Optic neuritis is a term used to refer to inflammation of the optic nerve. When it is associated with a swollen optic disc, it is called papillitis or anterior optic neuritis. When the optic disc appears normal, the terms retrobulbar optic neuritis or retrobulbar neuritis are used. In the absence of signs of multiple sclerosis (MS) or other systemic disease, the optic neuritis is referred to as isolated, monosymptomatic, or idiopathic. The pathogenesis of isolated optic neuritis is presumed to be demyelination of the optic nerve, similar to that seen in MS. It is likely that most cases of isolated acute optic neuritis are a forme fruste of MS.
Optic neuritis can be caused by disorders other than MS and related demyelinating diseases. In addition, two variants of optic neuritis occasionally occur. Neuroretinitis is a term used to describe inflammatory involvement of both the intraocular optic nerve and the peripapillary retina. Optic perineuritis, also called “perioptic neuritis,” describes inflammatory involvement of the optic nerve sheath, without inflammation of the nerve itself.
Idiopathic Demyelinating Optic Neuritis
Optic neuritis usually is a primary demyelinating process. It almost always occurs as an isolated phenomenon or in patients with MS. Patients in whom optic neuritis occurs as an isolated phenomenon have a higher risk of the subsequent development of MS than the normal population. There are three forms of primary demyelinating optic neuritis: acute, chronic, and subclinical.
Acute Idiopathic Demyelinating Optic Neuritis
Acute demyelinating optic neuritis is by far the most common type of optic neuritis that occurs throughout the world and is the most frequent cause of optic nerve dysfunction in the young adult population. Much of our knowledge regarding this form of optic neuritis was obtained from the Optic Neuritis Treatment Trial (ONTT), a prospective study in which patients with a first episode of unilateral optic neuritis were randomized to corticosteroid treatment (either intravenous or oral) or placebo. The investigators in this trial enrolled 455 patients with acute unilateral optic neuritis. Although the primary objective of the trial was the assessment of the efficacy of corticosteroids in the treatment of optic neuritis, the trial also provided information about the clinical profile of optic neuritis, its natural history, and its relationship to MS.
Demographics
The annual incidence of acute optic neuritis is estimated in population-based studies to be between 1 and 5 per 100,000. In Olmstead County, Minnesota, where the Mayo Clinic is located, the incidence rate is estimated to be 5.1 per 100,000 person-years and the prevalence rate 115 per 100,000.
Clinical Presentation
The two major symptoms in patients with acute optic neuritis are loss of central vision and pain in and around the affected eye.
Loss of central visual acuity is reported by over 90% of patients. Vision loss is typically abrupt, occurring over several hours to several days. Progression over a longer period of time can occur but should make the clinician suspicious of an alternative disorder. The majority of patients describe diffuse blurred vision, although some recognize that the blurring is predominantly central. Occasionally, patients complain of a loss of a portion of peripheral field, such as the inferior or superior region, often to one side. The visual loss is monocular in most cases, but in a small percentage, particularly in children, both eyes are simultaneously affected.
Pain in or around the eye is present in more than 90% of patients with acute optic neuritis. It is usually mild, but it may be severe and even more debilitating to the patient than the loss of vision. It may precede or occur concurrently with visual loss, usually is exacerbated by eye movement, and generally lasts no more than a few days. The presence of pain helps differentiate this condition from other causes of optic neuropathies such as anterior ischemic optic neuropathy, which typically produces painless visual loss (see Chapter 7).
Up to 30% of patients with optic neuritis experience positive visual phenomena, called photopsias, both at the onset of their visual symptoms and during the course of the disorder. These phenomena are spontaneous flashing black squares, flashes of light, or showers of sparks, sometimes precipitated by eye movement or certain sounds.
Examination of a patient with acute optic neuritis reveals evidence of optic nerve dysfunction. Visual acuity is reduced in most cases but varies from a mild reduction to no light perception. Contrast sensitivity and color vision are impaired in almost all cases. The reduction in contrast sensitivity is typically worse than the visual acuity loss, as is the reduction in color plate recognition (Ishihara or Hardy–Rand–Rittler). Even when the patient can detect all the pseudoisochromatic figures correctly, careful comparison of the appearance of a single plate by each eye may reveal a striking difference in color and brightness between the two eyes.
Visual field loss can vary from mild to severe, may be diffuse or focal, and can involve the central or peripheral field. Indeed, almost any type of field defect can occur in an eye with optic neuritis. Among 415 patients in the ONTT with baseline visual acuity of hand motions or better, automated perimetry of the central 30 degrees of visual field revealed diffuse visual field loss in 48% of patients and focal loss in 52%. Focal nerve fiber bundle type defects (altitudinal, arcuate, and nasal step) were present in 20% of patients; pure central or centrocecal defects in 8%; and hemianopic defects in 5%.
A relative afferent pupillary defect is demonstrable in almost all unilateral cases of optic neuritis. When such a defect is not present, either there is a coexisting optic neuropathy in the fellow eye (e.g., from previous or concurrent asymptomatic optic neuritis), or the visual loss cannot be attributed to optic neuritis or another optic neuropathy.
Patients with optic neuritis also can be shown to have a reduced sensation of brightness in the affected eye, either by simply asking them to compare the brightness of a light shined in one eye and then the other, or by more complex tests using polarized lenses or flickering lights of varying frequencies.
 Figure 6.1 Anterior optic neuritis. There is significant swelling and hyperemia of the disc with dilated surface capillaries. |
About one-third of Caucasian patients with acute optic neuritis have some degree of disc swelling (Fig. 6.1); disc swelling is more prevalent in optic neuritis patients of Asian, African, and Caribbean origin. Although the swelling is usually mild, it may be so severe that it mimics the choked disc seen in patients with papilledema (Fig. 6.2). The degree of disc swelling does not correlate with the severity of either visual acuity or visual field loss. Disc or peripapillary hemorrhages and segmental disc swelling are less common in eyes with acute optic neuritis than in eyes with anterior ischemic optic neuropathy. Over approximately 4 to 6 weeks, the optic disc may become pale, even as the
visual acuity and other parameters of vision improve (Fig. 6.3). The pallor may be diffuse or sectoral, most often in the temporal region.
visual acuity and other parameters of vision improve (Fig. 6.3). The pallor may be diffuse or sectoral, most often in the temporal region.
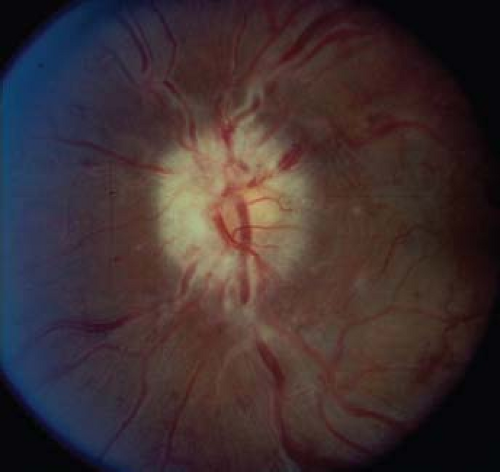 Figure 6.2 Severe anterior optic neuritis mimicking papilledema. Note hyperemia and elevation of the disc and several peripapillary retinal hemorrhages. |
Slit lamp examination in eyes with demyelinating optic neuritis is almost always normal, but a very mild anterior or posterior uveitis may be observed. Sheathing of retinal veins may also occur, especially in patients with MS. When the cellular reaction is extensive, etiologies other than demyelination should be considered, including sarcoidosis, syphilis, catscratch disease, and Lyme disease (see p. 140, Infectious and Parainfectious Optic Neuritis).
Bilateral simultaneous acute optic neuritis is uncommon in adults, although the relative frequency increases when evaluating populations of patients with established MS. The ONTT showed a relatively high percentage of presumably asymptomatic fellow eye deficits at baseline: 14% with visual acuity abnormalities, 22% with color vision abnormalities, and 48% with visual field defects. The majority of the fellow eye deficits resolved over several months, suggesting that such abnormalities may be caused by subclinical but concurrent acute demyelination in the fellow optic nerve. In contrast to adults, acute optic neuritis is often symptomatically bilateral and simultaneous in children and is presumed related to infection (see p. 142, Optic Neuritis in Children).
Diagnostic Studies
Studies in patients with presumed acute optic neuritis are performed for one of three reasons: (1) to exclude another cause of optic neuropathy, particularly a compressive lesion; (2) to determine if a process other than demyelination is responsible for optic nerve inflammation; and (3) to determine the visual and neurologic prognosis.
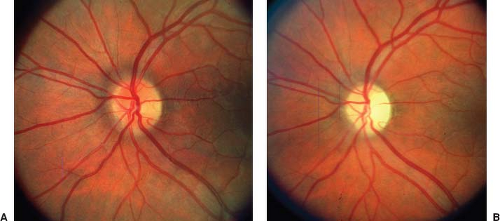 Figure 6.3 Optic atrophy after acute, retrobulbar optic neuritis. A: In acute phase, visual acuity in the left eye is 20/300 with a central scotoma, but the optic disc is normal. B: Three months later, visual acuity has returned to 20/30, but the optic disc is pale, particularly temporally, and there is mild nerve fiber layer atrophy. |
With the widespread availability of magnetic resonance imaging (MRI), computed tomographic (CT) scanning has little or no role in the evaluation of patients with presumed optic neuritis. MRI will show optic nerve enlargement, T2 hyperintensity, and/or enhancement with gadolinium contrast in most cases of optic neuritis (Fig. 6.4). However, these findings are nonspecific, as a similar appearance can be observed in patients with infectious, and other inflammatory optic neuropathies. The most important application of MRI
in patients with optic neuritis is in the identification of signal abnormalities in the white matter of the brain, usually in the periventricular region, consistent with demyelination (Fig. 6.5).
in patients with optic neuritis is in the identification of signal abnormalities in the white matter of the brain, usually in the periventricular region, consistent with demyelination (Fig. 6.5).
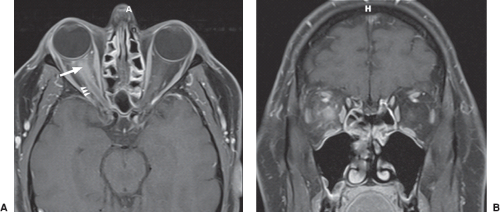 Figure 6.4 Magnetic resonance imaging (MRI), T1 weighted with gadolinium contrast and fat saturation, of the optic nerve in acute demyelinating optic neuritis. A: Axial image shows enhancement of the right optic nerve (arrow) with “spillover” to the optic nerve sheath leading to enhancement of this structure as well (arrowheads). B: Coronal image shows enlargement and enhancement of the right optic nerve. |
Other tests are similarly nonspecific in differentiating acute demyelinating optic neuritis from the less common systemic and local infectious and inflammatory optic neuropathies, and obtaining a thorough medical history is required to identify patients who may need additional testing. Therefore, diagnostic testing should be performed on a case-by-case basis to rule out common disorders such as syphilis, sarcoidosis, catscratch disease, Lyme disease, or systemic lupus erythematosus (SLE).
 Figure 6.5 Magnetic resonance imaging (MRI) of the brain of a patient with isolated optic neuritis and no previous history of neurologic dysfunction. T2/FLAIR-weighted sagittal MRI shows multiple ovoid periventricular white-matter lesions. |
The role of CSF analysis in the evaluation of patients with acute optic neuritis is not clear. Although the presence of oligoclonal banding in the CSF is associated with the development of MS, the powerful predictive value of brain MRI for MS has reduced the role of lumbar puncture in the evaluation of patients with optic neuritis. Lumbar puncture can help define a very low risk population for MS if both CSF and MRI are normal. CSF studies in patients with optic neuritis are mostly useful to rule out another inflammatory or infectious disorder.
Visual Prognosis
The natural history of acute demyelinating optic neuritis is to worsen over several days to 2 weeks, and then to improve. Initial recovery is usually rapid and then slows, but further improvement may occur for 1 year after the onset of visual symptoms. Among patients in the ONTT who received placebo, visual acuity began to improve within 3 weeks of onset in 79% and within 5 weeks in 93%. For most patients in this study, recovery of visual acuity was nearly complete by 5 weeks after onset. Two-thirds of patients recover central acuity of 20/20 or better, and less than 15% of patients have worse acuity than 20/40. Other parameters of visual function, including contrast sensitivity, color
perception, and visual field, improve in conjunction with improvement in visual acuity.
perception, and visual field, improve in conjunction with improvement in visual acuity.
Although the overall prognosis for visual acuity after an attack of acute optic neuritis is extremely good, some patients have persistent severe visual loss after a single episode. Furthermore, even patients with improvement in visual function to “normal” may complain of movement-induced photopsias or transient loss of vision with overheating or exercise (Uhthoff symptom). Uhthoff symptom is most common in patients with other evidence of MS, but it is also experienced after isolated optic neuritis, by patients with chronic or subclinical optic neuritis, and occasionally by patients with optic neuropathies from other causes. Two major hypotheses regarding Uhthoff symptom are that (1) elevation of body temperature interferes directly with axon conduction, and (2) exercise or a rise in body temperature changes the metabolic environment of the axon, which, in turn, interferes with conduction.
Subjectively, patients with recovered optic neuritis frequently complain that their vision in the affected eye is “not right,” or that colors are “washed out.” One cause of these symptoms is probably related to subtle abnormalities in the visual field in which patients experience abnormally rapid disappearance of focal visual stimuli and abnormally rapid fatigue in sensitivity. These patients typically complain that when they look at something, it appears as if they have “holes” in their vision.
Recurrent attacks of optic neuritis may occur in either eye. The 10-year ONTT recurrence rate was 35%. The risk of recurrence was increased (41%) in the ONTT group treated with oral steroids compared with those receiving intravenous steroids or placebo (25%).
Neurologic Prognosis
Optic neuritis occurs in about 50% of patients with MS and is the presenting manifestation in about 20%. Both retrospective and prospective studies have been performed to determine the prognosis for the development of MS in patients who experience an attack of acute optic neuritis. Although retrospective studies provide figures ranging from 11.5% to 85%, most prospective studies support the higher figures. Among 95 incident cases of optic neuritis in Olmstead County, Minnesota, the estimated risk of MS was 39% by 10 years, 49% by 20 years, 54% by 30 years, and 60% by 40 years. The average time interval from an initial attack of optic neuritis until other symptoms and signs of MS develop varies considerably; most studies found that the majority of persons who develop MS after optic neuritis do so within 7 years of the onset of visual symptoms.
Without question, the most highly predictive baseline factor for progression to MS is the presence of one or more lesions in the periventricular white matter on MRI, a phenomenon noted in 50% to 70% of patients with isolated optic neuritis. This was demonstrated by several studies, including the ONTT. Among patients with isolated optic neuritis in the ONTT, the cumulative percentage developing MS within 5 years was 16% in patients with normal MRI and 51% in patients with more than two lesions on the brain MRI. At 15 years from onset of optic neuritis, 72% of patients with even one typical MRI lesion at baseline (regardless of the number of lesions) had developed MS, while only 25% of those who had a normal MRI at baseline had developed MS (Fig. 6.6). Other risk factors for the development of MS among ONTT patients were Caucasian race, a family history of MS, history of previous ill-defined neurologic complaints, and a previous episode of optic neuritis. However, none of these factors affected the risk of developing MS as much as the results of MRI. Among patients with normal MRI, negative risk factors included male gender, absence of pain, mild visual acuity loss, and optic disc swelling. Although the ONTT did not support any correlation between age of onset and the development of MS, other studies suggest that the younger the age of onset of optic neuritis, the greater the subsequent risk for MS. Winter onset of optic neuritis also may be a risk factor.
The ONTT and the Longitudinal Optic Neuritis Study (LONS) have revealed a particularly low MS-risk group. Among the patients who had a normal brain MRI, none of the patients with severe disc edema, macular star, or disc hemorrhages developed MS at 15 years. These findings emphasize the role of the ophthalmologist in defining the prognosis of optic neuritis.



