I. Conjunctival and uveal melanocytes (Fig. 17.1) are derived from the neural crest; pigment epithelial (PE) cells are derived from neuroepithelium or the layers of the optic cup. II. Dermal and conjunctival melanocytes are solitary dendritic cells. VI. Normal PE tends to vary little, if at all, among the races, and always appears heavily pigmented. VIII. The PE readily undergoes reactive proliferation but rarely becomes neoplastic. I. Lentigo A. Lentigo is similar clinically to an ephelis but is somewhat larger. C. Multiple lentigines syndrome D. Lentigo maligna (melanotic freckle of Hutchinson; circumscribed precancerous melanosis of Dubreuilh; Fig. 17.2) 1. Lentigo maligna occurs as an acquired pigmented lesion, mostly in adults older than 50 years of age. 2. It appears as a brown or black flat lesion, usually on the face, sometimes with involvement of the eyelids and conjunctiva (see subsection Primary Acquired Melanosis in section Melanotic Tumors of Conjunctiva, later), enlarging slowly in an irregular manner. A. A nevus is a congenital, hamartomatous tumor, flat or elevated, and usually well-circumscribed lesion. 1. It may be pigmented early in life or not until puberty or even early adulthood. 2. The nevus is composed of nevus cells that are atypical but benign-appearing dermal melanocytes. B. Five types: (1) junctional, (2) intradermal (Fig 17.3), (3) compound (Fig. 17.4), (4) blue (Fig. 17.5), and (5) congenital oculodermal melanocytosis (nevus of Ota) (Fig. 17.6) C. The familial atypical mole and melanoma (FAM-M) syndrome (dysplastic nevus syndrome; B–K mole syndrome) 2. The nevi appear at an early age (usually during adolescence) and increase in number throughout life. 3. Familial cases are inherited in an autosomal-dominant pattern; sporadic cases also occur. II. Junctional nevus A. A junctional nevus is flat, well circumscribed, and a uniform brown color. B. The nevus cells are located at the “junction” of the epidermis and dermis (see Fig. 17.4C). C. The nevus has a low malignant potential. III. Intradermal nevus (common mole; see Fig. 17.3) B. It has a brown to black color when pigmented; often, however, it is “flesh-colored.” C. The nevus cells are entirely in the dermis. 2. No inflammatory cells are present unless the nevus is inflamed secondarily. D. The nevus may be seen with proliferated Schwann elements (i.e., a neural nevus). E. An unusual intradermal (or subepithelial) nevus is the peripunctal melanocytic nevus. 2. The nevus cells are subepithelial and also infiltrate the orbicularis muscle fibers. F. Intradermal nevus probably has no malignant potential. IV. Compound nevus (see Fig. 17.4) A. It combines junctional and dermal components, and it is usually brown. B. The dermal component shows a normal polarity (see Fig. 17.4; i.e., cells closest to the epidermis are larger, plumper, rounder, and paler than the deeper cells). C. Spindle cell nevus (juvenile “melanoma,” Spitz nevus) is a special form of compound nevus that occurs predominantly in children, often as a solitary lesion on the face. 1. Histologically, it superficially resembles a malignant melanoma, but biologically it is benign. V. Blue nevus A. Blue nevus is usually flat and almost always pigmented from birth, appearing blue to slate-gray. B. Nevus cells are present deep in the dermis in interlacing fasciculi. 1. The cells are located deeper than junctional, dermal, or compound nevus cells. 3. It may be very cellular [i.e., a cellular blue nevus (see Fig. 17.5), which has a low malignant potential]. C. Unless the nevus is the large or giant congenital cellular type, it has no malignant potential. VI. Congenital oculodermal melanocytosis (nevus of Ota; see Fig. 17.6) A. The condition can be considered a type of blue nevus of the skin around the orbit (in the distribution of the ophthalmic, maxillary, and occasionally mandibular branches of the trigeminal nerve), associated with an ipsilateral blue nevus of the conjunctiva and a diffuse nevus of the uvea (i.e., ipsilateral congenital ocular melanocytosis). 1. Skin pigmentation is usually prominent, but it may be quite subtle. 2. It is quite common in black and Asian patients but unusual in white patients. 3. Rarely, congenital oculodermal melanocytosis is bilateral. B. The diffuse uveal involvement causes heterochromia iridum (i.e., the involved eye is darker than the uninvolved iris). D. Congenital ocular melanocytosis (see earlier) E. Congenital oculodermal melanocytosis is potentially malignant only when it occurs in white patients. I. General information (Figs. 17.7 and 17.8) 2. An emerging epidemic of melanoma appears to be on the horizon. B. Melanoma involves the lower lid two-thirds more often than the upper lid. C. Associated histologic findings include solar elastosis, nevus, and basal cell carcinoma. D. Cuticular melanomas show a nonrandom alteration of chromosome 6. III. Skin melanomas are not classified according to cell type, as are uveal melanomas.2 B. Superficial spreading malignant melanoma 1. This type has only a vertical growth phase, involves the dermis early, and has the worst prognosis. D. Acrolentiginous melanoma occurs on the palms, soles, and terminal phalanges. F. Mucous membrane malignant melanoma (see discussion of conjunctival melanoma, later in this chapter). IV. Histology A. Normal polarity is lost (i.e., the deep cells are indistinguishable from superficial cells). B. The overlying epithelium is invaded. C. The cells of the neoplasm are atypical. 1. The nuclear-to-cytoplasmic ratio is increased, and large abnormal cells may be seen. 2. Mitotic figures may be present, but frequently they are absent. D. Often, an underlying inflammatory infiltrate of round cells, predominantly lymphocytes, is present. 2. Mitotic figures are usually present in the dermal component. 3. Melanomas greater than 1.5 mm in depth carry a distinctly worse survival rate. V. Prognosis B. Superficial, spreading malignant melanoma has a 75% survival rate. D. The level of expression of at least three integrin subunits is correlated with melanoma progression. I. An ephelis (freckle) is a brown, patchy, flat lesion with irregular borders, most often involving the bulbar conjunctiva near the limbus but sometimes the bulbar or palpebral conjunctiva. A. The pigmented conjunctiva is movable over the sclera. B. The lesion is present at birth. II. Freckles are common in dark races. I. General information (Figs. 17.9–17.12) A. A nevus is a hamartomatous, congenital, flat or elevated, well-circumscribed lesion that may not become pigmented until puberty or early adulthood. 2. They are almost entirely restricted to the epibulbar surface, the plica, the caruncle (see Fig. 17.11), and the lid margin. 4. Nevi are rarely located in the palpebral conjunctiva (1%), fornix (1%), or cornea (<1%). 5. Over time, a change in color may be seen in 13% of lesions, and the size may change in 8%. C. A nevus is the most common conjunctival tumor and consists of five “classic” types: 1. Junctional 2. Subepithelial (analogous to intradermal nevus of skin) 3. Compound 4. Blue a. Congenital ocular melanocytosis (melanosis oculi) b. Congenital oculodermal melanocytosis (nevus of Ota) 6. Unusual types of conjunctival nevi
Ocular Melanocytic Tumors
Normal Anatomy
Ocular Melanocytes
Melanotic Tumors of Eyelids
Ephelis (Freckle)
Lentigo
Nevus1
Heterochromia iridum (see Table 17.2) is a difference in pigmentation between the two irises, as contrasted to heterochromia iridis, which is an alteration within a single iris (e.g., occasionally, ipsilateral segmental heterochromia is caused by segmental ocular involvement; the alteration of pigmentation in the single iris is properly called heterochromia iridis).
Malignant melanomas have been reported in the skin, conjunctiva, uvea (most common), orbit (rarely), and even in the meninges.
Malignant Melanoma
Rarely, a primary lid melanoma can occur in conjunction with an ipsilateral primary conjunctival melanoma.
Melanotic Tumors of Conjunctiva
Ephelis (Freckle)
Nevus
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Ocular Melanocytic Tumors
17
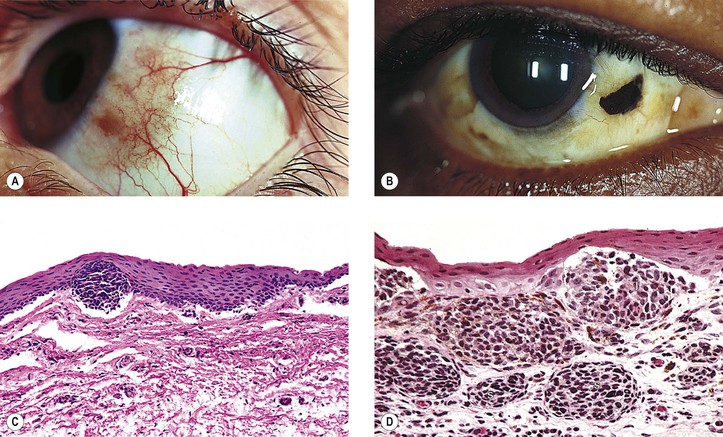
Fig. 17.1 Ocular melanocytes. Normally, the epidermal melanocytes appear in hematoxylin and eosin-stained sections as clear cells wedged between basal epithelial cells. Melanin is transferred by the dendritic processes of the melanocytes to the basal keratocytes, where it is stored and later degraded. A, In this tangential section of “reactive” epidermis, the usually clear melanocytes contain pigment around their nuclei and in their dendritic processes, making them easily visible (see Fig. 1.27C). B, A flat preparation of retinal pigment epithelium (RPE) of owl monkey shows the epithelial sheet configuration. RPE cells have a basement membrane (inner or cuticular portion of Bruch’s membrane) and are attached to one another near their apexes by terminal bars that contain “tight junctions.” C, Cross-section of the retina and choroid compares the epithelial nature of RPE with the nonepithelial individual and solitary choroidal melanocytes. The RPE cells have larger pigment granules than the choroidal melanocytes (see Fig. 9.2C). D, Thin section shows RPE pigment granules are considerably larger than those in choroidal melanocytes. Large nonpigmented cells in choroid (center toward bottom) are probably ganglion cells.
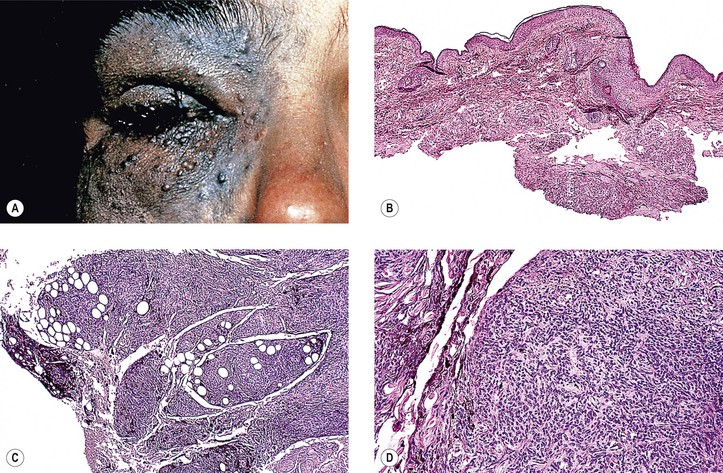
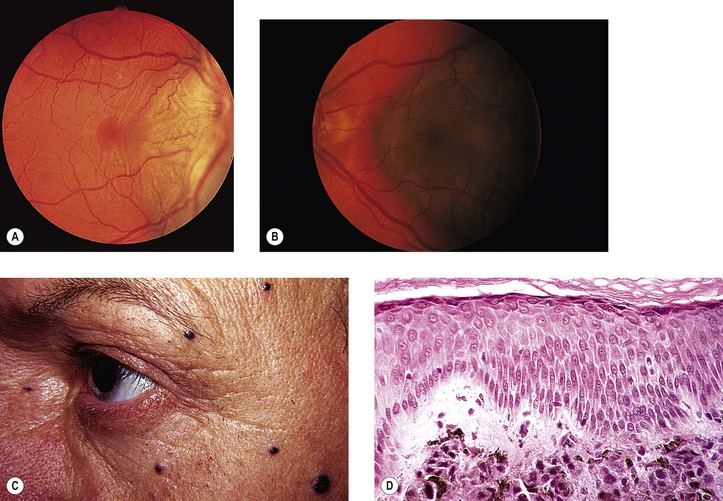
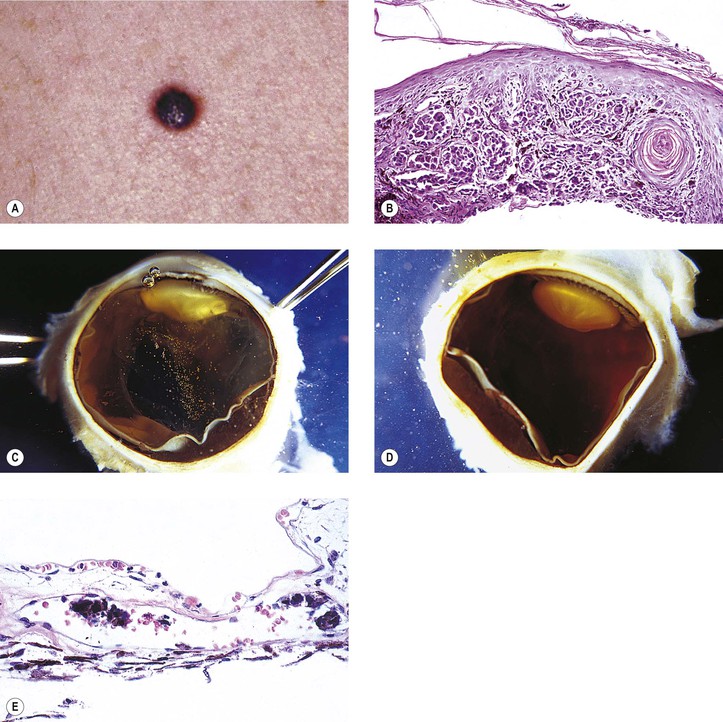
Fig. 17.7 Malignant melanoma of skin. A (OD) and B (OS), Patient presented with bilateral pigmented choroidal tumors. C, Same patient shows multiple pigmented skin tumors. D, Biopsy of skin tumor shows melanoma cells in dermis, sparing the junctional and epithelial locations, characteristic of metastatic melanoma—see Fig. 17.8. (Case referred by Drs. RC Lanciano, Jr. and S Bresalier.)
Fig. 17.8 Malignant melanoma of skin. A, Primary nodular malignant melanoma of skin found on back of patient shown in Fig. 17.7. Melanoma had metastasized to skin elsewhere and to both eyes. B, Biopsy shows melanoma cells in the junctional location and invading the epidermis, characteristic of primary melanoma. C and D, Gross specimens show right and left eyes removed at autopsy. Partially necrotic choroidal tumors seen. E, Pigmented melanoma cells are seen in a large vessel in the choroid. Most of the tumor cells in the choroid were necrotic. (Case referred by Drs. RC Lanciano, Jr. and S Bresalier.)