33
Ocular Histoplasmosis and Non-AMD Disorders Associated with Choroidal Neovascularization
Odette M. Houghton  Travis A. Meredith
Travis A. Meredith
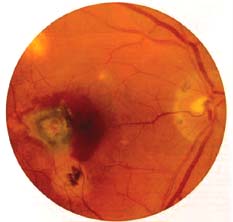
Choroidal neovascularization (CNV) can occur in presumed ocular histoplasmosis syndrome (POHS) as well as in other non–age-related macular degeneration (AMD) related disorders including pathologic myopia, angioid streaks, punctate inner choroidopathy (PIC), and multifocal choroiditis (MFC) (1–5). Since CNV can lead to severe loss of central vision in these disorders, several treatment approaches have been explored.
Various surgical techniques have been proposed as a treatment for CNV attributable to POHS and other non-AMD related disorders. The earliest reports on the surgical intervention of CNV were in patients with end-stage AMD. De Juan and Machemer were the first to describe the surgical excision of CNV (6). They gained direct exposure of the membrane by the creation of a large flap retinotomy. Blinder et al. subsequently described a surgical technique which similarly permitted direct access to the membrane (7). Unlike De Juan and Machemer, who describe the creation of a 180-degree peripheral retinotomy, Blinder et al. created a flap retinotomy, which encompassed the macula. Although the membranes were successfully removed using these methods, the postoperative result was complicated by poor visual acuity.
An alternative surgical approach, in which the subretinal space was accessed via a small retinotomy, was described in two patients with POHS by Thomas and Kaplan in 1991 (8). Subretinal manipulation of the membrane was aided by the creation of an overlying neurosensory retinal detachment via a subretinal infusion of fluid. This enabled the passage of instruments to dislodge and grasp the membrane. Both patients in this report experienced a dramatic improvement in visual acuity. Modifications of this technique have been used extensively in studies regarding the surgical removal of CNV (9–13).
Macular translocation has recently emerged as a strategy for the management of subfoveal CNV. The objective of this technique is to create a retinal detachment to relocate the fovea to a bed of healthier retinal pigment epithelium (RPE) (14). The first presentation of macular translocation in humans was in patients with submacular hemorrhage from AMD (14). Relocation of the fovea was accomplished by the creation of a total retinal detachment and a 360 degrees retinotomy, followed by rotation then reattachment of the retina. A different technique of limited translocation with scleral imbrication was used by de Juan et al. (15). Their approach involved creating a subtotal retinal detachment via a subretinal infusion, scleral shortening by suturing crescent shaped partial thickness scleral resections and retinal reattachment. Preliminary results were encouraging. This technique plus modifications of this technique, with scleral shortening achieved via scleral sutures without scleral resection, appear to be the most predominant method used in more recent studies (16–20).
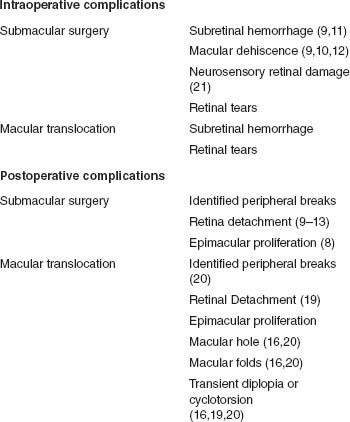
In entertaining a decision of surgery for CNV, the intraoperative and postoperative risks of the procedure must be taken into consideration. In addition to the specific complications associated with excising the CNV or relocating the macula, risks inherent to pars plana vitrectomy are also associated with these surgeries. Some of the reported intraoperative and postoperative complications are listed in Table 33-1.
The outcomes of CNV excision are varied and depend on the etiology of the CNV. The visual outcome of non–AMD-related CNV are listed in Table 33-2. The best candidates for this approach are considered to be those with POHS (10). Early studies investigating submacular surgery for CNV attributable to POHS were retrospective, noncontrolled and had limited follow-up (9–12). Together these studies showed that 74% to 83% of eyes experienced stable or improved visual acuity after the surgical removal of subfoveal CNV.
TABLE 33-1 COMPLICATIONS OF SURGERY FOR CHOROIDAL NEOVASCULARIZATION IN NON–AMD-RELATED DISORDERS
The Submacular Surgery Trial (SST) group H directly compared surgical intervention versus observation for the management of subfoveal CNV secondary to POHS and idiopathic membranes in a randomized manner (13). The findings of this study indicate that surgical removal of CNV did not offer an advantage over observation. The results did suggest that surgical removal of subfoveal CNV may be beneficial in patients with a best-corrected visual acuity <20/100. However, in light of the complications observed no strong recommendations can be made from these data.
Based on short term and retrospective results, encouraging submacular surgical outcomes have been obtained for patients with peripapillary CNV secondary to POHS extending to the subfoveal region (21–31). It appears that there may be a more favorable prognosis in younger patients with peripapillary CNV (32).
There have been studies indicating that the surgical intervention of CNV associated with high myopia may offer better restoration and preservation of visual function compared to observation in these eyes (13,16,17
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


