Nystagmus and Related Ocular Motility Disorders
General Concepts and Clinical Approach
This chapter concerns abnormal eye movements that disrupt steady fixation and thereby degrade vision. In the first section, the mechanisms by which gaze is normally held steady to achieve clear and stable vision are discussed. Next are described the pathogenesis and clinical features of each of the disorders that disrupt steady gaze, including the various forms of pathologic nystagmus and saccadic intrusions. Finally, currently available treatments for these abnormal eye movements are summarized.
Normal Mechanisms for Gaze Stability
In order for a person to see an object best, its image must be held steady over the foveal region of the retina. Although the visual system can tolerate some motion of images on the retina, if this motion becomes excessive, vision declines. Furthermore, if the image is moved from the fovea to peripheral retina, it will be seen less clearly.
In healthy persons, three separate mechanisms work together to prevent deviation of the line of sight from the object of regard. The first is fixation, which
has two distinct components: (a) the visual system’s ability to detect retinal image drift and program corrective eye movements; and (b) the suppression of unwanted saccades that would take the eye off target. The second mechanism is the vestibulo-ocular reflex (VOR), by which eye movements compensate for head perturbations at short latency and thus maintain clear vision during natural activities, especially locomotion. The third mechanism is the ability of the brain to hold the eye at an eccentric position in the orbit against the elastic pull of the suspensory ligaments and extraocular muscles, which tend to return it toward central position. For all three gaze-holding mechanisms to work effectively, their performance must be tuned by adaptive mechanisms that monitor the visual consequences of eye movements.
has two distinct components: (a) the visual system’s ability to detect retinal image drift and program corrective eye movements; and (b) the suppression of unwanted saccades that would take the eye off target. The second mechanism is the vestibulo-ocular reflex (VOR), by which eye movements compensate for head perturbations at short latency and thus maintain clear vision during natural activities, especially locomotion. The third mechanism is the ability of the brain to hold the eye at an eccentric position in the orbit against the elastic pull of the suspensory ligaments and extraocular muscles, which tend to return it toward central position. For all three gaze-holding mechanisms to work effectively, their performance must be tuned by adaptive mechanisms that monitor the visual consequences of eye movements.
Types of Abnormal Eye Movements that Disrupt Steady Fixation: Nystagmus and Saccadic Intrusions
The essential difference between nystagmus and saccadic intrusions lies in the initial eye movement that takes the line of sight off the object of regard. For nystagmus, it is a slow drift (or “slow phase”), as opposed to an inappropriate saccadic movement that intrudes on steady fixation. After the initial movement, corrective or other abnormal eye movements may follow. Thus, nystagmus may be defined as a repetitive, to-and-fro movement of the eyes that is initiated by a slow phase (drift). Saccadic intrusions, on the other hand, are rapid eye movements that take the eye off target. They include a spectrum of abnormal movements, ranging from single saccades to sustained saccadic oscillations.
Differences Between Physiologic and Pathologic Nystagmus
Not all nystagmus is pathologic. Physiologic nystagmus preserves clear vision during self-rotation. Under most circumstances, for example, during locomotion, head movements are small and the VOR is able to generate eye movements that compensate for them. Consequently, the line of sight remains pointed at the object of regard. In response to large head or body rotations, however, the VOR alone cannot preserve clear vision because the eyes are limited in their range of rotation. Thus, during sustained rotations, quick phases occur to reset the eyes into their working range: Vestibular nystagmus. If rotation is sustained for several seconds, the vestibular afferents no longer accurately signal head rotation, and visually driven or optokinetic nystagmus takes over to stop excessive slip of stationary retinal images. In contrast to vestibular and optokinetic nystagmus, pathologic nystagmus causes excessive drift of stationary retinal images that degrades vision and may produce illusory motion of the seen world: Oscillopsia. An exception is congenital nystagmus, which may be associated with normal visual acuity and which seldom causes oscillopsia.
Nystagmus, both physiologic and pathologic, may consist of alternating slow drifts (slow phases) in one direction and corrective, resetting saccades (quick phases) in the other: Jerk nystagmus (Fig. 21.1A). Pathologic nystagmus may, however, also consist of smooth to-and-fro oscillations: Pendular nystagmus (Fig. 21.1D). Conventionally, jerk nystagmus is described according to the direction of the quick phase. Thus, if the slow movement is drifting up, the nystagmus is called “downbeating”; if the slow movement is to the right, the nystagmus is “left beating.” Although it is convenient to describe the frequency, amplitude, and direction of the quick phases of the nystagmus, it is the slow phase that reflects the underlying abnormality.
Nystagmus may occur in any plane, although it is often predominantly horizontal, vertical, or torsional. Physiologic nystagmus is essentially conjugate. Pathologic nystagmus, on the other hand, may have different amplitudes in the two eyes (dissociated nystagmus), may go in different directions leading to different trajectories of nystagmus in the two eyes, or may have different temporal properties; that is, phase shift between the two eyes, leading to movements that are sometimes in opposite directions (disconjugate nystagmus).
Methods of Observing, Eliciting, and Recording Nystagmus
It is often possible to diagnose the cause of nystagmus through careful history and systematic examination of the patient. History should include duration of nystagmus, whether it interferes with vision and causes oscillopsia, and accompanying neurologic symptoms. The physician should also determine if nystagmus and attendant visual symptoms are worse with viewing far or near objects, with patient motion, or with different gaze angles (e.g., worse on right gaze). If the patient habitually tilts or turns the head, the physician should determine if these features are evident in old photographs.
Before assessing eye movements, the physician must examine the visual system to determine if the patient has any congenital or acquired afferent deficits that may indicate the cause of the nystagmus. The stability of fixation should be assessed with the eyes close to central position, viewing near and far targets, and at eccentric gaze angles. It is often useful to record the direction and amplitude of nystagmus for each of the cardinal gaze positions. If the patient has a head turn or tilt, the eyes should be observed in various
directions of gaze when the head is in that position as well as when the head is held straight. During fixation, each eye should be occluded, in turn, to check for latent nystagmus. The presence of pseudo-nystagmus and oscillopsia in patients with head tremor who have lost their VOR must be differentiated from true nystagmus.
directions of gaze when the head is in that position as well as when the head is held straight. During fixation, each eye should be occluded, in turn, to check for latent nystagmus. The presence of pseudo-nystagmus and oscillopsia in patients with head tremor who have lost their VOR must be differentiated from true nystagmus.
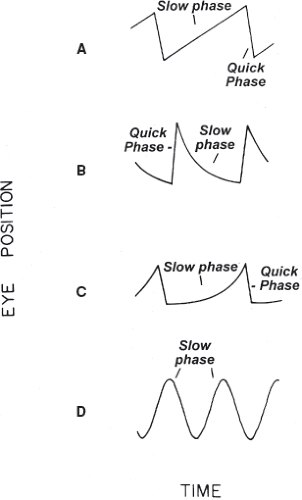 Figure 21.1 Four common slow-phase waveforms of nystagmus. A: Constant-velocity drift of the eyes. This occurs in nystagmus caused by peripheral or central vestibular disease and also with lesions of the cerebral hemisphere. The added quick phases give a “saw-toothed” appearance. B: Drift of the eyes back from an eccentric orbital position toward the midline (gaze-evoked nystagmus). The drift shows a negative exponential time course, with decreasing velocity. This waveform reflects an unsustained eye position signal caused by a “leaky” neural integrator. C: Drift of the eyes away from the central position with a positive exponential time course (increasing velocity). This waveform suggests an unstable neural integrator and is usually encountered in congenital nystagmus. D: Pendular nystagmus, which is encountered as a type of congenital nystagmus and with acquired brainstem disease. (Reprinted with permission from Leigh RJ, Zee DS. The Neurology of Eye Movements. 3rd ed. New York: Oxford University Press; 1999.) |
Subtle forms of nystagmus, due to low amplitude or inconstant presence, require prolonged observation over 2 to 3 minutes. Low-amplitude nystagmus may be detected only by viewing the patient’s retina with an ophthalmoscope. Note, however, that the direction of horizontal or vertical nystagmus is reversed when viewed through the ophthalmoscope. The effect of removal of fixation should always be determined. Nystagmus caused by peripheral vestibular imbalance may be apparent only under these circumstances. Lid closure will, of course, remove fixation, but lid closure itself may affect nystagmus. Thus, it is better to evaluate the effects of removing fixation with the eyelids open. Several clinical methods are available, such as Frenzel goggles: 10- to 20-diopter spherical convex lenses placed in a frame that has its own light source. The goggles defocus the patient’s vision, thus preventing fixation of objects, and also provide the examiner with a magnified, illuminated view of the patient’s eyes. An alternative is to use two high-plus spherical lenses from a trial case, or to determine the effect of transiently covering the viewing eye during ophthalmoscopy in an otherwise dark room.
Evaluation of nystagmus is incomplete without a systematic examination of each functional class of eye movements (vestibular, optokinetic, smooth pursuit, saccades, vergence) and their effect on the nystagmus because different forms of nystagmus can be directly attributed to abnormalities of some of these movements. For example, the vestibular system can be assessed with the oculocephalic maneuver or by rotating the patient in a swivel chair for 30 seconds, then stopping the rotation and observing the eyes for the development of postrotational nystagmus. The optokinetic system can be assessed by rotating a small drum or moving a tape on which a repetitive pattern is printed. The slow phases generated with this technique represent visual tracking, including smooth pursuit, whereas the resetting quick phases are saccadic in origin.
It is often helpful to determine the nystagmus waveform because the shape of the slow phase often provides a pathophysiologic signature of the underlying disorder. To properly characterize nystagmus, it is important to measure eye position and velocity, as well as target position, during attempted fixation at different gaze angles, in darkness, and during vestibular, optokinetic, saccadic, pursuit, and vergence movements. Common slow-phase waveforms of nystagmus are shown in Figure 21.1.
Conventionally, nystagmus is measured in terms of its amplitude, frequency, and their product: intensity; however, visual symptoms caused by nystagmus usually correlate best with the speed of the slow phase and displacement of the image of the object of regard from the fovea.
There are many different methods now available for recording eye movements. Because many patients with nystagmus cannot accurately point their eyes at visual targets, precise measurement is best achieved with the magnetic search coil technique. This is the only technique that permits precise measurement of horizontal, vertical, and torsional oscillations over an extended range of amplitudes and frequencies. Although originally introduced as a research tool, the technique is now widely used to evaluate clinical disorders of eye movements and is well tolerated.
Classification of Nystagmus Based on Pathogenesis
The classification of nystagmus starts by relating the various forms of nystagmus to disorders of visual fixation, the VOR, or the mechanism for eccentric gaze holding.
Nystagmus Associated with Disease of the Visual System and Its Projections to Brainstem and Cerebellum
Origin and Nature of Nystagmus Associated with Disease of the Visual Pathways
Disorders of the visual pathways are often associated with nystagmus. The most obvious example is the nystagmus that accompanies blindness. At least two separate mechanisms are responsible: dysfunction of the visual fixation mechanism itself and dysfunction of the visually mediated calibration mechanism that optimizes its action. The smooth visual fixation mechanism normally stops the eyes from drifting away from a stationary object of regard. This fixation mechanism depends upon the motion detection portion of the visual system that is inherently slow, with a response time of about 100 msec that encumbers all visually mediated eye movements, including fixation, smooth pursuit, and optokinetic responses. If the response time is delayed further by disease of the visual system, the attempts by the brain to correct eye drifts may actually add to the retinal error rather than reduce it, thus leading to ocular oscillations.
Vision is also needed for recalibrating and optimizing all types of eye movements. These functions depend on visual projections to the cerebellum. Lesions at any part of this recalibration pathway can deprive the brain of signals that hold each of the eyes on the object of regard, the result being drifts of the eyes off target, leading to nystagmus.
Clinical Features of Nystagmus with Lesions Affecting the Visual Pathways
Disease of the Retina
Congenital or acquired retinal disorders causing blindness, such as Leber congenital amaurosis, lead to continuous jerk nystagmus with components in all three planes and that changes direction over the course of seconds or minutes. This nystagmus is associated with a drifting “null point”—the eye position at which nystagmus changes direction—that probably reflects inability to calibrate the ocular motor system. This type of nystagmus often shows an increasing-velocity waveform (Fig. 21.1C). Recent developments in gene therapy for retinal disorders suggest that if vision can be restored, this type of nystagmus will be suppressed.
Disease Affecting the Optic Nerves
Optic nerve disease is commonly associated with pendular nystagmus. With unilateral disease of the optic nerve, nystagmus largely affects the abnormal eye, resulting in monocular or markedly asymmetric nystagmus. When both optic nerves are affected, the amplitude of nystagmus is often greater in the eye with poorer vision (the Heimann–Bielschowsky phenomenon). This phenomenon also occurs in patients with profound amblyopia, dense cataract, and high myopia (Video 21.1). Oscillations may disappear when vision is restored, supporting the contention that in such cases, the ocular oscillations are caused by loss of vision rather than by any primary disorder of the ocular motor system.
Disease Affecting the Optic Chiasm
Parasellar lesions such as pituitary tumors have traditionally, albeit rarely, been associated with seesaw nystagmus (see below). Seesaw nystagmus also occurs in persons whose optic nerve axons do not cross in the optic chiasm, such as some patients with severe albinism. Thus, it is possible that visual inputs, especially crossed inputs, are important for optimizing vertical–torsional eye movements and if interrupted, lead to seesaw oscillations.
Disease Affecting the Postchiasmal Visual Pathway
Horizontal nystagmus is a documented finding in patients with unilateral disease of the cerebral hemispheres, especially when the lesion is large and posterior. Such patients show a constant-velocity drift of the eyes toward the intact hemisphere (i.e., quick phases directed toward the side of the lesion, which is often low amplitude) and also usually show asymmetry of horizontal smooth pursuit that can be brought out using an optokinetic tape or drum. The response is reduced when the stripes move, or the drum is rotated, toward the side of the lesion. Whether this asymmetry occurs primarily
from impairment of parietal cortex necessary for directing visual attention or from disruption of cortical areas important for processing motion vision is unclear.
from impairment of parietal cortex necessary for directing visual attention or from disruption of cortical areas important for processing motion vision is unclear.
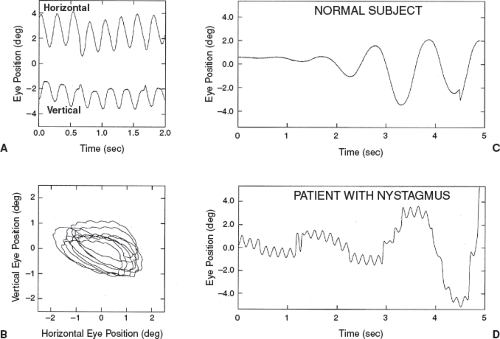 Figure 21.2 Acquired pendular nystagmus. Note both horizontal and vertical pendular waveforms. Represented as a function of time (A) or with coincident horizontal and vertical components at any given timepoint (B). Normal subject shows volitional, slow, smooth side-to-side movements (C) whereas a nystagmus patient has a much faster, smaller amplitude to-and-fro movement (D). |
Acquired Pendular Nystagmus and Its Relationship to Disease of the Visual Pathways
Acquired pendular nystagmus (Fig. 21.2) is one of the more common types of nystagmus and is associated with the most distressing visual symptoms. Its pathogenesis is undefined, and more than one mechanism may be responsible. It is encountered in a variety of conditions (Table 21.1).
Table 21.1 Etiology of Pendular Nystagmus | |||||||
|---|---|---|---|---|---|---|---|
|
Acquired pendular nystagmus usually has horizontal, vertical, and torsional components with the same frequency, although one component may predominate. The temporal waveform usually approximates a sine wave, but more complex oscillations have been noted. The frequency of oscillations ranges from 1 to 8 Hz, with a typical value of 3.5 Hz. For any particular patient, the frequency tends to remain fairly constant; only rarely is the frequency of oscillations different in the two eyes. In some patients, the nystagmus stops momentarily after a saccade (Video 21.2). This phenomenon is called postsaccadic suppression. Acquired pendular nystagmus may be suppressed or brought out by eyelid closure or evoked by convergence.
Acquired Pendular Nystagmus with Demyelinating Disease
Acquired pendular nystagmus is a common feature of acquired and congenital disorders of central
myelin, such as multiple sclerosis (MS), toluene abuse, Pelizaeus–Merzbacher disease, and peroxisomal disorders. Because optic neuritis often coexists in patients with MS who have pendular nystagmus, prolonged response time of the visual processing might be responsible for the ocular oscillations. However, the nystagmus often remains unchanged in darkness, when visual inputs should have no influence on eye movements. A more likely possibility is that visual projections to the cerebellum are impaired, leading to instability in the reciprocal connections between brainstem nuclei and cerebellum that are important for recalibration.
myelin, such as multiple sclerosis (MS), toluene abuse, Pelizaeus–Merzbacher disease, and peroxisomal disorders. Because optic neuritis often coexists in patients with MS who have pendular nystagmus, prolonged response time of the visual processing might be responsible for the ocular oscillations. However, the nystagmus often remains unchanged in darkness, when visual inputs should have no influence on eye movements. A more likely possibility is that visual projections to the cerebellum are impaired, leading to instability in the reciprocal connections between brainstem nuclei and cerebellum that are important for recalibration.
Oculopalatal Myoclonus (Oculopalatal Tremor)
Acquired pendular nystagmus may be one component of the syndrome of oculopalatal (pharyngo-laryngo-diaphragmatic) myoclonus. This condition usually develops several months after brainstem or cerebellar infarction, although it may not be recognized until years later. Oculopalatal myoclonus also occurs with degenerative conditions. The term “myoclonus” is misleading because the movements of affected muscles are to-and-fro and are approximately synchronized, typically at a rate of about 2 cycles per second. The palatal movements thus may be termed “tremor” rather than myoclonus, and the eye movements are really a form of pendular nystagmus. Although the palate is most often affected, movements of the eyes, facial muscles, pharynx, tongue, larynx, diaphragm, mouth of the eustachian tube, neck, trunk, and extremities may occur.
The ocular movements typically consist of to-and-fro oscillations. They often have a large vertical component, although they may also have small horizontal or torsional components. The movements may be somewhat disconjugate (both horizontally and vertically), with some orbital position dependency, and some patients show cyclovergence (torsional vergence) oscillations. Occasionally, patients develop the eye oscillations without movements of the palate, especially following brainstem infarction. Eyelid closure may bring out the vertical ocular oscillations. The nystagmus sometimes disappears with sleep, but the palatal movements usually persist. The condition is usually intractable, and spontaneous remission is uncommon.
The main pathologic finding with palatal myoclonus is hypertrophy of the inferior olivary nucleus (Fig. 21.3A), which may be seen using magnetic resonance (MR) imaging (Fig. 21.3B and C). There may also be destruction of the contralateral dentate nucleus. Histologically, the olivary nucleus has enlarged, vacuolated neurons with enlarged astrocytes. It has been postulated that the nystagmus of oculopalatal tremor results from instability in the projection from the inferior olive
to the cerebellar flocculus, a structure thought to be important in the adaptive control of the VOR.
to the cerebellar flocculus, a structure thought to be important in the adaptive control of the VOR.
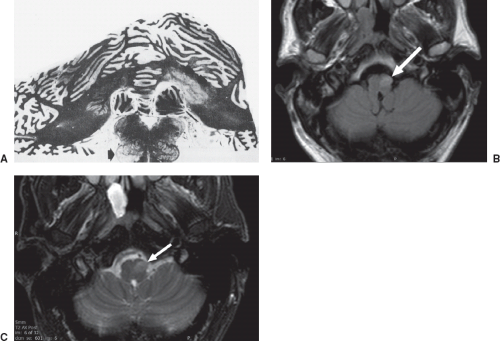 Figure 21.3 Pathology of oculopalatal myoclonus. A: Section through the cerebellum and medulla shows marked demyelination of the right dentate nucleus and restiform body. The left inferior olive is hypertrophic and shows mild demyelination (arrow). (Reprinted with permission from Nathanson M. Palatal myoclonus; further clinical and pathophysiological observations. Arch Neurol Psychiatr. 1956;75:285–296.) B: FLAIR and (C) T2-weighted imaging in a patient with oculopalatal myoclonus after resection of a pontine cavernous malformation, showing left hypertrophic olivary degeneration (arrows). |
Convergent-Divergent Pendular Oscillations
Vergence pendular oscillations occur in patients with MS, brainstem stroke, and cerebral Whipple disease. In Whipple disease, the oscillations typically have a frequency of about 1.0 Hz and are accompanied by concurrent contractions of the masticatory muscles, a phenomenon called oculomasticatory myorhythmia (Video 21.3). Supranuclear paralysis of vertical gaze also occurs in this setting and is similar to that encountered in progressive supranuclear palsy.
At least two possible explanations have been offered to account for the convergent-divergent nature of vergence pendular oscillations: A phase shift between the eyes, produced by dysfunction in the normal yoking mechanisms, or an oscillation affecting the vergence system itself. The latter explanation is more likely because patients who have been studied show no phase shift (i.e., are conjugate) vertically, and because the relationship between the horizontal and torsional components is similar to that occurring during normal vergence movements (excyclovergence with horizontal convergence).
Nystagmus Caused by Vestibular Imbalance
Nystagmus related to imbalance in the vestibular pathway can be caused by damage to peripheral or central structures. Because the nystagmus varies, it usually is possible to distinguish nystagmus caused by peripheral vestibular imbalance from nystagmus caused by central vestibular imbalance.
Nystagmus Caused by Peripheral Vestibular Imbalance
Clinical Features of Peripheral Vestibular Nystagmus
Disease affecting the peripheral vestibular pathway (i.e., the labyrinth, vestibular nerve, and its root entry zone) causes nystagmus with linear slow phases (Fig. 21.1A). Such unidirectional slow-phase drifts reflect an imbalance in the level of tonic neural activity in the vestibular nuclei. If disease leads to reduced activity, for example, in the vestibular nuclei on the left side, then the vestibular nuclei on the right side will drive the eyes in a slow phase to the left. In this example, quick phases will be directed to the right—away from the side of the lesion. Two features of the nystagmus itself are useful in identifying the vestibular periphery as the culprit: Its trajectory (direction) and whether it is suppressed by visual fixation.
The trajectory of nystagmus can often be related to the geometric relationships of the semicircular canals and to the finding that experimental stimulation of an individual canal produces nystagmus in the plane of that canal. Thus, complete unilateral labyrinthine destruction leads to a mixed horizontal–torsional nystagmus (the sum of canal directions from one ear), whereas in benign paroxysmal positional vertigo (BPPV), a mixed upbeat–torsional nystagmus reflects posterior semicircular canal stimulation. Pure vertical or pure torsional nystagmus almost never occurs with peripheral vestibular disease because this would require selective lesions of individual canals from one or both ears, an unlikely event.
Nystagmus caused by disease of the vestibular periphery often is more prominent, or may only become apparent, when visual fixation is prevented. The reason for this is that when visually generated eye movements are working normally, as they usually are in patients with peripheral vestibular disease, they will slow or stop the eyes from drifting.
Another common, but not specific, feature of nystagmus caused by peripheral vestibular disease is that its intensity increases when the eyes are turned in the direction of the quick phase—Alexander’s law. This probably reflects an adaptive strategy developed to counteract the drift of the vestibular nystagmus and so establish an orbital position (i.e., in the direction of the slow phases) in which the eyes are quiet and vision is clear. This phenomenon forms the basis for a common classification of unidirectional nystagmus. Nystagmus is called “first degree” if it is present only on looking in the direction of the quick phases, “second degree” if it is also present in the central position, and “third degree” if it is present on looking in all directions of gaze.
Although these clinical features help make the diagnosis of peripheral vestibular disease, it is important to realize that brainstem and cerebellar disorders may sometimes mimic peripheral disease and, especially in elderly patients or those with risk factors for vascular disease, careful observation is the prudent course.
Peripheral Vestibular Nystagmus Induced by Change of Head Position
Vestibular nystagmus is often influenced by changes in head position. This feature can be used to aid in diagnosis, especially of BPPV. Patients with BPPV complain of brief episodes of vertigo precipitated by change of head position, such as when they turn over in bed or look up to a high shelf. The condition may follow head injury or viral neurolabyrinthitis.
To test for nystagmus and vertigo in a patient with possible BPPV, the examiner should place the patient supine and turn the head toward one shoulder and then quickly move the head and neck together into a
head-hanging (down 30 to 45 degrees) position. About 2 to 5 seconds after the affected ear is moved to this dependent position, a patient with BPPV will report the onset of vertigo, and a mixed upbeat–torsional nystagmus, best viewed with Frenzel goggles, will develop. The direction of the nystagmus changes with the direction of gaze. Upon looking toward the dependent ear, it becomes more torsional; on looking toward the higher ear, it becomes more vertical. This pattern of nystagmus corresponds closely to stimulation of the posterior semicircular canal of the dependent ear (which causes slow phases mainly by activating the ipsilateral superior oblique and contralateral inferior rectus muscles). The nystagmus increases for up to 10 seconds, but it then fatigues and is usually gone by 40 seconds. When the patient sits back up, a similar but milder recurrence of these symptoms occurs, with the nystagmus being directed opposite to the initial nystagmus. Repeating this procedure several times will decrease the symptoms and make the signs more difficult to elicit. This habituation of the response is of diagnostic value because a clinical picture similar to that of BPPV can be caused by cerebellar tumors, MS, or posterior circulation infarction. With such central processes, however, there is no latency to onset of nystagmus and no habituation of the response with repetitive testing.
head-hanging (down 30 to 45 degrees) position. About 2 to 5 seconds after the affected ear is moved to this dependent position, a patient with BPPV will report the onset of vertigo, and a mixed upbeat–torsional nystagmus, best viewed with Frenzel goggles, will develop. The direction of the nystagmus changes with the direction of gaze. Upon looking toward the dependent ear, it becomes more torsional; on looking toward the higher ear, it becomes more vertical. This pattern of nystagmus corresponds closely to stimulation of the posterior semicircular canal of the dependent ear (which causes slow phases mainly by activating the ipsilateral superior oblique and contralateral inferior rectus muscles). The nystagmus increases for up to 10 seconds, but it then fatigues and is usually gone by 40 seconds. When the patient sits back up, a similar but milder recurrence of these symptoms occurs, with the nystagmus being directed opposite to the initial nystagmus. Repeating this procedure several times will decrease the symptoms and make the signs more difficult to elicit. This habituation of the response is of diagnostic value because a clinical picture similar to that of BPPV can be caused by cerebellar tumors, MS, or posterior circulation infarction. With such central processes, however, there is no latency to onset of nystagmus and no habituation of the response with repetitive testing.
Otolithic debris in the respective canals (canalolithiasis) interferes with the flow of endolymph or movement of the cupula and is probably responsible for BPPV. Neck movement causing vertebrobasilar kinking and vertigo as an isolated manifestation of transient brainstem ischemia is an uncommon mechanism; in such cases, associated neurologic symptoms are usually present.
Peripheral Vestibular Nystagmus Induced by Proprioceptive and Auditory Stimuli
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


