13 Odontogenic Disorders
Overview
1 | What germ layers and which branchial arch give rise to the teeth? | • Ectoderm • First branchial arch as well as ectomesenchyme from the neural crest and mesoderm |
2 | Name the muscles of mastication. | • Masseter muscle • Medial pterygoid muscle • Lateral pterygoid muscle • Temporalis muscle |
3 | Name the teeth from lateral to medial. | • Molars: Third (wisdom tooth), second, first • Premolars: Second bicuspid/premolar, first bicuspid/premolar • Canines: Cuspid • Incisors: Lateral incisor, central incisor |
4 | Number the teeth according to the universal numbering system. ( | Count maxillary teeth from right to left: • No. 1: Right maxillary third molar • No. 16: Left maxillary third molar • No. 17: Mandibular left third molar • No. 32: Mandibular right third molar |
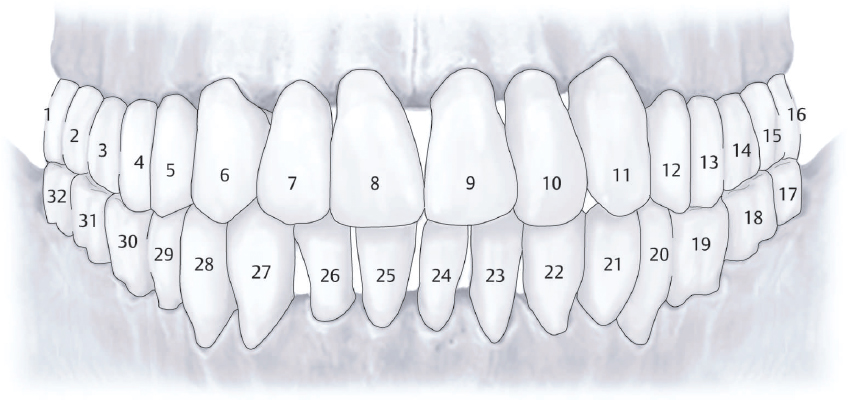
Fig. 13.1 Universal teeth numbering system. (Used with permission from Thieme Atlas of Anatomy: Head and Neuroanatomy, © Thieme 2007, illustration by Karl Wesker.)
5 | Name the origin, insertion, and function of the lateral pterygoid muscle. | • Origin: Superior head, greater wing of sphenoid; inferior head, lateral aspect of lateral pterygoid plate • Insertion: Superior head, articular disk; inferior head, condylar neck • Function: Opens and protrudes jaw |
Name the main components of the temporomandibular joint (TMJ) within the joint capsule from superior to inferior. ( | • Glenoid fossa • Superior joint space • Articular disk • Inferior joint space • Head of mandibular condyle |
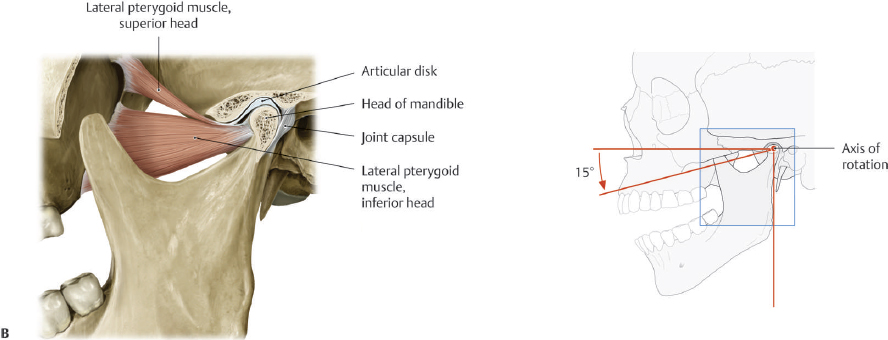
Fig. 13.2 Components of the temporomandibular joint. (Used with permission from Thieme Atlas of Anatomy: Head and Neuroanatomy, © Thieme 2007, illustration by Karl Wesker.)
7 | Describe the various surfaces of the teeth. ( | • Mesial: Toward the midline • Distal: Away from the midline • Facial: Toward the cheek or lips • Labial: Toward the lips (anterior teeth) • Buccal: Toward the cheeks (posterior teeth) • Lingual: Toward the tongue • Incisal: Toward the biting surface (anterior teeth) • Occlusal: Toward the biting surface (posterior teeth) • Apical: Toward the apex or tip of the root |
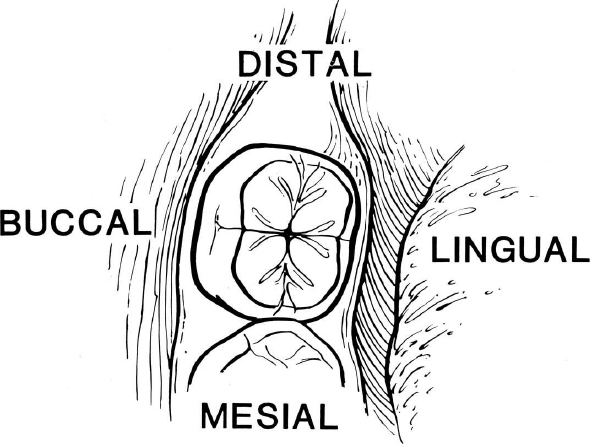
Fig. 13.3 Surfaces of the tooth. Mesial = toward the dental midline (the space between the central incisors); distal = away from the dental midline; buccal = adjacent to the cheek; lingual = adjacent to the tongue. (Used with permission from Edelstein DR, ed. Revision Surgery in Otolaryngology. New York, NY: Thieme; 2009.)
Describe the sensory innervation to the TMJ. | The masseteric, deep temporal, and auriculotemporal nerves (all branches of cranial nerve [CN] V3) supply the joint capsule. | |
9 | What are the three main layers of a tooth? ( | • Enamel • Dentin • Dental pulp |
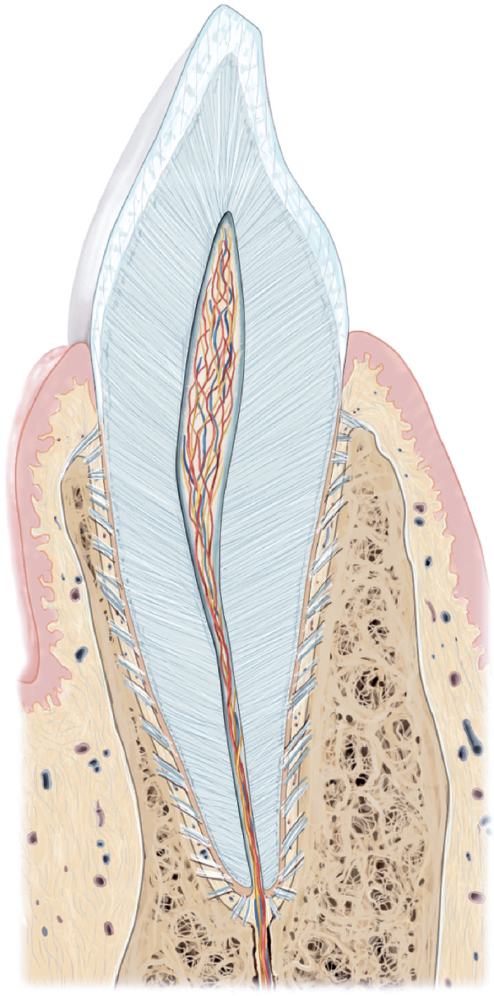
Fig. 13.4 Longitudinal section of a tooth and its layers. (Used with permission from Thieme Atlas of Anatomy: Head and Neuroanatomy, © Thieme 2007, illustration by Karl Wesker.)
What are the functions of the posterior teeth? | The premolars and molars grind food as well as establish a vertical dimension of occlusion. | |
11 | What are bone morphogenic proteins (BMPs)? | Proteins that are osteoinductive and are instrumental in regulating bone and cartilage development and formation |
12 | Describe the Angle classification of dental relationships. ( | • Class I: Normal occlusion, mesiobuccal cusp of the maxillary first molar aligns with the buccal groove of the mandibular first molar • Class II: Distoclusion (retrognathism), mesiobuccal cusp of the maxillary first molar mesial to the buccal groove • Class III: Mesioclusion (prognathism), mesiobuccal cusp of the maxillary first molar distal to the buccal groove |
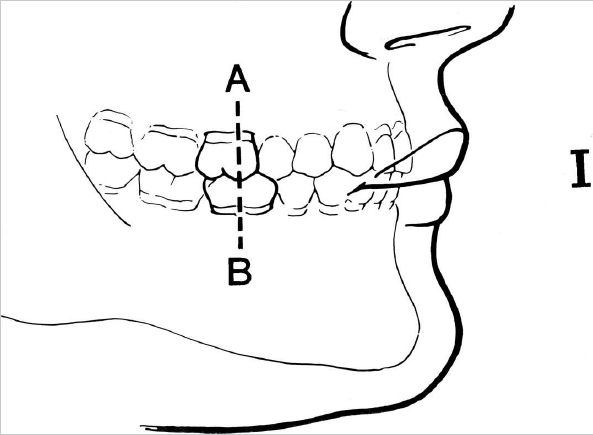
Fig. 13.5 Angle’s classification of occlusion: Class I (normal). The mesiobuccal cusp of the maxillary 1st molar aligns with the buccal groove of the mandibular first molar. (Used with permission from Donald PJ. The Surgical Management of Structural Facial Disharmony: A Self-Instructional Package. Washington, DC: American Academy of Otolaryngology–Head and Neck Surgery; 1985:13,14,15.)
13 | Describe the evaluation of a panoramic radiograph (orthopanotomogram). | Evaluation should include the teeth and any evidence of dental caries or periapical pathology, the alveolar and basal bone of the jaws, the inferior alveolar nerve canal, ramus and condyles, and maxillary sinuses; account for any impacted or missing/supernumerary teeth. |
14 | Describe the radiologic findings common to benign odontogenic tumors. | Common findings include radiolucency, often multilocular, and a propensity to expand the cortical boundaries of the jaw and push the inferior alveolar nerve inferiorly. Cortical margins are typically intact. Teeth may be displaced or roots resorbed (more aggressive malignancy will often show the whole root and a “tooth floating in space”). |
15 | Which anatomical regions are best visualized by standard dental X-rays? | Tooth-bearing regions of the maxilla and mandible are well demonstrated by dental films; the ramus, condylar region, and inferior aspect of the mandible are usually missed by most dental films (periapical and bitewing films). Panoramic radiographs show the jaws and the condyle more completely, but they are less accurate in diagnosing dental disease. Panorex is often distorted in the midline. |
16 | Describe the causes of osteoradionecrosis (ORN) of the mandible. | Radiation therapy results in endarteritis and fibrosis with resulting tissue becoming hypocellular, hypovascular, and hypoxic. ORN may develop spontaneously or even after minor trauma. Typical radiation thresholds for risk are 50 to 60 Gy. |
How long after radiation does ORN typically develop? | Onset is bimodal and peaks at both 3 months and 5 years after radiation. It can occur as early as 2 months and as late as 15 years. | |
18 | What are some signs and symptoms of mandibular ORN? | Deep bone pain, exposed bone with or without super-infection, trismus, fistula, halitosis, dysgeusia, pathologic fracture, paresthesia, anesthesia, and edema |
19 | What is the mechanism of bisphosphonate-related osteonecrosis of the mandible? | Bisphosphonates downregulate osteoclast function, resulting in impaired bone turnover and bone repair. They have also been found to inhibit angiogenesis. After even minor dentoalveolar trauma, affected bone has a limited capacity to heal and may develop osteonecrosis. Intravenous (IV) bisphosphonate use results in a significantly higher risk for development of osteonecrosis of the jaw. |
Temporomandibular Joint
20 | Name the two descriptive categories of TMJ disorders. Which is most common? | Extra-articular disorders and intra-articular disorders. Extra-articular disorders are far more common. |
21 | Contrast the findings in TMJ osteoarthritis and TMJ synovitis. | Osteoarthritis is a degenerative disease in the TMJ, as it is in other joints in the body. It is caused by a loss of articulating tissues and can be described as a mechanical, noninflammatory disease with bone-on-bone contact. By contrast, TMJ synovitis is definable by its inflammatory nature. Inflammatory mediators may accumulate secondary to trauma, disk malfunction, or parafunctional habits. |
22 | What is the best imaging modality for the TMJ? | Disk displacement and internal derangement of the TMJ are best imaged using MRI. Bony diseases such as ankylosis or degenerative joint disease are best evaluated using CT. Panorex may be used as to screen for fracture, condylar resorption, or large pathology. |
23 | How is TMJ internal derangement classified? | The Wilkes classification • Stage 1: Asymptomatic, painless clicking; mild disk displacement with reduction • Stage 2: Occasional painful clicking or locking; mild disk displacement and deformity • Stage 3: Joint pain with functional changes (limited opening); nonreducing disk with deformity • Stage 4: Chronic pain and functional deficit, degenerative osseous changes, and disk deformity • Stage 5: End stage with crepitus, degenerative joint disease (DJD), and disk perforation or loss |
24 | Name the two categories of TMJ disk displacement. | • Disk displacement with reduction (often heard as popping or clicking) • Disk displacement without reduction (usually no associated noise) Note: Often, displacement with reduction leads to displacement without reduction, which limits range of motion. This may be reversed with conservative therapy or with arthrocentesis or arthroscopy. |
25 | In the case of anterior disk displacement with or without reduction, what are the indications for intervention? | Pain, impaired mobility (especially acute closed lock), joint locking, failure to respond to conservative therapy Asymptomatic joint noise is common (in up to 35% of Americans). |
How does osteoarthritis of the TMJ manifest? | Degenerative joint disease or arthritis of the TMJ most commonly affects the elderly population, but it can affect all ages. Painful motion and joint loading are the hallmarks, along with CT findings of DJD. Myofascial pain symptoms must be ruled out. Unless related to ankylosis, it will not vastly reduce range of motion. | |
27 | What are the risk factors for septic TMJ arthritis? | History of trauma, burn, surgery or dental work, and systemic factors such as autoimmune disease, diabetes, immunosuppression, sexually transmitted infection, or prolonged steroid use |
28 | What is the most common systemic inflammatory condition to affect the TMJ? | Rheumatoid arthritis. Traditional rheumatologic laboratory studies in addition to MRI are useful for establishing a diagnosis. |
29 | What radiographic findings are expected in acute posttraumatic TMJ arthralgia? | Widening of the joint space might be seen, but radiographs may also be entirely normal. |
30 | How should trismus be clinically evaluated in a patient with head and neck cancer who has undergone radiation? | Objectively measure the mouth opening (opening < 35 mm is generally considered restricted) and compare with subjective assessment of restriction as well as its effect on daily functions. Assess for pain on opening or other symptoms besides simple restriction of opening from fibrosis. |
31 | What is the best initial therapy for postradiation trismus? | Stretching exercises, including insertion of stacked tongue blades or use of a commercial device such as Therabite. This requires multiple daily treatments over a period of months. |
32 | How should ankylosis of the TMJ be managed? |



