and P = .020, respectively) ( Table 4 ). All other variables were not related with postoperative BSCVA ( P > .05).
| Pearson Correlations at 6 Months Follow-up | |||||||
|---|---|---|---|---|---|---|---|
| BSCVA (LogMAR) | Anterior HOAs (RMS 3rd to 6th Order) | Posterior HOAs (RMS 3rd to 6th Order) | Anterior Densitometry (0–2 mm) | Anterior Densitometry (2–6 mm) | Posterior Densitometry (0–2 mm) | Posterior Densitometry (2–6 mm) | |
| BSCVA (logMAR) | |||||||
| Pearson correlation (r) | 1 | 0.427 b | 0.364 b | 0.371 b | 0.343 b | 0.244 b | 0.254 b |
| Significance (2-tailed) | 0.000 | 0.000 | 0.000 | 0.000 | 0.003 | 0.002 | |
| n = | 145 | 145 | 145 | 145 | 145 | 145 | 145 |
| Anterior HOAs (RMS 3rd to 6th order) | |||||||
| Pearson correlation (r) | 0.427 b | 1 | 0.438 b | 0.366 b | 0.278 b | 0.112 | 0.160 |
| Significance (2-tailed) | 0.000 | 0.000 | 0.000 | 0.001 | 0.179 | 0.054 | |
| n = | 145 | 145 | 145 | 145 | 145 | 145 | 145 |
| Posterior HOAs (RMS 3rd to 6th order) | |||||||
| Pearson correlation (r) | 0.364 b | 0.438 b | 1 | 0.299 b | 0.346 b | 0.185 a | 0.364 b |
| Significance (2-tailed) | 0.000 | 0.000 | 0.000 | 0.000 | 0.026 | 0.000 | |
| n = | 145 | 145 | 145 | 145 | 145 | 145 | 145 |
| Anterior densitometry (0–2 mm) | |||||||
| Pearson correlation (r) | 0.371 b | 0.366 b | 0.299 b | 1 | 0.891 b | 0.573 b | 0.451 b |
| Significance (2-tailed) | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 | |
| n = | 145 | 145 | 145 | 145 | 145 | 145 | 145 |
| Anterior densitometry (2–6 mm) | |||||||
| Pearson correlation (r) | 0.343 b | 0.278 b | 0.346 b | 0.891 b | 1 | 0.595 b | 0.612 b |
| Significance (2-tailed) | 0.000 | 0.001 | 0.000 | 0.000 | 0.000 | 0.000 | |
| n = | 145 | 145 | 145 | 145 | 145 | 145 | 145 |
| Posterior densitometry (0–2 mm) | |||||||
| Pearson correlation (r) | 0.244 b | 0.112 | 0.185 a | 0.573 b | 0.595 b | 1 | 0.818 b |
| Significance (2-tailed) | 0.003 | 0.179 | 0.026 | 0.000 | 0.000 | 0.000 | |
| n = | 145 | 145 | 145 | 145 | 145 | 145 | 145 |
| Posterior densitometry (2–6 mm) | |||||||
| Pearson correlation (r) | 0.254 b | 0.160 | 0.364 b | 0.451 b | 0.612 b | 0.818 b | 1 |
| Significance (2-tailed) | 0.002 | 0.054 | 0.000 | 0.000 | 0.000 | 0.000 | |
| n = | 145 | 145 | 145 | 145 | 145 | 145 | 145 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


