Opacification of the Ocular Media
Mohammad Ali Javadi
Hamid Ahmadieh
Sepehr Feizi
Media opacification after cataract surgery is more common in children than in adults. It interferes with the main goals of the operation and is a potential cause of amblyopia. Media opacification may develop rapidly or insidiously. Examples of sudden-onset media opacification include corneal edema, inflammatory pupillary membrane, and vitreous hemorrhage; these events are usually identified promptly, sometimes by the parents or caretaker, and usually resolve with appropriate treatment and with time. In contrast, some types of media opacity are delayed and tend to be progressive, including cellular, fibrinous, or pigmentary deposits on the intraocular lens (IOL) and posterior capsule opacification (PCO) or hyaloid face opacification. Since children may be unable to report decreased vision, these may go unnoticed and lead to irreversible visual damage.
Posterior capsular opacification remains the most common complication of pediatric cataract surgery1,2,3 (Fig. 50.1). PCO can be treated using Nd:YAG laser capsulotomy or surgical posterior capsulectomy. Nd:YAG laser technique involves clearing the visual axis by creating a central opening in the opacified posterior capsule.1,4 Although this procedure is easy and quick, there are complications, including retinal detachment, damage to the IOL, cystoid macular edema (CME), an increase in intraocular pressure (IOP), iris hemorrhage, corneal edema, IOL subluxation, and exacerbation of localized endophthalmitis.1,4,5
Posterior capsular opacification is more threatening in young adults and children, with a higher incidence, quicker onset, and greater amblyogenic effect. Additionally, PCO in young children is often dense (see Fig. 50.1) and may need to be removed with additional surgery, which carries more risks of potential complications.6,7 This chapter focuses on PCO and its incidence, predisposing factors including patient characteristics, IOL features, surgical techniques, preventive measures such as primary posterior capsulectomy accompanied by anterior vitrectomy, and intraoperative cytotoxic agents. Additionally, other less common causes of media opacification are reviewed.
POSTERIOR CAPSULE OPACIFICATION
Until the late 1960s, the preferred method of pediatric cataract surgery was lens aspiration, leaving the posterior capsule intact as popularized by Scheie.8 With this method, remaining lens epithelial cells (LECs) proliferate and migrate on the intact posterior capsule, leading to opacification of the once-clear capsule. In some cases, the ensuing opacity causes more visual deterioration than the original cataract itself.9 After the advent of automated posterior capsulectomy and vitrectomy in 1976, pediatric cataract surgeons began to perform lensectomy with anterior vitrectomy through a large opening in the posterior capsule, leaving only a 1- to 2-mm rim behind.10 This new trend quickly caught on and was used by the majority of pediatric cataract surgeons by the mid-1980s. It resulted in superior media clarity.10 Further refinements of surgical technique, improved IOL quality, and favorable results of IOL implantation in adults started a trend toward IOL implantation in children in the early 1990s. However, opacification of the retained lens capsule still led to poor vision and amblyopia.10,11 The secondary opacification and fibrosis may be severe enough to cause IOL decentration and even break the optic-haptic junction.12 Even in the era of modern cataract surgery, PCO still poses a challenge for ophthalmologists.13,14,15
Mechanism of PCO Development
LECs left behind in the capsular bag after any type of extracapsular cataract surgery are mainly responsible for PCO development.9 Proliferation, migration, epithelial-to-mesenchymal transition (EMT), collagen deposition, and lens fiber regeneration of LECs are the main causes of opacification. It appears that cataract surgery induces a wound healing response in the lens, and retained LECs proliferate and migrate across the posterior capsule and undergo lens fiber regeneration and EMT.16,17,18 In vitro studies and animal models of PCO suggest that several cytokines and growth factors play a major role in the pathogenesis of PCO.19,20 Studies show that levels of
several cytokines and growth factors increase in aqueous humor and influence the behavior of the remaining LECs after cataract surgery. These factors include transforming growth factor β (TGF-β), fibroblast growth factor 2 (FGF-2), hepatocyte growth factor, interleukins 1 and 6 (IL-1 and IL-6), and epithelial growth factor.19,21 TGF-β plays a central role in the cell biology of PCO. Clinically, there are two morphologic types of PCO, the fibrosis type and the pearl type. Fibrosis-type PCO is caused by the proliferation and migration of LECs, which undergo EMT, resulting in fibrous metaplasia and leading to significant visual loss by producing folds and wrinkles in the posterior capsule.16 Pearl-type PCO is caused by the LECs located at the equatorial lens region (lens bow) causing regeneration of crystallin-expressing lenticular fibers and forming Elschnig pearls and Soemmering ring, responsible for most cases of PCO-related visual loss.2,22
several cytokines and growth factors increase in aqueous humor and influence the behavior of the remaining LECs after cataract surgery. These factors include transforming growth factor β (TGF-β), fibroblast growth factor 2 (FGF-2), hepatocyte growth factor, interleukins 1 and 6 (IL-1 and IL-6), and epithelial growth factor.19,21 TGF-β plays a central role in the cell biology of PCO. Clinically, there are two morphologic types of PCO, the fibrosis type and the pearl type. Fibrosis-type PCO is caused by the proliferation and migration of LECs, which undergo EMT, resulting in fibrous metaplasia and leading to significant visual loss by producing folds and wrinkles in the posterior capsule.16 Pearl-type PCO is caused by the LECs located at the equatorial lens region (lens bow) causing regeneration of crystallin-expressing lenticular fibers and forming Elschnig pearls and Soemmering ring, responsible for most cases of PCO-related visual loss.2,22
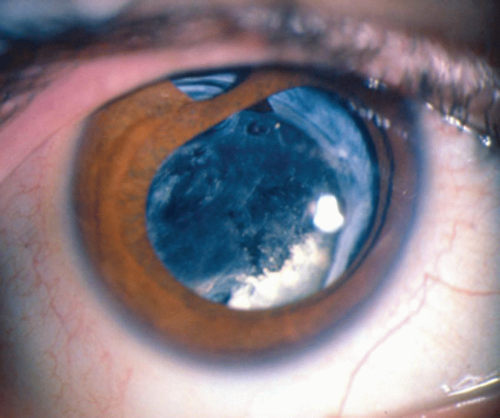 Figure 50.1. A dense posterior capsular opacification develops after lensectomy without posterior capsulectomy for congenital cataract. |
Incidence and Impact of PCO
PCO has been reported in 39% to 100% of pediatric cases in which the capsule is left intact.7,9,13,14,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46 Taylor47 reported 32 reoperations for capsular opacity in 28 pediatric eyes with an intact posterior capsule following lens aspiration. The incidence of PCO depends on the age at surgery, the type of cataract (congenital, developmental, or traumatic), aphakia versus pseudophakia, ciliary sulcus versus capsular bag fixation, associated ocular abnormalities (e.g., persistent fetal vasculature [PFV], microcornea), and preexisting systemic conditions such as juvenile rheumatoid arthritis. Additionally, the duration of follow-up affects the incidence of PCO; the longer the follow-up, the more PCO is manifested.
The burden of PCO is reflected in numerous reports. Basti et al.43 reported the mean time for PCO appearance to be 3 months after surgery. Jensen et al.37 observed significant PCO 1 to 26 months after cataract surgery in children with a mean age of 7.3 years. The peak incidence of PCO was 18 months after surgery; thereafter, the curve flattened considerably. PCO was more common in younger children: 64% of children 1 to 6 years old versus of those 6 to 13 years old developed PCO.37 Gimbel et al.42 reported a cumulative rate for Nd:YAG laser capsulotomy of 17%, 42%, 52%, and 59% at 1, 2, 3, and 4 years after surgery, respectively. Plager et al.14 observed a mean duration of 2 years for PCO development. Plager et al.14 reported PCO in 90% of 71 eyes with a retained posterior capsule by 3.5 years in children 10 months to 17 years of age. According to Crouch et al.,29 PCO developed in 72% of 35 eyes of children 5 to 18 years of age undergoing cataract surgery and IOL implantation with retention of the posterior capsule. Müllner-Eidenböck et al.48 observed PCO in 9 out of 15 eyes (60%) of children 6 to 16 years of age with an intact posterior capsule and acrylic IOL implant. Hosal and Biglan36 observed secondary capsular membranes in 78.6% of operated eyes 3 weeks to 53 months after surgery; they reported a 10.7-fold risk of media opacity with posterior capsule retention. In the same study, eyes with a primary posterior capsulectomy but no vitrectomy developed secondary media opacity 42.9% of the time compared to 22.5% when both a posterior capsulectomy and an anterior vitrectomy were done at the time of the cataract aspiration. Age <1 year at surgery was also an independent risk factor with a 4.7-fold added risk of secondary media opacity.
Recent modifications in IOL design (i.e., square edge profile) and improved biocompatibility (e.g., acrylic) have significantly reduced the incidence of PCO in adults; however, there are insufficient data to know whether these new lenses result in a commensurate reduction in children.48,49 Therefore, current options for prevention of PCO include primary posterior capsulectomy (with or without vitrectomy) or postoperative Nd:YAG laser disruption of the posterior capsule before opacification.50 Disadvantages of the latter method include the lack of sufficient cooperation by children and possible need for a second anesthesia, need for a special Nd:YAG laser capable of functioning with the patient in the supine position, risk of IOL damage, and, above all, risk of recurrent media opacity on the anterior vitreous or hyaloid face. A limitation of the Nd:YAG laser capsulotomy is that it does not address the problem of the residual intact anterior vitreous face that provides a scaffold on which residual lens fibers grow to create secondary opaque membranes. The anterior hyaloid face not only serves as a scaffold for migration and metaplasia of LECs but also acts as a surface for deposition of inflammatory cells, debris, and pigment.51 This procedure is not advisable in very young children. Atkinson and Hiles7 reported on 32 eyes of 28 children undergoing cataract surgery with or
without IOL implantation who received postoperative Nd:YAG laser capsulotomy with the Microruptor III, which is capable of rotating 90 degrees. In 16 eyes in which laser capsulotomy was performed earlier than 4 weeks, the mean energy required was 114 mJ; however, in the remaining eyes, the procedure was performed later than 4 weeks, and the mean energy required was 324 mJ. Overall, the rate of membrane reformation was 25% in this series. Hutcheson et al.38 compared the incidence of media opacity between pediatric cataract extractions with primary posterior capsulectomy (33 eyes) and those with postoperative laser disruption (23 eyes); 3% versus 57% of the eyes, respectively, developed media opacity needing further treatment. Furthermore, in the second group, 17% required repeat laser treatment after the second laser session. Koch and Kohnen52 noted that all 5 eyes with intact posterior capsules required Nd:YAG laser capsulotomies within 18 months of the initial surgery and 3 eyes required a second laser treatment within 9 months of the first one. In a study of PCO rates after foldable acrylic IOL implantation, Müllner-Eidenböck et al.48 observed that 60% of the eyes belonging to the younger age group (<4 years) developed recurrent opacification following Nd:YAG laser treatment. Based on this observation, the authors concluded that surgical capsulectomy combined with anterior vitrectomy rather than Nd:YAG laser capsulotomy may be needed in young children to maintain a clear visual axis. Laser capsulotomy is often ineffective in the presence of fibrous PCO. When a dense retrolental membrane develops, a more invasive approach, using the vitrectomy handpiece, is required.
without IOL implantation who received postoperative Nd:YAG laser capsulotomy with the Microruptor III, which is capable of rotating 90 degrees. In 16 eyes in which laser capsulotomy was performed earlier than 4 weeks, the mean energy required was 114 mJ; however, in the remaining eyes, the procedure was performed later than 4 weeks, and the mean energy required was 324 mJ. Overall, the rate of membrane reformation was 25% in this series. Hutcheson et al.38 compared the incidence of media opacity between pediatric cataract extractions with primary posterior capsulectomy (33 eyes) and those with postoperative laser disruption (23 eyes); 3% versus 57% of the eyes, respectively, developed media opacity needing further treatment. Furthermore, in the second group, 17% required repeat laser treatment after the second laser session. Koch and Kohnen52 noted that all 5 eyes with intact posterior capsules required Nd:YAG laser capsulotomies within 18 months of the initial surgery and 3 eyes required a second laser treatment within 9 months of the first one. In a study of PCO rates after foldable acrylic IOL implantation, Müllner-Eidenböck et al.48 observed that 60% of the eyes belonging to the younger age group (<4 years) developed recurrent opacification following Nd:YAG laser treatment. Based on this observation, the authors concluded that surgical capsulectomy combined with anterior vitrectomy rather than Nd:YAG laser capsulotomy may be needed in young children to maintain a clear visual axis. Laser capsulotomy is often ineffective in the presence of fibrous PCO. When a dense retrolental membrane develops, a more invasive approach, using the vitrectomy handpiece, is required.
Primary posterior capsulectomy with or without anterior vitrectomy decreases the chance for PCO, and it is believed to be safe (Fig. 50.2). Dahan and Salmenson53 suggested removal of the center of the posterior capsule with a vitrector in association with IOL implantation. Buckley et al.54 observed no media opacity by 13 months in 20 eyes undergoing IOL implantation followed by primary posterior capsulectomy and anterior vitrectomy through a pars plana approach. Luo et al.55 observed that the rate of fibrous exudates in the anterior chamber and the rate of IOL subluxation or capture were significantly lower when posterior continuous curvilinear capsulorhexis (PCCC) and anterior vitrectomy were performed in children aged between 2 and 5 years. They concluded that primary PCCC with anterior vitrectomy is an effective procedure with a low PCO rate in pediatric cataract. However, opponents of this approach believe that retention of the posterior capsule without concomitant vitrectomy may decrease the risk of CME, retinal detachment, and vitreous incarceration into the surgical wound, facilitate in-the-bag IOL implantation, and provide long-term IOL stability.50
Opinions differ regarding the effect of primary posterior capsulectomy on CME. Hoyt and Nickel56 operated on 27 children with bilateral cataracts: one eye of each patient underwent lensectomy and vitrectomy; the fellow eye was treated with lens aspiration and discission of the posterior capsule. In the first group, 10 eyes developed CME, while no instances were noted in the fellow eyes. On the other hand, other investigators have reported different results. Gilbard et al.57 reported only one case of suspected CME on angiographic and angioscopic examination of 25 eyes of 17 patients undergoing lensectomy and anterior vitrectomy. Green et al.58 observed no cases of CME in 52 eyes undergoing pars plicata lensectomy and vitrectomy. In a series of 24 children undergoing bilateral cataract surgery and IOL implantation, Gimbel et al.46 reported only one case of bilateral CME in a patient with retinitis pigmentosa. Pinchoff et al.59 reported on lensectomy and vitrectomy (12 eyes), extracapsular cataract extraction and discission (5 eyes), extracapsular cataract extraction (3 eyes), and secondary discission (3 eyes); in none of the eyes, CME was detectable by angiography. Ahmadieh et al.60 also reported no case of CME on the angioscopic examination of 38 eyes undergoing limbal or pars plana lensectomy, anterior vitrectomy, and posterior chamber IOL implantation. It is generally difficult to diagnose and document CME in children as it is a rare event. Even more notable is the low retinal detachment rate after this procedure.56 This can be partly attributed to the presence of a well-formed vitreous in the child’s eye.
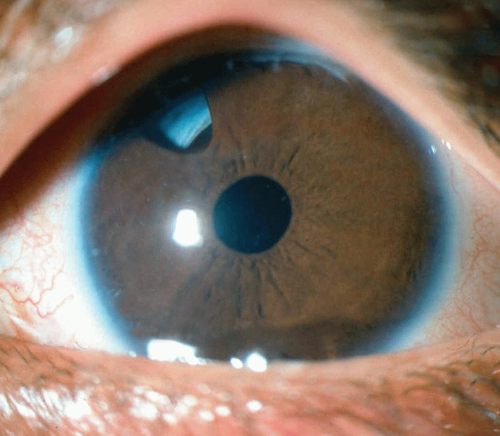 Figure 50.2. A clear media after lensectomy, primary posterior capsulectomy, vitrectomy, and in-the-bag IOL implantation. |
Overall, current evidence supports the idea that primary posterior capsulectomy is a safe procedure in children and is effective in the prevention of media opacity. Primary posterior capsulectomy may be performed with a vitrectomy probe via the limbus, pars plicata, or pars plana; another method is to perform a PCCC with
forceps. Following posterior capsulectomy, the posterior chamber IOL may be implanted into the capsular bag or ciliary sulcus. In either case, capture of the optic into the posterior capsular opening may be performed in hopes of providing better lens centration or further reduction of the risk of media opacity.
forceps. Following posterior capsulectomy, the posterior chamber IOL may be implanted into the capsular bag or ciliary sulcus. In either case, capture of the optic into the posterior capsular opening may be performed in hopes of providing better lens centration or further reduction of the risk of media opacity.
Despite removal of the posterior capsule, numerous studies have shown that secondary membranes and media opacity can still develop.9,15,25,27,28,30,32,40,41,49,58,61,62 An intact hyaloid face can serve as a scaffold for migration of LECs and their subsequent proliferation and transformation.30,49,62,63 This phenomenon is further enhanced in children by the more intense inflammatory response following surgery.64 O’Keefe et al.25 reported media opacity in 33.3% of cases following primary posterior capsulectomy when anterior vitrectomy was not performed. Metge et al.65




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
