Normal and Abnormal Eyelid Function
Disorders of neuro-ophthalmologic significance may affect not only visual sensory, ocular motor, and pupil function but also the function of the eyelids. Indeed, the inability of a patient to fully open or close his or her eyelids may be the first sign of a more extensive process, the early diagnosis and treatment of which may be crucial to the ultimate well being of the patient. This chapter describes the elements that make up a complete assessment of eyelid function, the anatomy of the structures that provide normal eyelid function, and the various pathologic processes that impair eyelid opening and closure. We focus on eyelid disorders of neuro-ophthalmologic significance and direct the reader to oculoplastic texts for coverage of other causes of ptosis.
Examination of Eyelid Function
Detailed observation of eyelid position and movement is an important but often neglected part of the neuro-ophthalmologic examination (Table 22.1). In evaluating the eyelids, one should note the resting position of the upper and lower eyelids, assess the ability of the upper eyelid to open and close, and observe the various settings in which eyelid opening and closing occur, including voluntary, reflex, and spontaneous blinking, and lid movements accompanying eye movements.
Patients with eyelid dysfunction often complain of visual problems. Many of these problems are neurologic in origin. For example, laxity of the eyelids from a facial palsy can cause exposure keratopathy with associated blurring of vision, ocular pain, and tearing. However, the same clinical symptoms can also result from involutional changes in the elastic connective tissue supporting the lids. Ptosis, which also can be neurologic and nonneurologic in origin, can produce visual problems, even when incomplete, if the eyelashes or lid margin cover the pupil. When obtaining a history, it is important to inquire about the onset, duration and progression of the problem, and fluctuations of symptoms at different times of the day, in different seasons, and in different environmental conditions. Systemic diseases often affect eyelid function, but patients may have no reason to associate them with their eye problems. Therefore, a thorough medical history with particular attention to thyroid conditions, diabetes mellitus, systemic hypertension, myopathies, myasthenia gravis, sarcoidosis, and facial paresis should be obtained. In many situations, old photographs are useful in establishing the presence of a pre-existing condition such as ptosis or eyelid retraction, which may have only recently become symptomatic or noticed by the patient.
The detailed examination of the eyelids should proceed as outlined in Table 22.1, with the examiner noting any abnormalities or asymmetries. In addition, because abnormalities of eyelid position, function, or both often are associated with other neuro-ophthalmic signs, a complete eyelid evaluation must be accompanied by an assessment of visual sensory function, ocular motility and alignment, pupil function, function of the trigeminal and facial nerves, and the status of the orbit, particularly for signs of orbital disease such as proptosis or enophthalmos.
All lid movements result from the interaction of four simple forces: (a) an active closing force produced by the orbicularis oculi muscle; (b) an active opening force generated by the levator palpebrae superioris muscle (often called the levator muscle or, simply, “the levator”); (c) an active opening force generated by a smooth muscle—Müller muscle (also called the superior tarsal muscle); and (d) passive lid-closing forces produced by stretching of ligaments and tendons of the eyelid. For example, normal blinks result from a cessation of the tonically active levator followed by a transient burst
of the normally quiescent orbicularis oculi. The active orbicularis oculi force combined with passive lid-closing forces rapidly lower the lid. When the orbicularis oculi activity terminates, the tonic levator activity resumes. This action slowly raises the eyelid until the passive closing forces match the active opening forces generated by the levator. Moving the lid in conjunction with vertical eye movements involves changes only in the activity of the levator. This muscle receives an eye movement input qualitatively identical with that of its developmental progenitor, the superior rectus muscle. As the eye elevates, the tonic activity on the levator increases and raises the eyelid. With decreases in levator activity, the passive downward forces pull the lid down until the passive closing and active opening forces again match. By understanding these forces, it is possible to determine which element or elements of the lid system are affected by a local, systemic, or neurologic disorder.
of the normally quiescent orbicularis oculi. The active orbicularis oculi force combined with passive lid-closing forces rapidly lower the lid. When the orbicularis oculi activity terminates, the tonic levator activity resumes. This action slowly raises the eyelid until the passive closing forces match the active opening forces generated by the levator. Moving the lid in conjunction with vertical eye movements involves changes only in the activity of the levator. This muscle receives an eye movement input qualitatively identical with that of its developmental progenitor, the superior rectus muscle. As the eye elevates, the tonic activity on the levator increases and raises the eyelid. With decreases in levator activity, the passive downward forces pull the lid down until the passive closing and active opening forces again match. By understanding these forces, it is possible to determine which element or elements of the lid system are affected by a local, systemic, or neurologic disorder.
Table 22.1 Examination of the Eyelids | |
|---|---|
|
Anatomy of the Eyelids
The eyelids contain three main muscles innervated by three different neural networks. The oculomotor nerve (see Chapter 18) provides innervation to the levator palpebrae superioris muscle that keeps the eyelids open, a function assisted somewhat by Müller muscle, which is innervated by the sympathetic nervous system. Eyelid closure is achieved by contraction of the orbicularis oculi muscle, innervated by the facial nerve (see below).
Anatomy of the Muscles of Eyelid Opening
The principal muscle involved in opening the upper eyelid and in maintaining normal lid posture is the levator palpebrae superioris. Two accessory muscles of lid opening, Müller muscle and the frontalis muscle, play only minor roles.
Levator Palpebrae Superioris
The levator palpebrae superioris muscle originates at the annulus of Zinn and courses anteriorly along the superior aspect of the orbit, passing through a suspensory structure, Whitnall ligament (also called the superior transverse ligament), to which it is attached by bands of connective tissue (Fig. 22.1). The levator does not extend all the way from its origin to the superior tarsus. Instead, it begins to gradually transition from muscle to tendon just posterior to Whitnall ligament. Anterior to Whitnall ligament, it exists only as a tendinous aponeurosis. It is this aponeurosis that fuses with the orbital septum and attaches to the superior tarsus. The levator palpebrae superioris is innervated by branches of the superior division of the oculomotor nerve.
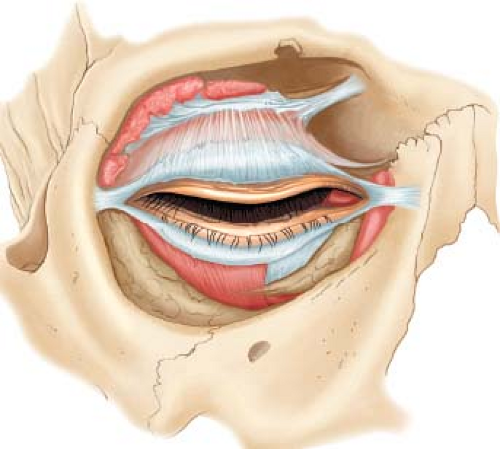 Figure 22.1 Anatomy of the levator palpebrae superioris muscle and its aponeurosis. |
Müller Muscle
Müller muscle is a thin band of smooth muscle about 10 mm in width that inserts on the superior border of
the upper tarsus (Fig. 22.2). The muscle originates 10 to 12 mm above the tarsus from tendons inserted near the origin of the levator aponeurosis. Müller’s muscle is innervated by fibers of the oculosympathetic pathway.
the upper tarsus (Fig. 22.2). The muscle originates 10 to 12 mm above the tarsus from tendons inserted near the origin of the levator aponeurosis. Müller’s muscle is innervated by fibers of the oculosympathetic pathway.
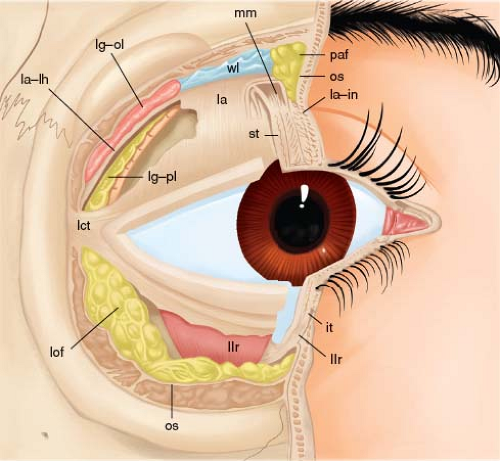 Figure 22.2 Anatomy of Müller muscle. Anterior view of transected and partially dissected upper and lower eyelids. The lateral portion of the orbital septum and the levator have been excised to demonstrate adjacent relationships. Note that Müller muscle (mm) is located just underneath the levator aponeurosis (la) and inserts directly into the upper aspect of the superior tarsus (st), whereas the levator aponeurosis inserts into the anterior aspect of the tarsus (la-in). it, inferior tarsus; la-lh, lateral horn of levator aponeurosis; lct, lateral canthal tendon; lg-ol, orbital lobe of lacrimal gland; lg-pl, palpebral lobe of lacrimal gland; llr, lower lid retractors; lof, lateral orbital fat; os, orbital septum (cut edge); paf, preaponeurotic fat; wl, Whitnall ligament. (Reprinted with permission from Rootman J, Stewart B, Goldberg RA. Orbital Surgery: A Conceptual Approach. Philadelphia, PA: Lippincott-Raven, 1995.) |
Although Müller muscle is located in the upper eyelid, there is a similar, much smaller, sympathetically innervated muscle located in the lower eyelid. Hypofunction of this muscle (such as occurs in Horner syndrome) results in slight elevation of the lower eyelid (“upside-down” ptosis).
Frontalis and Associated Muscles
The muscles controlling the eyebrow contribute to the eyelid appearance and, to a lesser extent, its elevation. Control of the eyebrow involves three sets of muscles: frontalis, procerus, and corrugator superciliaris (Fig. 22.3). The frontalis has cutaneous insertions at the level of the eyebrow, and frontalis fibers also intermingle with peripheral orbicularis oculi muscle fibers. Contraction of the frontalis raises the entire eyebrow and the upper eyelid through its cutaneous and orbicularis
oculi connections. The procerus muscle originates from the medial portion of the lower region of the frontalis muscle and inserts on the nasal bone. Contraction of this muscle pulls the medial portion of the eyebrow downward. The corrugator supraciliaris originates from the frontal bone and lies beneath the frontalis and orbicularis oculi. It extends 2 to 3 cm laterally, where it blends with the frontalis and orbicularis oculi fibers. Contraction of the corrugator supraciliaris pulls the eyebrow medially and downward.
oculi connections. The procerus muscle originates from the medial portion of the lower region of the frontalis muscle and inserts on the nasal bone. Contraction of this muscle pulls the medial portion of the eyebrow downward. The corrugator supraciliaris originates from the frontal bone and lies beneath the frontalis and orbicularis oculi. It extends 2 to 3 cm laterally, where it blends with the frontalis and orbicularis oculi fibers. Contraction of the corrugator supraciliaris pulls the eyebrow medially and downward.
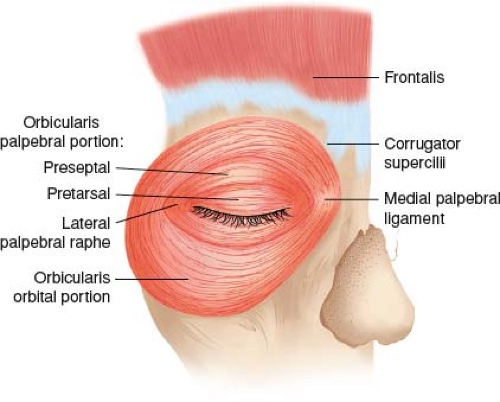 Figure 22.3 Anatomy of the orbicularis oculi, frontalis, procerus, and corrugator muscles. |
Anatomy of the Muscles of Eyelid Closure
The primary muscle responsible for eyelid closure, the orbicularis oculi, is a typical striated muscle. It completely covers the orbital opening, forming concentric rings around the palpebral fissure and surrounding bone (Fig. 22.3). It is responsible not only for active eyelid closure, but also for much of the facial expression around the eyes. It can be divided into three parts: orbital, preseptal, and pretarsal.
Abnormalities of Eyelid Opening
Abnormalities of eyelid opening include ptosis—insufficient opening of the eyelid—which can be caused by a variety of congenital and acquired disorders, many of which are of neuro-ophthalmologic importance, apraxia of eyelid opening (AEO) caused by supranuclear inhibition of levator function, and eyelid retraction, the only pathognomonic sign of thyroid eye disease and an important sign of other neuropathic, neuromuscular, myopathic, and mechanical disorders.
Ptosis
A deficiency of levator tonus produces the clinical sign called blepharoptosis or ptosis. Ptosis may be produced by damage to the motor system controlling eyelid elevation and position at any point along the pathway, from the cerebral cortex to the levator muscle itself. Topical diagnosis of ptosis depends on the character of the deficiency and on evidence of neuropathic, neuromuscular, aponeurotic, developmental, mechanical, or myopathic disease. In this chapter, only a subset of these topics will be considered.
The degree of ptosis can be quantified clinically by measuring the height of the palpebral fissure—about 9 mm in normal subjects—assuming the lower eyelid is normally positioned. A more useful measure is the distance between the upper lid margin and the midcorneal reflex when the globe is in primary position. This is called the MRD-1. Ptosis can be defined as an MRD-1 less than 2 mm or an asymmetry of more than 2 mm between eyes. Using this definition, most patients with ptosis exhibit a contraction of the superior visual field to 30 degrees or less.
Neurogenic Ptosis
Neurogenic ptosis may be caused by supranuclear, nuclear, or infranuclear dysfunction. In some cases, associated symptoms and signs make the distinctions among these causes obvious; in other cases, however, neither the location nor the nature of the lesion is clear.
Supranuclear Ptosis
Unilateral ptosis is a rare manifestation of hemisphere dysfunction. This manifestation, called cortical ptosis, usually, although not invariably, is contralateral to the lesion. Unilateral ptosis has been described contralateral to lesions of the angular gyrus, to seizure foci in the temporal lobe, to hemispheric stroke, and to frontal lobe arteriovenous malformations (AVMs). It also has been described ipsilateral to ischemic hemispheric strokes (Fig. 22.4).
 Figure 22.4 Unilateral supranuclear (cortical) ptosis. The patient developed a left ptosis associated with a left hemiparesis from a right hemisphere stroke. The patient also has a pre-existing right ptosis from dehiscence of the levator tendon. (Reprinted with permission from Caplan LR. Cerebral ptosis. J NeurolNeurosurg Psychiatry. 1974;37:1–7.) |
Bilateral cortical ptosis can also occur. It is associated most frequently with extensive nondominant hemisphere lesions. In most instances, the ptosis is accompanied by midline shift, gaze deviation to the right, and other signs of right hemisphere dysfunction, including left hemiparesis. The ptosis is often asymmetric. In the setting of cerebral infarction, the ptosis is transient, lasting from several days to 5 months or more.
Ptosis may develop in certain eccentric positions of gaze from congenital supranuclear inhibition of the levator; that is, supranuclear oculopalpebral synkinesia. In such cases, lid position in primary gaze may be normal, or the lid may be slightly ptotic. When the patient adducts (or occasionally abducts) the eye on the affected
side, however, the eyelid drops abruptly because of a loss of levator muscle tone. When the eye returns toward center, or toward the opposite side, the levator contracts and the eyelid returns to a normal position. The synkinesia may be unilateral (Fig. 22.5) or bilateral (Fig. 22.6). It may occur as an isolated phenomenon or in association with other congenital syndromes, such as the Duane retraction syndrome. The causes of supranuclear paradoxical levator inhibition are unclear. They may involve a variety of mechanisms, including ephaptic transmission or disturbances in the supranuclear pathways responsible for levator tonus, excitation, and inhibition.
side, however, the eyelid drops abruptly because of a loss of levator muscle tone. When the eye returns toward center, or toward the opposite side, the levator contracts and the eyelid returns to a normal position. The synkinesia may be unilateral (Fig. 22.5) or bilateral (Fig. 22.6). It may occur as an isolated phenomenon or in association with other congenital syndromes, such as the Duane retraction syndrome. The causes of supranuclear paradoxical levator inhibition are unclear. They may involve a variety of mechanisms, including ephaptic transmission or disturbances in the supranuclear pathways responsible for levator tonus, excitation, and inhibition.
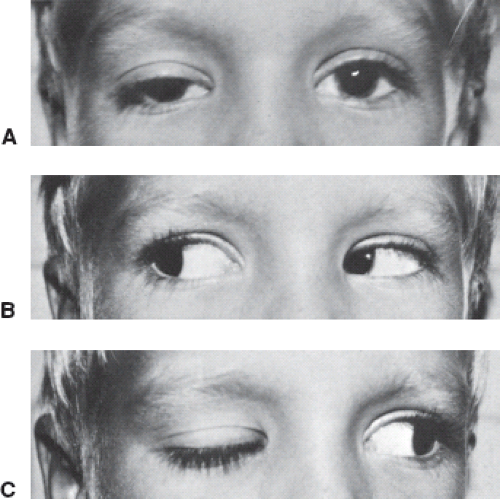 Figure 22.5 Congenital unilateral supranuclear oculopalpebral synkinesia. A: This young child has moderate right ptosis when looking straight ahead. B: When the patient looks to the right, the position of both upper eyelids is normal. C: On left gaze, there is almost complete right ptosis from inhibition of the levator muscle. Note that the left upper eyelid remains in a normal position in all positions of gaze. (Courtesy of Dr. C. Hedges.) |
Ptosis associated with mouth opening—the inverse Marcus Gunn phenomenon—is a rare condition in which the ipsilateral eyelid closes when the external pterygoid muscle moves the jaw to the opposite side (Fig. 22.7). Patients with this condition have mild ptosis of the affected eyelid when the eyes are in primary position and the mouth is closed. The associated ptosis is consequent to levator inhibition without contraction of the orbicularis oculi. This syndrome is an inverse of the Marcus Gunn jaw-winking phenomenon (see below) and probably represents a supranuclear synkinesis affecting the oculomotor and trigeminal nerves.
 Figure 22.6 Congenital bilateral supranuclear oculopalpebral synkinesia. Center: In primary position, the patient has a moderate right ptosis. On right gaze (right), the patient develops a marked left ptosis, whereas on left gaze (left), the patient develops a marked right ptosis. (Courtesy of Dr. H. Rose.) |
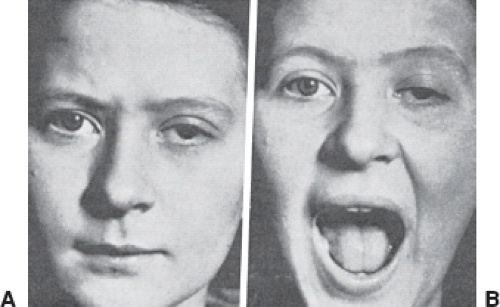 Figure 22.7 The inverse Marcus Gunn phenomenon. A: When the patient looks straight ahead, she has a mild left ptosis. B: When the patient opens her mouth, the ptosis increases from inhibition of the left levator muscle. |
Ptosis from Lesions of the Oculomotor Nucleus, Fascicle, or Nerve
By far, the most common causes of acquired neurogenic ptosis are related to dysfunction of the oculomotor nucleus, fascicle, or nerve. Because the central caudal subnucleus of the oculomotor nucleus supplies bilateral equal innervation to the levator muscles, ptosis resulting from a nuclear midbrain lesion is always bilateral and symmetric as well as usually complete or at least very severe (Fig. 22.8). This midbrain ptosis is commonly associated with other signs of mesencephalic dysfunction. However, in some cases, only the central caudal subnucleus of the oculomotor nuclear complex is affected or is much more severely affected than the other oculomotor subnuclei, and bilateral, severe, symmetric ptosis is the predominant or only manifestation of the nuclear lesion.
Midbrain ptosis may be congenital, occurring as a consequence of dysplasia or aplasia of the oculomotor nucleus, or acquired. Acquired causes include ischemia, inflammation, infiltration, compression, and metabolic and toxic processes.
Lesions of the fascicle of the oculomotor nerve produce unilateral oculomotor nerve dysfunction that may be mild or severe (see Chapter 18). When ptosis occurs in patients with a lesion of the oculomotor fascicle, it is always unilateral, of variable severity, and,
in our experience, associated with weakness of one or more of the extraocular muscles innervated by the oculomotor nerve (Fig. 22.9). Pupillary involvement is commonly but not invariably present.
in our experience, associated with weakness of one or more of the extraocular muscles innervated by the oculomotor nerve (Fig. 22.9). Pupillary involvement is commonly but not invariably present.
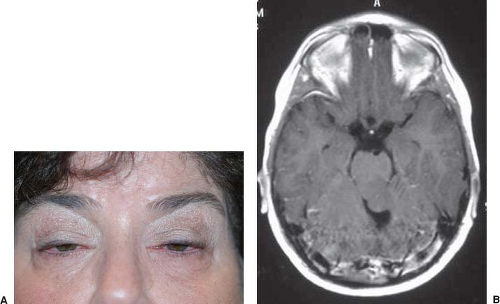 Figure 22.8 Midbrain ptosis. Isolated, bilateral ptosis in a patient with a mass lesion infiltrating the posterior and caudal midbrain. A: Severe bilateral ptosis. B: T1-weighted axial MRI with gadolinium shows a nonenhancing lesion involving the central aspect of midbrain. Ocular motility was completely normal. |
The ptosis that accompanies a lesion of the peripheral oculomotor nerve is, like that caused by a fascicular lesion, unilateral and usually accompanied by ophthalmoparesis, pupillary involvement, or both (Fig. 22.10). Rarely, however, ptosis precedes the other signs of oculomotor nerve dysfunction by days, weeks, or even months, depending on the location and nature of the lesion. Isolated ptosis caused by peripheral oculomotor nerve dysfunction has been reported in patients with aneurysms, pituitary adenomas, meningiomas, and meningitis. Some of these cases are examples of truly isolated ptosis. In others, there are other symptoms, for example, headache, or subtle signs of oculomotor dysfunction, a mildly dilated but reactive pupil, an incomitant phoria, or asymptomatic underaction of the superior rectus that is only evident on extreme upgaze. Recurrent, isolated ptosis lasting 6 to 8 weeks has been described with ophthalmoplegic migraine. Isolated, complete, neurogenic ptosis can also occur from orbital trauma that generates forceful anterior displacement of the upper eyelid with denervation of the levator muscle. This form of ptosis usually resolves spontaneously within weeks.
Ptosis from Lesions of the Oculosympathetic Pathways
Lesions of the oculosympathetic pathway produce Horner syndrome, a condition that is characterized in part by a partial, unilateral ptosis from hypofunction of Müller muscle. The ptosis of Horner syndrome is often mild, variable, and always associated with ipsilateral miosis (Fig. 22.11), in contrast to the more severe ptosis with mydriasis in an oculomotor nerve lesion. Horner syndrome is discussed in detail in Chapter 15 of this text.
The ptosis occasionally observed after conjunctival instillation of timolol maleate, a β-adrenergic–blocking agent, may be caused by Müller muscle blockade. Similarly, thymoxamine, an α-adrenergic–blocking agent, may cause ptosis when given topically or parenterally.
Myopathic Ptosis
Ptosis that occurs from damage to the levator palpebrae superioris muscle itself (as opposed to its tendon) may be either congenital (i.e., developmental) or acquired; the latter is discussed below.
Acquired Myopathic Ptosis
Acquired myopathic ptosis occurs in a number of the mitochondrial cytopathies characterized by chronic progressive external ophthalmoplegia (CPEO) (see Chapter 20). In some
patients, the ptosis is the presenting sign and may persist in isolation for months to years before the development of ophthalmoplegia. Ptosis of this type usually is bilateral, relatively symmetric, and very slowly progressive. The superior palpebral lid fold may be completely absent. Excessive wrinkling of the brow and backward head tilting are commonly employed to facilitate vision beneath the drooping lids (Fig. 22.12). Orbicularis oculi function, tested by forced lid closure, is frequently weak, and this combination of weakness of both eyelid opening and eyelid closure serves to distinguish the condition from other causes of ptosis except myasthenia gravis and myotonic dystrophy.
patients, the ptosis is the presenting sign and may persist in isolation for months to years before the development of ophthalmoplegia. Ptosis of this type usually is bilateral, relatively symmetric, and very slowly progressive. The superior palpebral lid fold may be completely absent. Excessive wrinkling of the brow and backward head tilting are commonly employed to facilitate vision beneath the drooping lids (Fig. 22.12). Orbicularis oculi function, tested by forced lid closure, is frequently weak, and this combination of weakness of both eyelid opening and eyelid closure serves to distinguish the condition from other causes of ptosis except myasthenia gravis and myotonic dystrophy.
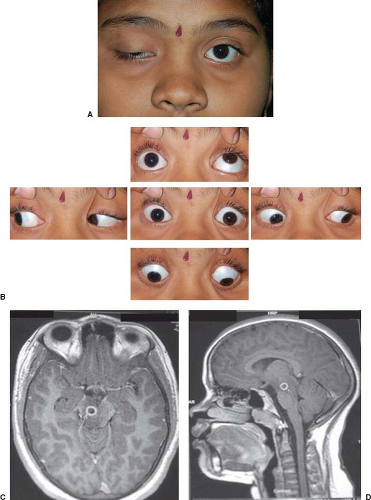 Figure 22.9 Unilateral ptosis associated with other evidence of a right third nerve paresis caused by damage to the fascicle of the third nerve from a cryptococcal abscess. A and B: Appearance of patient; (C) axial and (D) sagittal MRI showing a ring-enhancing lesion along the path of the right oculomotor nerve fascicle (arrows). |
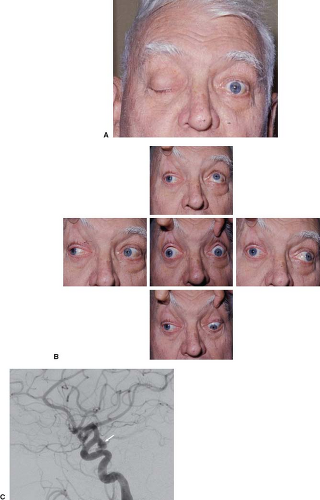 Figure 22.10 Unilateral ptosis associated with other evidence of a right third nerve paresis caused by damage to the subarachnoid portion of the third nerve from an intracranial aneurysm. A: Appearance of patient; in primary gaze and (B) in different gaze positions. C: Angiogram in a different patient showing aneurysm (arrow) at the junction of the left internal carotid artery and left posterior communicating artery. |
 Figure 22.11 Horner syndrome. Note mild unilateral ptosis, anisocoria with smaller pupil on side of ptosis, and redness from associated cluster headache. The usual “upside-down” ptosis (i.e., elevation) of the lower lid is masked by coexisting eyelid laxity and blepharitis, which can be confounding factors in older adults. |
 Figure 22.12 Ptosis in a patient with CPEO. Note also flat, expressionless facial features associated with continuous frontalis effort to lift the brows. (Pupil dilation is pharmacologic.) |
Because the manifestations of the disease are so slowly progressive and in part because they tend to be symmetric, patients with ptosis associated with CPEO are remarkably tolerant of their symptoms, and thus generally present relatively late in their course.
Bilateral partial ptosis contributes to the characteristic appearance of patients with myotonic dystrophy.
The levator palpebrae superioris muscle may be damaged by a variety of inflammatory, ischemic, or infiltrative processes affecting the orbit. Occasionally, ptosis is the most prominent manifestation. For example, lymphoid infiltration, sarcoidosis, amyloidosis, and idiopathic inflammatory disease of the orbit can sometimes selectively affect the levator and spare the extraocular muscles. Patients with diabetes mellitus also may develop unilateral or bilateral ptosis in association with other evidence of microangiopathic changes elsewhere in the body. Although most of these patients probably have a localized infarction in the midbrain, which affects either the oculomotor nerve nucleus or fascicle, or in the peripheral oculomotor nerve, chronic hypoxia of the levator muscle is responsible for this form of ptosis in some diabetic patients.
Neuromuscular Ptosis
Recognition of neuromuscular ptosis depends in part on the absence of clinical signs of an oculomotor or sympathetic lesion and the presence of clinical signs of neuromuscular disease. Ptosis in myasthenia gravis may occur in isolation, but it is more often associated with diplopia, varying degrees of ophthalmoparesis, weakness of the orbicularis oculi, and normal pupillary function by clinical testing (see Chapter 19). Ultimately, ptosis occurs in the majority of patients with myasthenia gravis. Regardless of when it develops, the ptosis of myasthenia gravis may be unilateral or bilateral, and when it is bilateral, it may also be symmetric or asymmetric (Fig. 22.13).
The hallmark of myasthenic ptosis is its fatigability and tendency to fluctuate in severity, although this feature is by no means pathognomonic. A similar tendency to fatigue (although not to the same degree) occurs in patients with aponeurotic defects and oculomotor nerve palsies. Patients with ptosis from myasthenia gravis, myasthenic syndromes, botulism, or drugs affecting neuromuscular transmission usually have sufficient signs and symptoms to allow the correct diagnosis to be made, such as the Cogan lid-twitch sign (Video 22.1), enhancement of ptosis with manual elevation of the contralateral eyelid (Video 22.2), and the orbicularis “peek” sign (Fig. 22.14). In addition, unless it is complete, myasthenic ptosis often improves when ice is held to the affected eyelid for 2 minutes (Fig. 22.15; see Chapter 19).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


