CHAPTER 13 Nucleus disassembly

The evolution of phacoemulsification from the procedure described by Kelman1 in the late 1960s to the techniques that we currently practice represents one of the greatest success stories of modern medicine. Understanding this historical development engenders understanding of the fundamental forces at work during phaco; therefore, we begin this section with a historical review of phaco technique.
Divide and conquer technique
Divide and conquer phaco, described by Gimbel2, was the first nucleofractis (two-instrument) cracking technique developed. After adequate hydrodissection, a deep crater is sculpted into the center of the nucleus, leaving a dense peripheral rim that can later be fractured into multiple sections. A shaving action is used to sculpt away the central nuclear material, and when this material is no longer accessible to the phaco probe, the lens should be rotated and additional central phaco performed to enlarge and deepen the crater. The size of the central crater should be expanded for progressively denser nuclei. Enough of the dense material must be left in place, however, to allow the phaco probe and second instrument to engage the rim and fracture the lens into sections. Notably, the peripheral nuclear rim stretches the entire capsular bag and acts as a safety mechanism to prevent the posterior capsule from suddenly moving anteriorly and being cut by the phaco probe. Once fractured, the lens sections should be left in place within the rim both to maintain the circular rim and to hold tension on the capsule rather than emulsifying them as they are broken away. Leaving the sections in place also facilitates rotation and the progressive fracturing of the remaining rim. After the rim is fractured around the entirety of its circumference, each segment can then be brought to the center of the capsule for safe emulsification.
Phaco fracture technique
In phaco fracture, a technique described by Shepherd3, the surgeon sculpts a groove from the 12- to 6-o’clock position after performing hydrodissection. Using the phaco handpiece and a second instrument, he or she then rotates the nucleus 90° and sculpts a second groove perpendicular to the first, in the form of a cross. Sculpting continues until the red reflex is seen at the base of the grooves, often requiring additional rotations and removal of nuclear material. At this point, a bimanual cracking technique is used to create a fracture through the nuclear rim in the plane of one of the grooves. The nucleus is then rotated 90°, and additional fractures are made until four separate quadrants are isolated. These are then tumbled toward the center of the capsule. A short burst of phaco power is used to embed the phaco tip into the bulk of the isolated quadrant and then, with the use of aspiration, the quadrant is gently pulled into the center for safe emulsification.
Chip and flip technique
Introduced by Fine4, and useful for softer grades of nuclei, this procedure relies on a nucleus that rotates freely within the capsular bag. Initially, a central bowl is sculpted in the nucleus until a thin central plate remains (the chip). The second instrument introduced through the side port incision engages the subincisional nuclear rim to move the inferior nuclear rim toward the center of the capsule bag. Clock-hour pieces of the rim are then carefully emulsified as the nucleus is rotated. Once the entire rim is removed, the second instrument is used to elevate the chip, which is then emulsified. The epinucleus is engaged at the 6-o’clock position with aspiration alone. As the phaco tip is moved superiorly, the second instrument pushes the epinucleus toward the 6-o’clock position thereby tumbling the epinuclear bowl and permitting it to be aspirated (the flip).
Crack and flip technique
Fine and colleagues modified Shepherd’s phaco fracture technique by adding hydrodelineation, resulting in the crack and flip technique4. Sculpting with minimal vacuum, relatively low aspiration flow, and low phaco power can be used to create two deep grooves at right angles to each other that extend to the golden ring, or the perimeter of the endonucleus, and permits bimanual nucleus cracking. Due to hydrodelineation of the epinucleus, only the endonucleus cracks.
Phaco chop
Koch and Katzen5 modified this procedure because they encountered difficulty in mobilizing the nuclear fragments. They created a central groove or central crater, depending on the density of the nucleus, which permits ease of removing the nuclear fragments liberated by the phaco chop technique.
Choo choo chop and flip
Fine described the ‘choo choo chop and flip’ technique in 19986. Subsequently, Fine, Packer, and Hoffman correlated the reduction of ultrasound energy with this technique to improvement in uncorrected postoperative day one visual acuity7. A 30° standard bevel down tip is used throughout endonuclear removal. After aspirating the epinucleus uncovered by the capsulorrhexis, a Fine/Nagahara chopper (Rhein Medical, Tampa, FL) is placed in the golden ring by touching the center of the nucleus with the tip and pushing it peripherally so that it reflects the capsulorrhexis. The chopper is used to stabilize the nucleus by lifting and pulling toward the incision slightly (Fig. 13.1), after which the phaco tip lollipops the nucleus. This can be done in either pulse mode at 2 pulses/second or 80 millisecond burst mode.

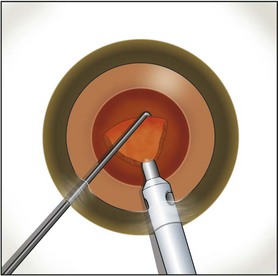
Burst mode is a power modulation that utilizes a fixed percentage power, a programmable burst width, and a linear interval between bursts. Phaco in burst mode or at this low pulse rate sounds like ‘choo-choo-choo-choo’; therefore, the name of this technique. With the energy delivered in this way, ultrasound energy into the eye is minimized and hold on the nucleus is maximized as vacuum builds between pulses or bursts. Because of the decrease in cavitational energy around the tip at this low pulse rate or in burst mode, the tunnel in the nucleus in which the tip is embedded fits the needle very tightly and allows excellent hold on the nucleus, thus maximizing control of the nucleus as it is scored and chopped (Fig. 13.2).The nucleus is scored by bringing the Fine/Nagahara chop instrument to the side of the phaco needle. It is chopped in half by pulling the chopper to the left and slightly down while moving the phaco needle to the right and slightly up. Then the nuclear complex is rotated. The chop instrument is again brought into the golden ring (Fig. 13.3), and the nucleus lollipopped, scored, and finally chopped with the resulting pie-shaped segment now lollipopped on the phaco tip (Fig. 13.4). The segment is then evacuated utilizing high vacuum and short bursts or pulse-mode phaco at 2 pulses/second. The nucleus is continually rotated so that pie-shaped segments, the size of which is driven by the density of the cataract, can be scored, chopped, and removed easily by the high vacuum and assisted by short bursts or pulses of phaco (Fig. 13.5).
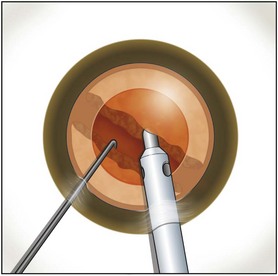
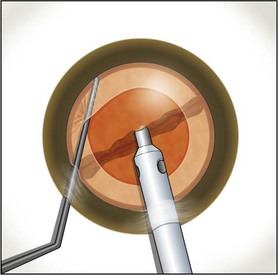
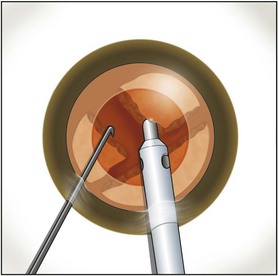
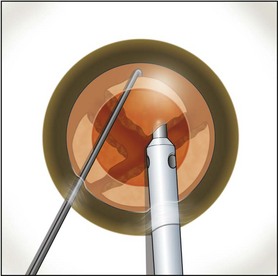
Fig. 13.5 An additional chop may be taken in the pie-shaped wedge if its density is relatively high.
After complete evacuation of the first heminucleus, the second heminucleus is rotated to the distal portion of the bag and the chop instrument stabilizes it while it is lollipopped. It is then scored and chopped (Fig. 13.6). The pie-shaped segments can be chopped a second time to reduce their size (Fig. 13.7) if they appear too large to easily evacuate.
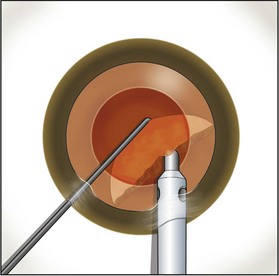
Fig. 13.6 After extraction of the first heminucleus, the remaining material is rotated distally and chopped.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


