The ocular motor system is separated anatomically and physiologically into infranuclear (peripheral), nuclear, internuclear, and supranuclear components. In this chapter, we consider ocular motor disturbances caused by congenital and acquired lesions of the nuclear and infranuclear neural structures—the lesions of the ocular motor nuclei and nerves.
Disorders that produce dysfunction of the oculomotor, trochlear, and abducens nerves may be located anywhere from the ocular motor nuclei to the termination of the nerves in the extraocular muscles within the orbit. Ocular motor nerve palsies may present in one of four ways:
As isolated partial or complete nerve palsy without any other neurologic signs and without symptoms except those related to the palsy itself.
In association with symptoms other than those related to the palsy (e.g., pain, dysesthesia, paresthesias) but without any signs of neurologic or systemic disease.
In association with other ocular motor nerve palsies (e.g., the simultaneous onset of an oculomotor palsy and an abducens palsy) but without any other neurologic signs.
In association with neurologic signs other than the ocular motor nerve palsy.
Oculomotor (Third) Nerve Palsies
Congenital
Congenital oculomotor nerve palsies constitute nearly half of the oculomotor nerve pareses seen in children (Fig. 18.1). Most cases are unilateral. As a general rule, patients with congenital oculomotor nerve palsies have no other neurologic or systemic abnormalities. Usually, these patients have some degree of amblyopia.
All patients with congenital oculomotor nerve palsy have some degree of ptosis, ophthalmoparesis, and pupillary involvement. In most of these cases, the pupil is miotic rather than dilated, presumably because of misdirected (aberrant) oculomotor nerve regeneration. Abnormalities of the oculomotor nerve that are present at birth may be caused by absent or incomplete development of the nucleus, nerve, or both. Injury to the oculomotor nerve during gestation or at the time of delivery may produce a congenital oculomotor nerve palsy. Such patients may or may not have other physical signs of trauma or other neurologic signs.
In addition to simple congenital oculomotor nerve palsy, several congenital syndromes implicate oculomotor maldevelopment with anomalous or paradoxic innervation of the extraocular muscles. These syndromes include (1) congenital adduction palsy with synergistic divergence, (2) atypical vertical retraction syndrome, and (3) cyclic oculomotor nerve paresis with cyclic spasm.
Congenital Adduction Palsy with Synergistic Divergence
Patients with this syndrome have congenital unilateral paralysis of adduction associated with simultaneous
bilateral abduction on attempted gaze into the field of action of the paretic medial rectus muscle (Fig. 18.2). Most patients with congenital adduction palsy with synergistic divergence have no other neurologic abnormalities.
bilateral abduction on attempted gaze into the field of action of the paretic medial rectus muscle (Fig. 18.2). Most patients with congenital adduction palsy with synergistic divergence have no other neurologic abnormalities.
 Figure 18.1 Congenital left oculomotor nerve palsy with aberrant regeneration in a child with a history of birth trauma. A: In primary position, there is a left hypotropia. Note the miotic left pupil. B: On attempted downward gaze, there is retraction of the left upper eyelid (pseudo-Graefe sign). |
Electromyographic studies in patients with this condition suggest that it is caused by absent oculomotor nerve innervation of the affected medial rectus muscle, combined with absent or minimal innervation of the lateral rectus muscle by the abducens nerve but with a branch of the oculomotor nerve innervating the lateral rectus muscle (Fig. 18.3).
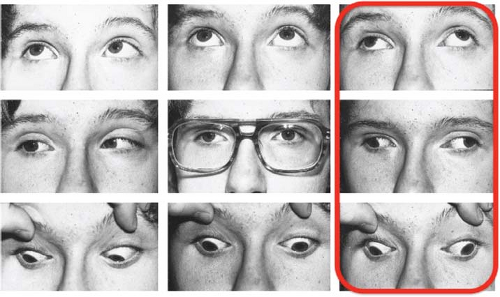 Figure 18.2 Congenital right adduction palsy and synergistic divergence. Extraocular movements in nine fields of gaze. The right eye abducts somewhat on attempted right lateral gaze, but also abducts on left lateral gaze. (Reprinted with permission from Wilcox LM Jr, Gittinger JW Jr, Breinin GM. Congenital adduction palsy and synergistic divergence. Am J Ophthalmol. 1981;91:1–7.) |
Vertical Retraction Syndrome
The main clinical feature of the vertical retraction syndrome is limitation of movement of the affected eye on elevation or depression, associated with a retraction of the globe and narrowing of the palpebral fissure. There may be an associated esotropia or exotropia on attempted vertical gaze, more marked in the direction of the restricted vertical field of action. The condition is usually unilateral. The results of both electro-oculography and electromyography in patients with this condition are consistent with anomalous oculomotor innervation of the vertical rectus muscles of the affected eye.
Oculomotor Paresis with Cyclic Spasms (Cyclic Oculomotor Paresis, COPS)
Cyclic oculomotor paresis is usually unilateral and is, in the majority of cases, present from birth. The typical patient with this condition has an oculomotor nerve paresis with ptosis, mydriasis, reduced accommodation, and ophthalmoparesis. About every 2 minutes, the ptotic eyelid elevates, the globe begins to adduct, the pupil constricts, and accommodation increases. These spasms last 10 to 30 seconds and then give way to the paretic phase. Cyclic oculomotor palsy usually continues throughout life.
Most patients with unilateral cyclic oculomotor paresis have reduced visual acuity in the affected eye
because of amblyopia. The syndrome is occasionally associated with other pathologic conditions, including birth trauma and congenital infections. Rarely, cases occur after an acquired oculomotor nerve palsy, such as from a posterior fossa tumor. However, patients with true congenital oculomotor nerve paresis with cyclic spasms do not require any workup unless they have other evidence of neurologic disease, or they give a history of progressive neurologic dysfunction. Carbamazepine has been shown to be helpful for some patients. COPS and ocular neuromyotonia (ONM) (discussed later in this chapter) likely share a similar pathogenetic mechanism; however, they differ in that COPS patients typically lack a history of previous radiation treatment and have pre-existing paresis of the oculomotor nerve, unlike ONM patients.
because of amblyopia. The syndrome is occasionally associated with other pathologic conditions, including birth trauma and congenital infections. Rarely, cases occur after an acquired oculomotor nerve palsy, such as from a posterior fossa tumor. However, patients with true congenital oculomotor nerve paresis with cyclic spasms do not require any workup unless they have other evidence of neurologic disease, or they give a history of progressive neurologic dysfunction. Carbamazepine has been shown to be helpful for some patients. COPS and ocular neuromyotonia (ONM) (discussed later in this chapter) likely share a similar pathogenetic mechanism; however, they differ in that COPS patients typically lack a history of previous radiation treatment and have pre-existing paresis of the oculomotor nerve, unlike ONM patients.
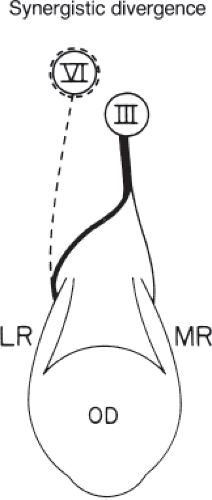 Figure 18.3 Anomaly of peripheral innervation that may explain synergistic divergence with congenital limitation of adduction. The oculomotor nerve provides major innervation of the lateral rectus muscle (which may or may not also be innervated by the abducens nerve). The thickness of the line representing the nerve represents quantitative innervation. Dashed lines indicate hypoplasia or aplasia of the abducens nucleus and/or nerve. OD, right eye; LR, lateral rectus muscle; MR, medial rectus muscle; III, oculomotor nucleus; VI, abducens nucleus. (Redrawn from Wilcox LM Jr, Gittinger JW Jr, Breinin GM. Congenital adduction palsy and synergistic divergence. Am J Ophthalmol. 1981;91:1–7.) |
Acquired
Acquired dysfunction of the oculomotor nerve is far more common than its congenital counterpart, being caused by nearly every pathologic process.
Lesions of the Oculomotor Nucleus
Lesions that damage the oculomotor nucleus are relatively uncommon. When they occur, they often produce bilateral defects in ocular motility, eyelid position, or both. The bilaterality of involvement is explained by the anatomy of the nucleus and its fibers. Both levator palpebrae superioris muscles are innervated by a single, midline subnucleus located at the caudal end of the oculomotor nerve complex (central caudal nucleus) (Fig. 18.4). A lesion that damages this region thus produces a bilateral, symmetric ptosis. In some cases, the ptosis is isolated, whereas in others, there is associated ophthalmoplegia.
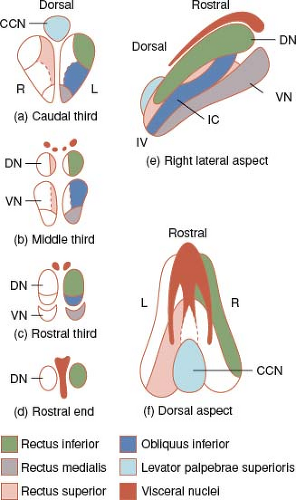 Figure 18.4 Warwick schema of topographic organization within the oculomotor nucleus. Note the caudal dorsal midline position of caudal central nucleus (CCN), the motor pool for the levator palpebrae superioris. The motor pool of the superior rectus (hashed area) is contralateral to the extraocular muscle it innervates. The visceral (parasympathetic) nuclei are shown in black. DN, dorsal nucleus; IC, intermediate column; IV, region of the trochlear nucleus; VN, ventral nucleus. (Reprinted with permission from Warwick R. Representation of the extra-ocular muscles in the oculomotor nuclei of the monkey. J Comp Neurol. 1953;98:449–504.) |
Lesions of the oculomotor nuclear complex may spare the central caudal nucleus. Patients with such lesions have fixed, dilated pupils and ophthalmoparesis affecting one or more of the muscles innervated by the oculomotor nerve but no ptosis.
A second anatomic feature of the oculomotor nuclear complex that results in bilateral ocular damage is the course of the nerve to the superior rectus muscle, which is crossed. The subnucleus for superior rectus function on either side of the brain stem gives rise to fibers that pass through the contralateral superior rectus subnucleus without synapse and innervate the contralateral superior rectus muscle. Lesions that affect this region thus cause not only ipsilateral weakness of superior rectus, medial rectus, inferior rectus, inferior oblique, or a combination of these muscles, but also limitation of elevation in the contralateral eye from impairment of superior rectus function on that side. Such patients have bilateral limitation of upward gaze, occasionally worse on the contralateral side (Figs. 18.5 and 18.6; Table 18.1).
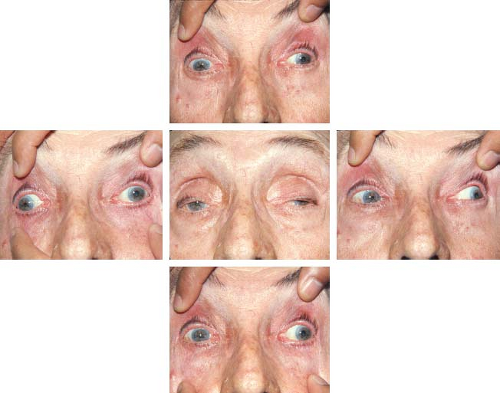 Figure 18.5 Nuclear oculomotor nerve palsy. There is a complete left oculomotor nerve palsy. In addition, however, there is absence of elevation of the right eye. The right eye also has marked limitation of depression, suggesting that the lesion is not limited to the left oculomotor nerve nucleus but also involves the right nucleus as well. Neither oculocephalic nor caloric stimulation produced any improvement in vertical gaze. |
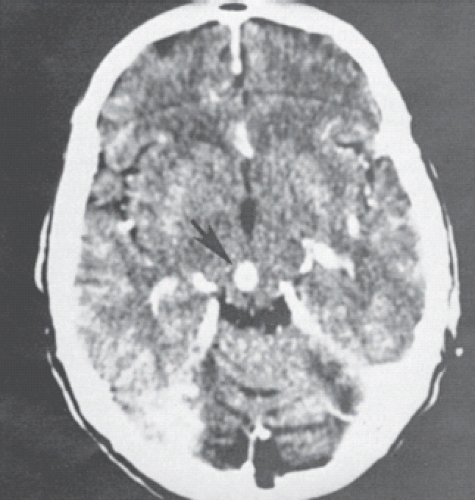 Figure 18.6 Computed tomographic scan in the patient whose appearance is seen in Figure 18.5. Note the enhancing lesion in the dorsal mesencephalon (arrow). |
Lesions of the oculomotor nucleus are most often caused by ischemia, usually from embolic or thrombotic
occlusion of small, dorsal perforating branches of the mesencephalic portion of the basilar artery or, less often, from occlusion of the distal portion of the basilar artery itself (“top of the basilar syndrome”). Other etiologies include hemorrhage, infiltration by tumor, inflammation, and brain stem compression.
occlusion of small, dorsal perforating branches of the mesencephalic portion of the basilar artery or, less often, from occlusion of the distal portion of the basilar artery itself (“top of the basilar syndrome”). Other etiologies include hemorrhage, infiltration by tumor, inflammation, and brain stem compression.
Table 18.1 Nuclear Oculomotor Nerve Palsy | |||||
|---|---|---|---|---|---|
|
Involvement of the immediate premotor mesencephalic structures located adjacent to the oculomotor nuclei complex may produce difficulties with ocular motility that may initially appear indistinguishable from direct damage to the nucleus itself. Such supranuclear defects can usually be distinguished from their nuclear and infranuclear counterparts by stimulation of the vestibular system using oculocephalic or caloric testing.
Lesions of the Oculomotor Nerve Fascicle
Fascicular lesions of the oculomotor nerves produce both complete and incomplete palsies that cannot be differentiated clinically from palsies caused by lesions outside the brain stem. Although most lesions that affect the fascicle produce an oculomotor nerve palsy with pupillary involvement, occasionally the pupil is spared. A fascicular oculomotor nerve palsy may occur as an isolated finding or in association with other neurologic signs (Fig. 18.7).
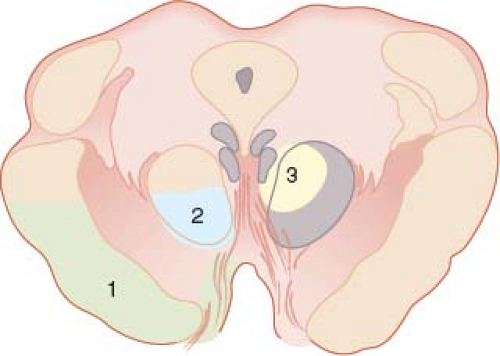 Figure 18.7 Diagram of a section through the mesencephalon showing regions in which the oculomotor nerve fascicle may be injured causing specific neurologic syndromes. (1) Weber syndrome. (2) Benedikt syndrome. (3) Claude syndrome (red nucleus and superior cerebellar peduncle). |
Fascicular oculomotor nerve palsies that are associated with other neurologic manifestations produce several characteristic syndromes. Lesions in the area of the brachium conjunctivum (superior cerebellar peduncle) may produce ipsilateral oculomotor nerve palsy and cerebellar ataxia (Nothnagel syndrome). The syndrome of ipsilateral oculomotor nerve palsy combined with contralateral involuntary movements (rubral hemitremor) is known as Benedikt syndrome and reflects damage to the red nucleus, especially its dorsocaudal portion, through which the oculomotor fascicle passes (see Fig. 18.7). Mesencephalic lesions ventral to the red nucleus may damage fascicular oculomotor fibers and motor fibers in the cerebral peduncle, producing an oculomotor nerve palsy with contralateral hemiplegia or hemiparesis, including the lower face and tongue (Weber syndrome) (Figs. 18.7 to 18.9). Simultaneous damage in the mesencephalon to the red nucleus and the brachium conjunctivum produces a syndrome with the features of both Benedikt and Nothnagel syndromes—oculomotor nerve paresis, contralateral asynergia, ataxia, dysmetria, and dysdiadochokinesia—called Claude syndrome (see Fig. 18.7). The majority of mesencephalic syndromes are vascular in origin and are caused by occlusion or other injury to the vascular area of the basilar artery or perforating branches of the posterior cerebral artery; however, Claude syndrome can result from thrombosis of the medial interpeduncular branch of the posterior cerebral artery.
Although divisional oculomotor nerve pareses are often caused by lesions in the cavernous sinus or posterior orbit, anatomic separation into superior and inferior divisions begins in the brain stem. Thus, rarely lesions of the oculomotor fascicles can cause isolated dysfunction of either the superior or inferior division of the oculomotor nerve. It is also possible that fascicular lesions can also cause isolated weakness of only one of the muscles innervated by the oculomotor nerve.
As with nuclear oculomotor palsies, fascicular lesions may be ischemic, hemorrhagic, compressive,
infiltrative, traumatic, or rarely, inflammatory. Because the fascicles are white matter tracts, demyelinating disease may also cause an oculomotor nerve paresis that may occur as an isolated phenomenon or associated with other neurologic manifestations.
infiltrative, traumatic, or rarely, inflammatory. Because the fascicles are white matter tracts, demyelinating disease may also cause an oculomotor nerve paresis that may occur as an isolated phenomenon or associated with other neurologic manifestations.
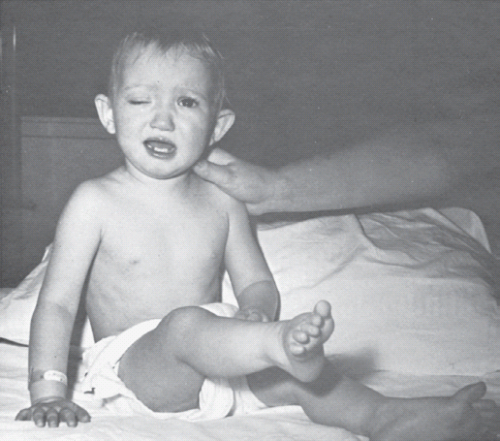 Figure 18.8 Weber syndrome produced by a brain stem glioma infiltrating the mesencephalon. Note the oculomotor nerve palsy on the right, and the hemiplegia on the left. |
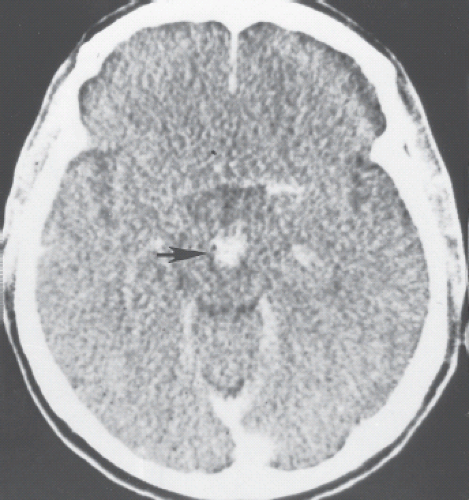 Figure 18.9 Computed tomogram in a patient with Weber syndrome showing an enhancing lesion in the ventral mesencephalon (arrow). The lesion was thought to be a solitary metastasis from a breast carcinoma. |
Lesions of the Oculomotor Nerve in the Subarachnoid Space
Lesions that damage the oculomotor nerve in the interpeduncular fossa may be located anywhere from the emergence of the nerve at the ventral surface of the mesencephalon to the point at which the nerve penetrates the dura beside the posterior clinoid process to enter the cavernous sinus (Fig. 18.10). Interpeduncular damage to the oculomotor nerve may be partial or complete. In some cases, the palsy is initially incomplete but progresses over hours, days, weeks, or even months. In most cases, there is some degree of accommodative paresis, but pupillary involvement is variable and depends primarily on the nature of the lesion. Oculomotor nerve dysfunction that is produced by damage to its subarachnoid portion may occur as (1) isolated pupillary dilation with a reduced or absent light reaction, (2) ophthalmoplegia with
pupillary involvement, or (3) ophthalmoplegia with normal pupillary size and reactivity.
pupillary involvement, or (3) ophthalmoplegia with normal pupillary size and reactivity.
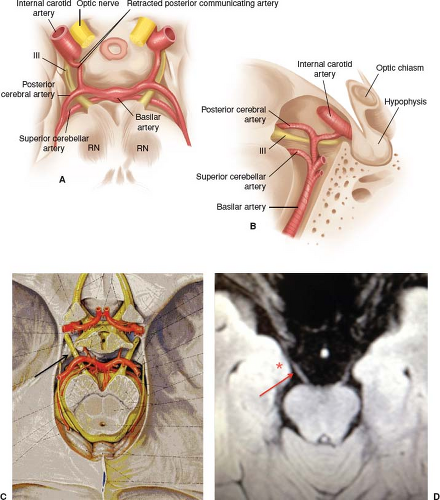 Figure 18.10 The relationship of the oculomotor nerve to the intracranial arteries in the subarachnoid space. A: The oculomotor nerves (III) are viewed from above. On the left, the posterior communicating artery has been retracted to show the groove that it may produce through its contact with the oculomotor nerve. RN, red nucleus. B: Lateral view of the left oculomotor nerve (III) showing its arterial relationships. C: Schematic showing the emergence of the oculomotor nerves from brain stem, accessing the cisternal region from in between the posterior cerebral and superior cerebellar arteries, traveling anterolaterally. D: T2-FLAIR MRI, axial view, arrow pointing to the right oculomotor nerve (cisternal portion); note proximity to overlying hippocampal gyrus (uncus), denoted by the asterisk. |
Isolated Fixed, Dilated Pupil as the Sole Manifestation of Subarachnoid Oculomotor Nerve Palsy
Many different lesions that compress the oculomotor nerve from above and medially rarely may produce isolated pupillary dilation, given that the Edinger–Westphal nuclei are draped over the superomedial aspect of each oculomotor nerve. Intracranial aneurysms, particularly those at the junction of the internal carotid artery and the posterior communication artery, are capable of producing a fixed dilated pupil in the early stages of oculomotor nerve involvement, but other signs of oculomotor nerve palsy usually develop within a few hours. Basilar artery aneurysms or basal meningitis can produce an isolated middilated nonreactive or poorly reactive pupil that may be the only sign of an oculomotor nerve palsy for days or even weeks. Hence, close follow-up (daily pupil checks within the first week) is recommended for patients that present with this isolated finding. Nonetheless, truly isolated pupillary dilation from involvement of the interpeduncular portion of the oculomotor nerve is exceptionally rare. The occurrence of a widely dilated, nonreactive pupil in an otherwise healthy patient, even a patient complaining of headache, is far more likely to be caused by either ciliary ganglion involvement (i.e., a tonic pupil) or direct pharmacologic blockade, both of which can be diagnosed easily by pharmacologic testing.
Subarachnoid Oculomotor Nerve Palsy with Pupillary Involvement
Intracranial aneurysms are the most common cause of isolated oculomotor nerve palsy with pupillary involvement, particularly when the patient has a history of sudden severe pain in or around the eye (Figs. 18.11 and 18.12). The aneurysms usually arise from the junction of the internal carotid and posterior communicating arteries; however, aneurysms located at the top of the basilar artery and aneurysms located at the junction of the basilar artery and superior cerebellar artery may produce a similar clinical picture. Such aneurysms may injure the oculomotor nerve by direct compression, from a small hemorrhage, or at
the time of a major rupture. Trauma to the oculomotor nerve may occur during aneurysm surgery.
the time of a major rupture. Trauma to the oculomotor nerve may occur during aneurysm surgery.
 Figure 18.11 Complete right oculomotor nerve palsy with involvement of the pupil. The patient also complained of severe right-sided retro-orbital pain. |
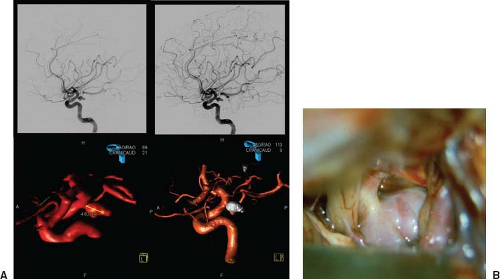 Figure 18.12 A: Top panels show selective left internal carotid arteriogram showing large aneurysm at the junction of the left internal carotid and left posterior communicating arteries and bottom left panel shows 3D MRA reconstruction of the aneurysm. Bottom left, aneurysm postendovascular coiling. (Courtesy of Dr. Carlos Torres.) B: Intraoperative photo shows compression of oculomotor nerve (red arrow) from a large posterior communicating artery aneurysm (blue oval). |
A painful oculomotor nerve palsy with pupillary involvement may result from a posteriorly draining, low-flow carotid-cavernous sinus fistula. Tumors and other compressive lesions, such as ectatic posterior cerebral or basilar artery vessels, can occasionally stretch or compress the oculomotor nerve in the interpeduncular fossa. Intrinsic lesions of the oculomotor nerve, such as schwannomas or cavernous angiomas, can also produce an acute or progressive oculomotor nerve paresis (Fig. 18.13). The presence of pain in a patient with an oculomotor palsy does not necessarily suggest a compressive lesion since ischemic injury can also produce periorbital pain. However, pain that lasts beyond 1 to 2 weeks should raise suspicion for an alternate process to microvascular ischemia. In the event that the pupil cannot be reliably assessed (surgical distortion, trauma, heavy panretinal photocoagulation), the pupil must be assumed to be involved.
 Figure 18.13 T1-weighted magnetic resonance image (axial view) in a 31-year-old woman with progressive bilateral pupillary-involved oculomotor pareses and neurofibromatosis. There are bilateral enhancing lesions in the interpeduncular cistern (arrows) consistent with schwannomas of the oculomotor nerves. |
Subarachnoid Oculomotor Nerve Palsy with Pupillary Sparing
Ischemia is the most frequent cause of pupil-sparing oculomotor nerve palsies, particularly those that are unassociated with any other neurologic signs or symptoms (Fig. 18.14). In most instances, the patient has diabetes mellitus, but systemic hypertension, atherosclerosis, and migraine can all produce a similar clinical picture. In cases of ischemic oculomotor nerve palsy, the lesion is most often located in the oculomotor nerve fascicle, where the pupillary efferent fibers
are anatomically separated from the fibers to the extraocular muscles, or in the subarachnoid portion of the nerve, where the pupillary fibers occupy a peripheral (superomedial) location and receive more collateral (pial) blood supply than the main trunk of the nerve.
are anatomically separated from the fibers to the extraocular muscles, or in the subarachnoid portion of the nerve, where the pupillary fibers occupy a peripheral (superomedial) location and receive more collateral (pial) blood supply than the main trunk of the nerve.
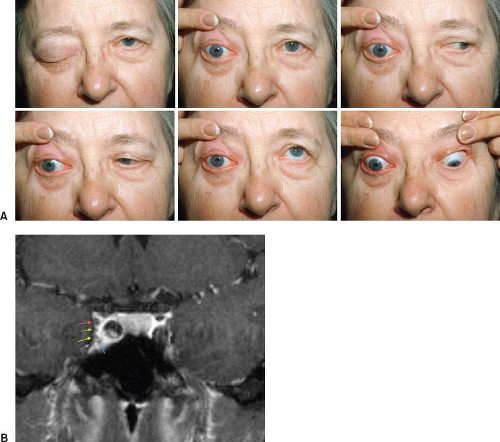 Figure 18.14 A: Patient with cavernous sinus syndrome from basal meningioma. The patient has right proptosis associated with a complete right oculomotor nerve palsy, a right abducens nerve paresis, and a right Horner syndrome. Note that the right pupil is slightly smaller than the left pupil. B: T1-gadolinium–enhanced MRI, coronal view, demonstrates the cranial nerves as they travel within the cavernous sinus. Red arrow, oculomotor nerve; green, trochlear nerve; yellow, ophthalmic division of the trigeminal; purple, maxillary division of the trigeminal; and blue, abducens nerve. |
Patients with oculomotor nerve pareses caused by ischemia often have severe pain regardless of whether or not the pupil is involved. Ischemic oculomotor nerve palsies characteristically resolve within 4 to 16 weeks without treatment. The resolution is almost always complete, and there is almost never evidence of aberrant regeneration. Around 20% of patients with ischemic oculomotor nerve palsies will present with some involvement of the pupil.
Although most pupil-sparing oculomotor nerve palsies (with or without associated pain) are caused by ischemia, such palsies may also be produced by subarachnoid compressive lesions, particularly aneurysms, ipsilateral temporal lobe astrocytomas, and ipsilateral acute subdural hematomas. It is estimated that approximately 5% of compressive oculomotor palsies are pupil sparing. Such palsies are nearly always incomplete and are often accompanied by persistent ocular or orbital pain. Patients with a painful, incomplete, pupil-sparing oculomotor nerve paresis should undergo MRI as well as either computed tomographic angiography (CTA) or MR angiography (MRA). Depending on the results of these studies, conventional angiography may be appropriate, although very rarely performed at this point for diagnostic purposes given the perpetual advances in imaging resolution and techniques (see Table 18.2).
Subarachnoid Oculomotor Nerve Palsy from Involvement at or near its Entrance to the Cavernous Sinus
The oculomotor nerve is particularly vulnerable to stretch and contusion injuries where it is firmly attached to the dura adjacent to the posterior clinoid process just posterior to the cavernous sinus. Frontal head trauma, aneurysms, and surgery in the parasellar region are the common causes of injury at this site.
Herniation of the hippocampal gyrus (uncus) compresses the oculomotor nerve where it passes over the
ridge of the dura associated with the attachment of the free edge of the tentorium to the clivus. As the herniating hippocampal gyrus descends into the tentorial incisura, it presses upon the upper surface of the ipsilateral oculomotor nerve that is running beneath it (see Fig. 18.10D) and pulls the oculomotor nerve more firmly into contact with the posterior clinoid process. The herniating cerebral mass ultimately reaches and impinges on the dorsal surface of the pons on the same side. The posterior cerebral arteries are also drawn tightly down across the dorsal surface of the oculomotor nerves, producing even more compression (see Fig. 18.10A). Pupillary dilation is often the first sign of increasing cerebral edema or of an ipsilateral, expanding, supratentorial mass. This initial pupillary sign is caused by pressure on the peripheral portion of the nerve. With increasing compression, additional signs of impaired oculomotor nerve function appear.
ridge of the dura associated with the attachment of the free edge of the tentorium to the clivus. As the herniating hippocampal gyrus descends into the tentorial incisura, it presses upon the upper surface of the ipsilateral oculomotor nerve that is running beneath it (see Fig. 18.10D) and pulls the oculomotor nerve more firmly into contact with the posterior clinoid process. The herniating cerebral mass ultimately reaches and impinges on the dorsal surface of the pons on the same side. The posterior cerebral arteries are also drawn tightly down across the dorsal surface of the oculomotor nerves, producing even more compression (see Fig. 18.10A). Pupillary dilation is often the first sign of increasing cerebral edema or of an ipsilateral, expanding, supratentorial mass. This initial pupillary sign is caused by pressure on the peripheral portion of the nerve. With increasing compression, additional signs of impaired oculomotor nerve function appear.
Table 18.2 Evaluation of Oculomotor Palsies/Risk of Compressive Lesion | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|



