and Charles P. Molumi2
(1)
University of Papua New Guinea and Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
(2)
Port Moresby General Hospital, Boroko, National Capital District, Papua New Guinea
1.1 Sublabial Approach for Maxillary Cyst
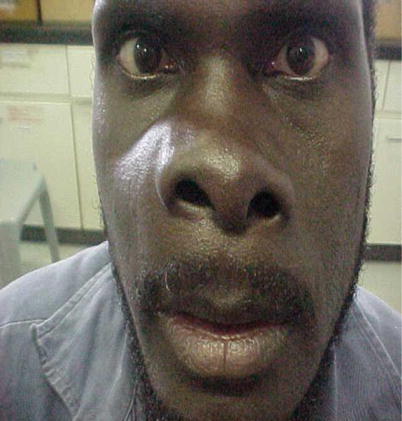
Fig. 1.1
Right nasolabial swelling due to cyst in the maxillary sinus
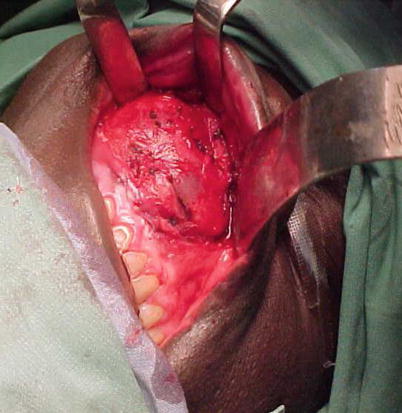
Fig. 1.2
The incision begins 0.5 cm above the junction of the gingivolabial sulcus mucosa. It extends from the canine to the first molar tooth. The incision is made bone deep. The superior mucosal flap is raised preserving the neurovascular bundle in the infraorbital foramen

Fig. 1.3
A small gouge is placed at the canine fossa and hammered till the maxillary sinus antrum is entered taking care not to damage the root of the tooth. The opening is enlarged by nibbling the bone edges with a Kerrison rongeurs till adequate exposure is attained. In cases where the bone is thinned out by the tumor, this might not be necessary
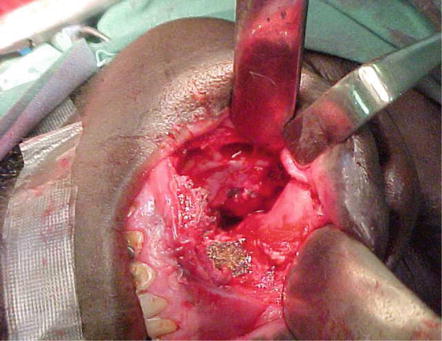
Fig. 1.4
The tumor is removed and the cavity is packed with an acroflavin pack. An inferior meatus antrostomy is made. The end of the pack is kept in the nasal cavity and removed on the third post operative day. The sublabial incision is closed in layers
1.2 Midfacial Degloving

Fig. 1.5
After oral intubation, patient is placed in head extended position. The nasal vestibular hairs are trimmed off and the nose is prepared with cophenylcaine spray and lignocaine with adrenaline infiltration. Bilateral tarsorrhaphies are done. A columella clamp is used to retract the columella. A total transfixation incision is marked out on each side at the junction between the stratified squamous and respiratory columnar epithelium

Fig. 1.6
The transfixation incision is extended from the tip of the nose onto the nasal floor

Fig. 1.7
A sublabial incision is made from the first molar of the ipsilateral side to first molar of the contralateral side. The incision is deepened to the periosteum of the canine fossa
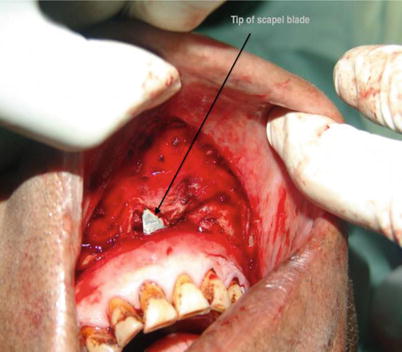
Fig. 1.8
The nasal vestibule is released circumferentially by a through and through incision made down through the periosteum of the pyriform margin and the nasal floor
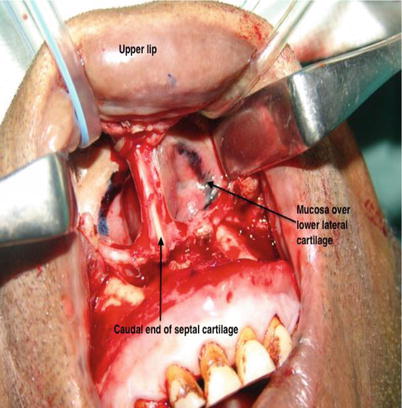
Fig. 1.9
Through the sublabial incision, the upper lip and the columella are elevated exposing the anterior end of the septal cartilage and marking over the lower lateral cartilage at the junction between the stratified squamous and columnar epithelium for the intercartilagenous incision
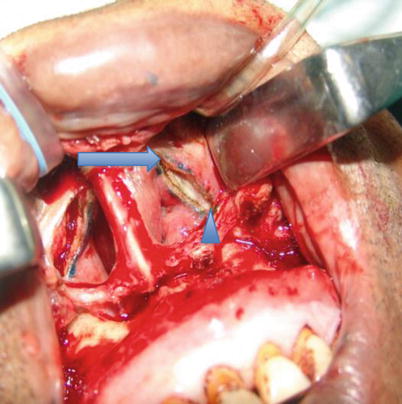
Fig. 1.10
An intercartilagenous incision is made to join the superior end of the transfixation incision medially (joining to the septal incision) (arrow) and the nasal floor laterally (arrow head)
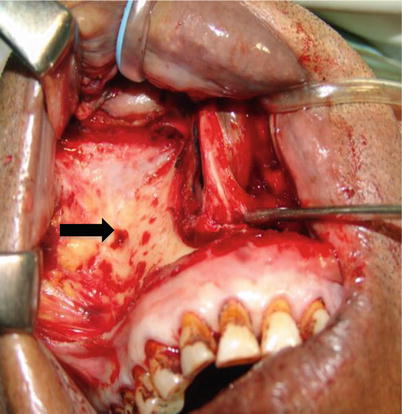
Fig. 1.11
Dissection is continued through the intercartilagenous incision exposing the dorsum of the upper lateral cartilage and then to the nasal bones. The periosteum is incised with a curved Joseph knife, and the soft tissue is separated from the nasal bones. The elevation is continued laterally to the nasomaxillary suture line and superiorly to the glabella. Soft tissue over the anterior maxilla is elevated with a periosteal elevator in the subperiosteal plane to the zygoma and the infraorbital rim. The neurovascular bundle in the infraorbital foramen (arrow) is carefully preserved
1.3 Lateral Rhinotomy with Medial Maxillotomy

Fig. 1.12
Moure’s incision begins below the medial aspect of the eyebrow and curves downwards and forwards to the medial canthus. The incision extends to the nasofacial junction and along the nasal alar rim ending within the nostrilla

Fig. 1.13
The incision is carried to the bone. The angular vessels are coagulated

Fig. 1.14
The periosteum is elevated from the lateral nasal wall and the anterior wall of the maxilla preserving the infraorbital foramen with its neurovascular bundle. The periosteum over the inferior orbital margin is elevated. The lacrimal sac can be divided. The frontoethmoidal suture is identified

Fig. 1.15
The nasal alar is mobilized by carrying the Moure’s incision through the entire thickness along the pyriform aperture
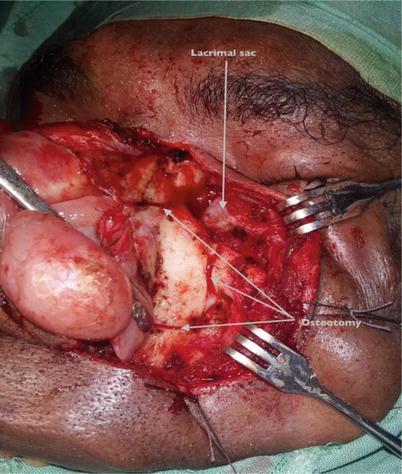
Fig. 1.16
The periosteum is elevated from the lateral nasal wall and the anterior wall of the antrum preserving the infraorbital foramen with its neurovascular bundle. The periosteum over the inferior orbital margin is elevated. The frontoethmoidal suture is identified and osteotomy done obliquely along the nasomaxillary suture line, vertically medial to the infraorbital foramen and horizontally above the level of the dental roots and the pyriform aperture
Fig. 1.17
The bone (medial wall of maxilla) is removed and preserved in saline for reinsertion later. The lacrimal sac and duct is mobilized from their bony bed and retracted laterally. The maxillary sinus is inspected
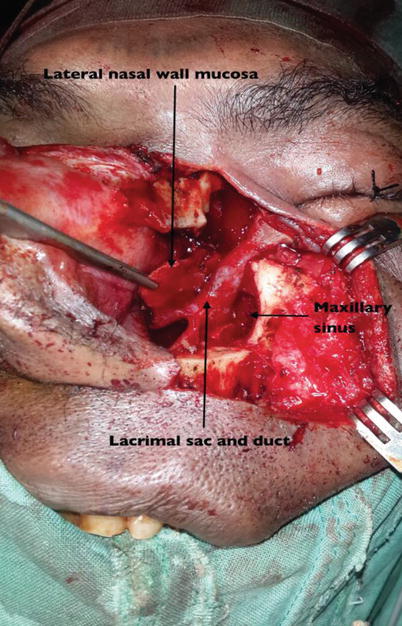
Fig. 1.18
The tumor is removed accordingly
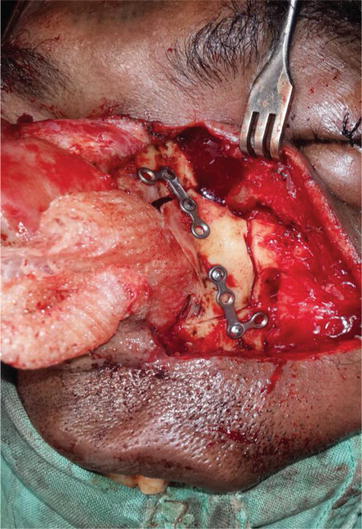
Fig. 1.19
After hemostasis the nasal cavity is packed with gauze and the bone placed back and fixed with miniplate and screws

Fig. 1.20
The nasal alar is returned and the skin closed with interrupted sutures
1.4 Transpalatal Approach by Palatal Osteomucoperiosteal Flap

Fig. 1.21
A 5 cm gingivolabial sulcus incision is made equally on either side of the midline. The incision is made bone deep and the nasal mucoperioseal floor is elevated from the pyriform aperture to the posterior end of the hard palate and side to side as much as possible. With a heavy scissor, the junction of the maxillary crest and septum is cut all the way from its anterior end to the posterior end. A space is created between the bony and soft tissues of the nasal floor where a malleable copper retractor is placed. This is done to prevent injury to the nasal floor mucoperiosteum during subsequent osteotomy of the hard palate

Fig. 1.22
A incision is made on the hard palate from the last molar tooth of the pathological side to the junction between the contralateral canine and first premolar tooth. It is made where the palatal mucoperiosteum meet the tooth. The palatal mucoperiosteum is elevated just medial to the greater palatine canal posteriorly and posterior to the incisive foramen anteriorly. The greater and lesser palaltine arteries are coagulated to reduce bleeding
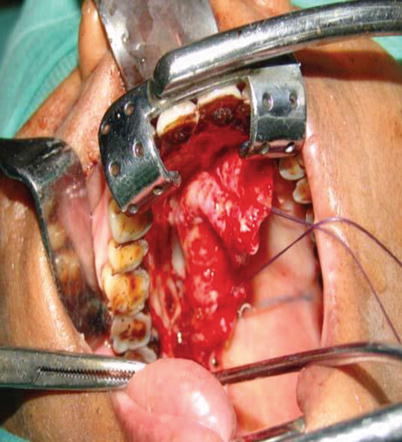
Fig. 1.23
On the side of the lesion a inverted ‘J’ shaped cut is made on the bony hard palate. The side arms of the inverted ‘J’ is placed at the junction of the horizontal and vertical part of the hard palate. The summit of the inverted ‘J’ is located almost 2 cm posterior to the base of the central incisor tooth. By this way, the very thick palatal bone is avoided. The cut is made just medial to the greater palatine canal using a mastoid drill with a small cutting burr. The cut is made through and through the bony nasal floor

Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


