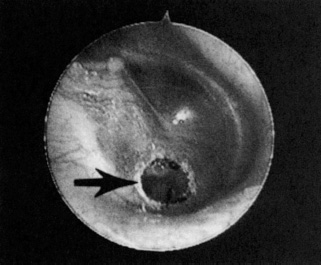
27 The current medical climate encourages the development of minimally invasive, cost-effective approaches to existing medical problems. Technological advances aid the rapid development of new procedures fulfilling these requirements. Ideally, these procedures are designed to take place in an office-based setting. Otolaryngologists are well positioned to take advantage of these procedures and pass the benefits along to their patients. These benefits include decreases in health care costs, operative time, exposure to general anesthesia, and postoperative morbidity. Various otologic procedures are now performed safelyand effectively using office-based techniques without compromising results. Middle ear exploration can be performed using the latest equipment in a minimally invasive fashion. The two instruments contributing most to the success of office-based otologic surgery are the CO2 laser and the otoendoscope. The CO2 laser creates an instant, bloodless, and nearly painless myringotomy, providing temporary middle ear ventilation as well as access for otoendoscopy. The otoendoscope provides near microscope quality images of the middle ear, allowing the surgeon to observe for perilymphatic fistula (PLF) and cholesteatoma, evaluate an unexplained conductive hearing loss, and view the round window membrane and eustachian tube orifice prior to instillation of intratym-panic medications. These techniques are reviewed in the following chapter, along with the authors’ approach to inner ear and eustachian tube perfusion. ■ Laser-assisted Tympanostomy Myringotomy has long been used to treat serous otitis media (SOM) and conditions related to eustachian tube dysfunction. If pressure equalization tubes (PET) tubes are not concurrently placed, a myringotomy without PETs tubes heals in 2 to 3 days and is no more effective than medical therapy for SOM.1 Although the optimal length of time to aerate the middle ear to cure SOM is not known, it appears that the more chronic the problem, the longer the surgical aeration required to cure eustachian tube dysfunction. The CO2 laser enables the surgeon to create a tympanostomy that ventilates the middle ear for 2 to 4 weeks. This may provide adequate aeration while largely avoiding the problems associated with PET tube insertion, including persistent tympanic membrane perforation and otorrhea. Early intervention with the laser may decrease the number of patients who will eventually require a PET tube. Indications Laser-assisted tympanostomy (LAT) is offered to adult patients with SOM for whom medical management has failed or to those patients requiring immediate relief of symptoms of SOM (e.g., SOM in an only hearing ear). The majority of these adult patients present with middle ear effusions following upper respiratory tract infections or recent air travel. Patulous eustachian tube is another indication for the LAT procedure, to determine whether middle ear aeration will be effective in relieving the associated symptoms. LAT can provide middle ear ventilation prior to air travel for patients susceptible to barotrauma during descent. Cooperative children with persistent SOM are candidates for the procedure. Finally, LAT is performed to create a controlled bloodless opening for laser-assisted otoendoscopy. Surgical Technique Initially, the drum is anesthetized using topical tetra-caine anesthesia (as described in detail in earlier publications).2, 3 The tetracaine quickly and painlessly anesthetizes the drum (Table 27 The technique avoids the need for use of needles or the burning associated with phenol and is well tolerated by adults as well as children. Tetracaine is adequate anesthesia for LAT, but local anesthetic injections are required if middle ear instrumentation is required. The adult patient or older child is placed in the supine position wearing laser-approved safety goggles. The tympanic membrane is viewed through an operative microscope. The microscope is adapted for the model 1030 Sharplan CO2 laser (Lumenis Ltd., Yokneam, Israel) using a microslad optical delivery system. The tympanostomy technique has evolved from a focused beam technique to a defocused beam technique and most recently to a scanner technique in our practice. The SurgiTouch ENT flashscanner (Lumenis Ltd.) enables the surgeon to create a controlled tympanostomy of a predictable size and depth with a single burst of focused laser energy. The beam moves in a spiral pattern at a constant velocity resulting in char-free ablation and minimal depth of laser energy penetration. With the pulse duration set at 0.15 second, 15 to 20 W are used to penetrate the tympanic membrane when middle ear effusion is present. When no effusion is present, 10 to 15 W are used. A thin, atrophic drum requires a lower power setting, and a thicker tympanic membrane requires increased wattage. Middle ear effusion absorbs laser energy and allows a higher power to be directed at the tympanic membrane without inadvertently striking the promontory and causing pain. Occasionally, two or three bursts are necessary to penetrate the drum, which occurs when the laser beam is not focused sharply or the drum is thickened. The tympanostomy is placed anterior to the malleus when treating SOM, as traditionally used for the placement of PETs tubes. The tympanostomy site is made over the round window niche when performing inner ear perfusion, over the eustachian tube when treating the eustachian tube, and over the incus when conductive hearing loss is being evaluated. 1. Measure 160 mg of tetracaine powder into 1 mL vial 2. Mix with 0.2 mL isopropyl alcohol 3. Inspect ear canal to verify absence of obstructions or drum perforations 4. Place 0.2 mL of solution in ear canal for a minimum of 7 minutes 5. Drain and aspirate solution from ear canal completely to avoid entry into middle ear, which can cause severe vertigo 6. The tympanic membrane is anesthetized for > 1 hour; the ear canal skin and middle ear mucosa are not anesthetized (Used with permission from Silverstein H, Rosenberg SI, Poe D, Jackson LE. Minimally Invasive Otological Surgery. Clifton Park, NY: Thomson Learning; 2002:13.) If children do not tolerate lying supine and motionless underneath the microscope, the OtoLAM (Lumenis Ltd.) is utilized. The device is similar to an otoscope with a laser and TV camera attached. The procedure can be performed with the patient sitting up, even in a parent’s lap, and is generally well tolerated. Both patients and parents can watch the procedure on the TV monitor. The drum is visualized while the surgeon positions the OtoLAM and watches the TV monitor. When the circulating beam is brought into sharp focus, the laser is fired using settings of 15 to 20 W at 0.15 seconds. Sometimes, the loud noise of the laser frightens children; however, the procedure can be performed on any cooperative child. Postoperative Care Very little care is required in the postoperative period. The majority of patients experience immediate relief of their symptoms. Antibiotic eardrops are not routinely prescribed. Patients are counseled to avoid water exposure to the operated ear and are followed until the opening completely heals. Using dexamethasone (4 mg/mL) ear drops, self-administered by the patient three times daily, may delay healing and allow the tympanostomy to remain open longer, which is sometimes desired. It may also improve eustachian tube function more rapidly and more effectively. In addition, placement of a eustachian tube MicroWick (Microme-dics, Eagan, Minnesota) facilitates medication reaching the eustachian tube mucosa and is used in resistant cases of eustachian tube dysfunction. Results Over 1000 LAT procedures have been performed in the authors’ practice. LAT size has been correlated to patency time. LATs less than 1.0 mm in diameter typically heal within 2 weeks, LATs 1.5 mm heal within 3 weeks, and LATs 2.0 mm in size heal within 4 weeks. LAT successfully resolves persistent SOM in 80% of adult cases without the need for PET tube placement. Children of all ages tolerate the procedure well, and placement of PETs tubes is avoided in almost half (46%) of these patients.4 Complications Creating a laser opening in the drum of an atrophic membrane may result in no postoperative healing and permanent perforation. This has occurred in one case. Otorrhea is rare and is treated with antibiotic eardrops. Recurrent serous otitis can be treated with a repeat LAT. If two sequential LATs do not resolve the problem, then a pressure-equalizing tube is used with the third procedure. Discussion LAT is a useful office-based technique. Over 1000 LATs have been performed in our office with minimal complications. It enables the otolaryngologist to create an instant, near painless temporary opening into the middle ear in a predictable and repeatable fashion. LAT is well tolerated by adults and many children. LAT closure typically occurs over 2 to 4 weeks, depending upon the diameter of the LAT. SOM is usually cured, and PETs tubes are often avoided in children. The cost and risk of general anesthesia and the cost of an operating room are avoided. LAT also creates a bloodless field necessary for otoendoscopy. Finally, the majority of LATs heal spontaneously within 6 weeks with normal drum appearance and mobility. ■ Middle Ear Exploration by Otoendoscopy Endoscopy of the middle ear was introduced by Mer et al in 1967.5 They inserted a flexible fiberoptic endoscope through an existing tympanic membrane perforation. Eichner attempted to improve visualization using a rigid endoscope, but the 2.7 mm scope proved too large to be useful.6 Nomura, in 1982, was the first to pass an endoscope through a myringotomy incision examining an otherwise undisturbed middle ear cavity.7 The improved optics, illumination, and miniaturization of the endoscopes, coupled with the bloodless opening created by the CO2 laser, opened the way for continued advancements in office-based otoendoscopy. Middle ear otoendoscopy was popularized by Poe et al8, 9 in the early 1990s, as well as by our practice.10–12 Indications The technique of otoendoscopy has multiple applications in the office-based setting, and it also has multiple intraoperative applications.2 It is useful in evaluating the etiology of unexplained conductive hearing losses, examining the round window membrane prior to inserting the MicroWick, evaluating tympanic cavity masses, analyzing the status of the middle ear and ossicular chain prior to mastoid-tympanoplasty, and evaluating the patency of the eustachian tube in cases of recurrent SOM or patulous eustachian tube. When there is an obvious history of trauma or surgical manipulation, office endo-scopy is used to evaluate the round and oval windows for PLF. Surgical Technique Otoendoscopes have a length of 10 cm and a diameter of 1.7 mm and are shorter and narrower than standard nasal rigid endoscopes usually seen in an otolaryngology office. We utilize two different angled otoendoscopes with 0 and 30 degree views. The 30-degree angled scope is our most commonly used scope and provides visual perspectives of the middle ear not seen with direct microscopic visualization. The otoendoscopes have excellent optics and produce images of superior quality, comparable to the operating microscope. The otoendo-scope must be attached to a light source. Additional optional equipment includes a camera attachment to the endoscope, a color television monitor for viewing the image, and a VHS recorder and a color video printer for documenting the procedural findings. Multiple copies of the still photos can be immediately produced for placement in the office chart, for explaining the procedure to the patient, and for the patient’s personal medical records. The patient is placed in the supine position, and anesthesia is achieved with local infiltrative anesthetic. Tetracaine can be utilized if middle ear instrumentation is not anticipated, but care must be taken to avoid contact with the skin of the ear canal. A 2.0 mm LAT is performed, creating a bloodless opening for placement of the endoscope. For most applications, a posteroinferior LAT placement overlying the round window niche is desirable (Fig. 27 The posteroinferior LAT allows for visualization of the round window, incudostapedial joint, oval window, eustachian tube, and undersurface of the tympanic membrane. Cadaver studies have indicated that the round window niche is located 3.14 mm posterior from the umbo of the malleus at a 113 degree angle. Once the LAT is created, the 1.7 mm diameter, 10 cm length otoendoscope (0 or 30 degrees) is inserted to examine the tympanic cavity. The otoendoscope is held in the surgeon’s nondominant hand and steadied by placing it against the speculum. The dominant hand is left free to focus the lens and handle any instrumentation required during the procedure. The areas of interest in the middle ear are visualized and photographed. The otoendoscope is then removed, and the LAT is either patched with Gelfilm covered in antibiotic ointment or allowed to heal spontaneously. Water precautions are followed until the tympanic membrane is healed. FIGURE 27-1 A tympanostomy made with a single laser burst using the flashscanner attachment in a right ear allows excellent visualization of the round window niche. (Used with permission from Silverstein H, Rosenberg SI, Poe D, Jackson LE. Minimally Invasive Otological Surgery. Clifton Park, NY: Thomson Learning; 2002:24.) Results
Office-based Minor Surgery: Otoendoscopy and Inner Ear Perfusion
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


