Purpose
To describe the optical coherence tomography (OCT) findings in eyes with active anterior scleritis and compare the findings to those with episcleritis and normal controls.
Design
Prospective evaluation of a diagnostic test.
Methods
We included a total of 30 eyes of 30 patients with unilateral anterior scleral or episcleral inflammation. The contralateral 30 eyes with no active ocular disease served as controls. OCT was performed over the anterior sclera in the inflamed area on all cases. The OCT images were analyzed to determine the thickness of the sclera and the presence or absence of scleral hyporeflective areas representing intrascleral edema.
Results
There were 17 male and 13 female patients. The mean age was 43 years with an age range of 21–77 years. Eighteen patients had anterior scleritis and 12 patients had episcleritis. The mean transconjunctival scleral thickness was 747 μm (SD ± 68.97) with a range of 616–877 μm in normal eyes, 882 μm (SD ± 87.35) with a range of 773–1089 μm in patients with scleritis, and 825 μm (SD ± 85.57) with a range of 718–949 μm in patients with episcleritis.
Conclusions
Patients with active anterior scleritis showed increased thickness of the sclera and presence of intrascleral hyporeflective areas of edema by OCT compared to patients with episcleritis and normal eyes. OCT adds both qualitative and quantitative information to diagnosis and monitoring of patients with scleritis.
The sclera is a collagenous layer that provides structural integrity to the globe. Involvement of the sclera by inflammation can give rise to variable clinical manifestations ranging from mild self-limiting episodes to a more severe form of scleritis. Clinically anterior scleritis may have several distinct patterns including diffuse scleritis, nodular scleritis, and necrotizing scleritis (with or without inflammation). However, there may be some slight overlap between the groups. The majority of cases of necrotizing scleritis usually have an underlying autoimmune or infectious etiology. Treating the underlying cause may alter favorably the general as well as the ocular prognosis in these patients. Differentiation between episcleritis and scleritis is important for the diagnosis and management. The clinical course and visual prognosis may be different. Furthermore, patients with the diagnosis of scleritis may be associated with underlying systemic diseases, which may be fatal in some cases.
Differentiation between the 2 forms of inflammation, scleritis and episcleritis, could be guided by obtaining careful history and performing appropriate clinical examinations. In some cases, however, the differentiation between scleritis and episcleritis may be difficult. Unfortunately, there are limited methods for differentiating one from the other and there is no objective test to establish the diagnosis. The aim of this study is to characterize the optical coherence tomography (OCT) findings in eyes with scleral inflammation and compare the findings to normal controls. We decided to use a noninvasive diagnostic test by OCT to differentiate between scleritis and episcleritis.
Patients and Methods
The protocol was approved by The Eye Center institutional review board. Patients gave informed consent to participate in this research study. The study was adherent to the tenets of the Declaration of Helsinki and was registered at clinicaltrials.gov (registration number is NTC 01958567). A total of 30 eyes of consecutive patients were included. All patients had the clinical diagnosis of unilateral scleral or episcleral inflammation in the period from June 2012 to December 2013. The contralateral 30 eyes with no active ocular disease served as controls. The diagnosis of episcleritis consisted of symptoms of acute onset of mild ocular discomfort or occasional pain localized to the eye with mild tenderness and superficial episcleral hyperemia. The clinical diagnosis of scleritis was made based on symptoms of gradual onset of more severe ocular pain that radiates to the surrounding tissues, moderate to severe tenderness, photophobia, and blurring of vision and signs of congestion. The congestion was noted maximally in the deep episcleral network with some congestion in the superficial episcleral network, by both external daylight examination and slit-lamp biomicroscopy.
Patients had complete eye examinations. Medical evaluation by an internist was carried out as required and laboratory investigations were performed whenever indicated. Other causes of red eye were excluded. The inclusion criteria were patients over the age of 18 years with clinical signs of anterior scleritis or episcleritis. The exclusion criteria consisted of patients suffering from other causes of ocular surface inflammation such as infectious keratitis or conjunctivitis, pterygia and pingueculae, and patients 18 years or younger. OCT of the anterior sclera in the inflamed area was performed on all cases using spectral-domain OCT (3D OCT-2000; Topcon Corp, Tokyo, Japan). In order to achieve accurate measurements, we asked all patients to look at a fixation target to ensure that the orientation of the desired area is perpendicular to the incoming light wave from the OCT machine. The same beam orientation was used for the eyes with anterior scleritis as well as the control eyes.
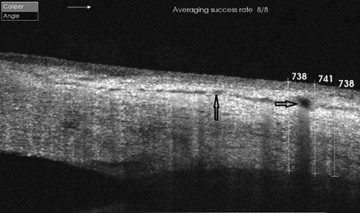
The OCT images were assessed to detect the presence or absence of scleral hyporeflective areas representing intrascleral edema. The thickness and consistency of conjunctiva, episclera, and sclera was measured in all cases. The inclusion of the tissues overlying the sclera in the measured thickness was owing to the inability to precisely identify the borders of the sclera from the overlying fused episclera. Measurement of thickness was done by obtaining the average of 3 readings, which were done on the inflamed sclera midway between the limbus and the site of insertion of the rectus muscle ( Figure 1 ). The measurements were done on areas of diffuse involvement avoiding areas of irregularities or nodular appearance. The exact same area was imaged in control eyes and corresponding images were compared with study eyes.
Statistical Analysis
ANOVA test was used to compare the groups of eyes. Statistical significance was defined as a P value of less than .05.
Results
There were a total of 30 patients. All patients had the clinical diagnosis of anterior scleral or episcleral inflammation. There were 17 male and 13 female patients. The mean age was 43 years with an age range of 21–77 years. The main presenting symptoms in our patients with episcleritis were redness and mild ocular pain, which was localized to the eye; in patients with scleritis the main presenting symptoms were moderate to severe ocular pain that radiates to the eyebrow and sinuses, severe tenderness, redness, photophobia, decreased visual acuity, and foreign body sensation. Clinically, in cases of episcleritis the maximum congestion was noted superficially and in cases of scleritis the maximum congestion was noted deeper. OCT of the sclera in the 30 normal control eyes revealed scleral thickness of 747 μm (range; 616–877, SD ± 68.97) ( Figure 1 ). In the 18 patients with the clinical diagnosis of scleritis, OCT scans of the sclera revealed hyporeflective areas representing intrascleral edema ( Figure 2 ). The eyes with scleral involvement showed increased scleral thickness on OCT sections with a mean thickness of 882 μm (range: 773–1089, SD ± 87.35) ( P = .001). In the 12 patients with the clinical diagnosis of episcleritis, OCT showed predominant involvement of the episclera without involvement of the sclera by hyporeflective areas ( Figure 3 ) and a mean thickness of 825 μm (range: 718–949, SD ± 85.57) ( P = .003).



