Operative Considerations and Techniques for Partial Glossectomy
Kwang Hyun Kim
INTRODUCTION
Cancer of the oral cavity is the sixth most common cancer worldwide. Cancer of the tongue represents 2% of the annual cancer incidence in the United States with a male preponderance of 2:1. The prevalence of cancer of the tongue is much higher in certain Asian countries, especially where betel nut chewing is popular. However, the incidence of cancer of the tongue is also high in Eastern Europe and France, where smoking and alcohol intake are higher than in other countries. Despite the high incidence of cancer of the oral tongue, treatment outcome has hardly changed over the last few decades.
Histopathologically, squamous cell carcinoma is the most common form, which is further divided into three types: exophytic, ulcerative, and infiltrative. Cancer of the tongue is usually well differentiated. Small cancers of <1 cm may go undetected until the patient becomes symptomatic, or the cancer is detected by chance such as when a physical examination is done for other reasons. However, because the mobile tongue is readily visible and is relatively accessible, there is a good chance of detecting early lesions. Cancer of the tongue is usually found in the mobile tongue, most commonly on the lateral border. Approximately 75% of the cancers are located in the posterolateral aspect of the oral tongue, 20% in the anterolateral and ventral surface, and 3-5% on the dorsum. The lingual and hypoglossal nerves may be invaded directly by tumors, which may cause loss of sensation and deviation on tongue protrusion. Advanced cancer of the tongue is also associated with induration and ulceration of the tongue.
Surgery is still the mainstay of treatment for cancer of the oral tongue, especially in early cases. Partial glossectomy (PG) suffices in most cases of early cancers, especially those on the lateral aspect of the tongue. Minimal morbidity and good functional outcome are a big advantage of PG.
Relevant Anatomy
The root of the tongue rests on the floor of mouth (FOM) and is attached by muscles to the hyoid bone, mandible, styloid processes, and pharynx. The anterior and posterior limits of the mobile tongue are the lingual frenulum and the circumvallate papillae (sulcus terminalis). The oral tongue is a freely mobile portion of the tongue, which is also referred to as the mobile tongue. By definition, the muscular tissue posterior to the circumvallate papillae is the base of the tongue (BOT), which is a part of the oropharynx, although this boundary does not act as a barrier of tumor growth. The oral tongue is covered by stratified keratinizing squamous epithelium. Various taste buds cover the surface, including the filiform, fungiform, and circumvallate papillae (Fig. 4.1).
The surface topography of the mobile tongue reveals four anatomic regions: the tip, the lateral borders, the dorsum, and the undersurface or ventral surface (nonvillous surface). The tongue musculature is composed of three intrinsic muscles and three extrinsic muscles. The extrinsic muscles include the genioglossus, the hyoglossus, and the styloglossus muscles. The intrinsic muscles are composed of three groups of fibers
running in different directions, which are the superior/inferior longitudinal, vertical, and transverse muscles. The trilaminar group of intrinsic muscles is not attached to the bone. These six muscles together allow the mobile tongue to change shape and consistency, which enables various functions of the tongue such as speech and deglutition (Fig. 4.2).
running in different directions, which are the superior/inferior longitudinal, vertical, and transverse muscles. The trilaminar group of intrinsic muscles is not attached to the bone. These six muscles together allow the mobile tongue to change shape and consistency, which enables various functions of the tongue such as speech and deglutition (Fig. 4.2).
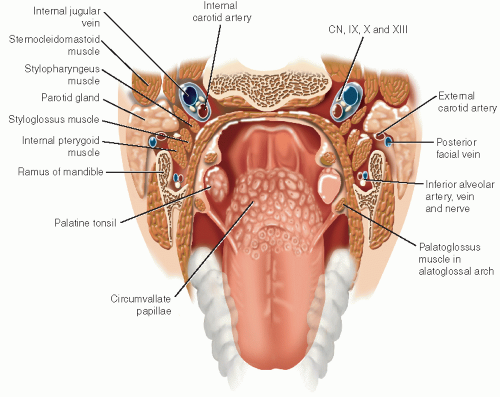 FIGURE 4.1 Tongue and its surrounding structures. |
The major blood supply of the tongue is the lingual artery, which is a direct branch of the external carotid artery. The lingual artery bifurcates at the level of the hyoid bone and courses anteriorly to reach deep into the hyoglossus muscle. The artery then branches off small tributaries in the ipsilateral tongue, which do not cross the midline. The artery travels further into the tongue toward the tip. Only then the arteries create an anastomosis with the branches from the contralateral side. The primary vein is the lingual vein, which flows into the internal jugular vein.
The main motor innervation of the tongue is supplied by the hypoglossal (CN XII) nerve. From posterior to anterior, the nerve courses between the hyoglossus muscle and the submandibular gland. Nerve fibers spread out to innervate the extrinsic muscles and are connected to the intrinsic muscles at its terminus. The lingual branch of the mandibular nerve (CN V3) delivers general sensation. Taste, from the taste buds, is conveyed by the chorda tympani nerve, which is joined by the lingual nerve and confluences into the facial nerve (CN VII) (Fig. 4.3).
The rich lymphatics in the tongue form the submucosal lymphatic plexus. Whereas the blood vessels cross the midline only at the tip, the lymphatics communicate freely from both sides which provide a route for cancer to spread in all directions. Lymphatics in the tip of the tongue drain into the submental lymph nodes. The dorsum and lateral tongue lymphatics flow into the ipsilateral submandibular nodes. Hence, these two lymph node groups form the first echelons of the lymphatic drainage of the mobile tongue. The lymphatic flow eventually drains into the deep jugular lymph nodes located between the digastric and the omohyoid muscles.
HISTORY
Detailed history taking is an essential initial step for the approach to the patient. Smoking habit and alcohol intake are essential part of the history. Functional status of the patient regarding the cancer should also be noted. Depending on the location of the cancer, the patient may have dysphagia, odynophagia, and dysarthria.
Pain may be a sign of nerve involvement. History of a mass in the neck should be sought. The general condition of the patient, including weight loss and decreased appetite, should also be noted. Recent and remote dental treatment history should also be sought. Family history should not be omitted.
Pain may be a sign of nerve involvement. History of a mass in the neck should be sought. The general condition of the patient, including weight loss and decreased appetite, should also be noted. Recent and remote dental treatment history should also be sought. Family history should not be omitted.
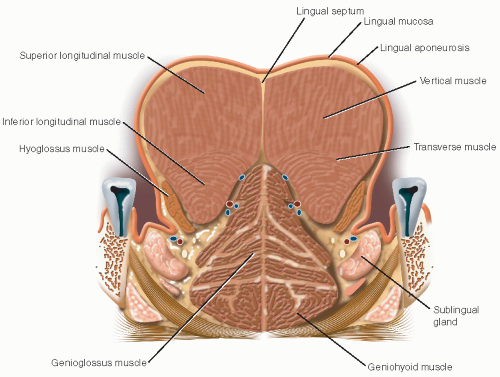 FIGURE 4.2 Coronal section through the tongue showing the intrinsic and extrinsic musculature. |
 FIGURE 4.3 Vessel and nerve supply to the tongue. |
PHYSICAL EXAMINATION
Complete examination of the head and neck must be performed. This includes thorough inspection of the upper aerodigestive tract comprising the oral cavity, the pharynx, and the larynx using office endoscopy and laryngoscopy. The possibility of a second primary cancer should not be neglected even in early cancers. Panendoscopy (direct laryngoscopy and esophagoscopy) may be performed. However, it is not routinely performed as the benefit of a separate general anesthesia is not well established in early cancers of the mobile tongue. Examination of the neck for cervical lymphadenopathy is also mandatory. It is reported that 30% to 40% of patients with cancer of the oral tongue demonstrate evidence of cervical metastasis at initial presentation. Additional care should be taken when palpating the ipsilateral levels I-III as the sentinel nodes are usually located in this area.
It is advisable that examination of the teeth also be performed. In a significant number of patients, dental conditions require extraction of the teeth. This is especially important when postoperative radiotherapy is anticipated. If needed, thorough dental examination and/or tooth extraction may be performed by a dentist prior to surgery. However, for many patients, tooth extraction may be performed during the general anesthesia by the oral surgeons just prior to the main surgical procedure.
INDICATIONS
Early cancer of the mobile tongue is the primary indication for PG (T1, T2). Carcinoma in situ and leukoplakia with heterogeneous features are less common indications. Early T3 lesions may be an indication for PG, when the cancer is situated anteriorly and laterally. Patients with lesions in the lateral tongue are good candidates for PG.
CONTRAINDICATIONS
PG may not be suitable for advanced T3, T4 primary cancer of the tongue. Although it may be applicable, the morbidity and resulting functional deficit may not be acceptable. There also is a concern for oncologic safety regarding obtaining adequate surgical margins and excessive manipulation of a large volume cancer. Cancer invading into adjacent structures is also a contraindication. Location of the cancer where obtaining adequate margins is expected to be difficult is also a contraindication for PG. Cancers located in the posterior aspect of the mobile tongue adjacent to the BOT are especially difficult to completely excise by PG, which makes it a contraindication for this procedure.
Cancer crossing the midline of the tongue also precludes a PG. Because PG requires preservation of one lingual artery and one hypoglossal nerve, tumor infiltration beyond the midline with proximity to the contralateral neurovascular bundle is a contraindication for PG.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


