Although the preponderance of cerebellopontine angle lesions are schwannomas, focused attention to patient clinical history, imaging studies, and tissue biopsies when indicated will aid in detection of less common lesions that might otherwise be misdiagnosed. This is most critical for pathologies that dictate different management paradigms be undertaken.
Key points
- •
Vestibular schwannoma (VS), meningioma, epidermoid, and lipoma account for 95% of cerebellopontine angle (CPA) lesions.
- •
There is wide differential of rarer lesions of the CPA, including benign and malignant lesions.
- •
Many of these lesions may mimic schwannomas except for subtle imaging findings underlying the importance of their careful review.
- •
Management of CPA pathology may include single- or multimodality treatment, including observation, microsurgical resection, and stereotactic radiation therapy.
| CPA | Cerebellopontine angle |
| CSF | Cerebrospinal fluid |
| ELST | Endolymphatic sac tumor |
| VHL | von Hippel-Landau |
| VS | Vestibular schwannoma |
Introduction
Fewer than 10% of intracranial neoplasms involve the CPA in adults although this number is less than 1% in children. Although VSs are the most common lesion of the CPA (70%–90%), other pathology may present in this location. Meningiomas are the second most common lesion, occurring between 5% and 15% of cases, followed by epidermoids and lipomas. A wide differential of rarer lesions compose the remainder, some of which develop directly in the CPA, whereas others may extend from neighboring structures. Diagnosis may be made from the clinical history as well as radiologic features ( Table 1 ).
| Tumor Type | Radiographic Characteristics |
|---|---|
| VSs, hemangioblastoma | T1 iso/hypointense, T2 isointense, enhance with contrast (vascular flow voids for hemangioblastoma) |
| Meningioma, hemangiopericytomas | Uniformly enhancing, broad petrous base, hyperostosis of underlying bone, possible calcifications |
| Epidermoid | CSF-like intensity on CT and MRI T1, T2 sequences demonstrate restriction on diffusion sequences |
| Lipomas | Hyperintense on T1, do not enhance, lose their signal on fat-suppression sequences |
| ELSTs | T1 hyperintense, heterogenous enhancement with contrast |
| Glomus tumors/parangangliomas | T1 hypointense, T2 hyperintense, enhance with gadolinium |
| Arachnoid cyst, granulation | CSF-like intensity on CT and all MRI sequences, may erode bone |
Introduction
Fewer than 10% of intracranial neoplasms involve the CPA in adults although this number is less than 1% in children. Although VSs are the most common lesion of the CPA (70%–90%), other pathology may present in this location. Meningiomas are the second most common lesion, occurring between 5% and 15% of cases, followed by epidermoids and lipomas. A wide differential of rarer lesions compose the remainder, some of which develop directly in the CPA, whereas others may extend from neighboring structures. Diagnosis may be made from the clinical history as well as radiologic features ( Table 1 ).
| Tumor Type | Radiographic Characteristics |
|---|---|
| VSs, hemangioblastoma | T1 iso/hypointense, T2 isointense, enhance with contrast (vascular flow voids for hemangioblastoma) |
| Meningioma, hemangiopericytomas | Uniformly enhancing, broad petrous base, hyperostosis of underlying bone, possible calcifications |
| Epidermoid | CSF-like intensity on CT and MRI T1, T2 sequences demonstrate restriction on diffusion sequences |
| Lipomas | Hyperintense on T1, do not enhance, lose their signal on fat-suppression sequences |
| ELSTs | T1 hyperintense, heterogenous enhancement with contrast |
| Glomus tumors/parangangliomas | T1 hypointense, T2 hyperintense, enhance with gadolinium |
| Arachnoid cyst, granulation | CSF-like intensity on CT and all MRI sequences, may erode bone |
Nonschwannomatous lesions of cerebellopontine angle
Meningioma
Meningiomas, which develop from arachnoid cap cells in the dura, are the second most common tumor in the CPA, comprising approximately 10% of lesions in this location. Of all locations, approximately 10% of meningiomas are found in the CPA. These can have origins in the dura around the internal auditory canal, Meckel cave, jugular foramen, jugular tubercle, suprameatal tubercle, sigmoid sinus, torcula, the superior or inferior petrosal sinuses, porus acusticus, and clivus although most commonly they originate from the posterior petrous dura. They tend to be benign tumors that displace local structures at the tumor’s periphery as opposed to infiltrating, although they may be adherent. There is a female predominance in CPA meningiomas, as there is with those in other locations.
As opposed to the presentation of VSs, audiovestibular symptoms (hearing loss, tinnitus, and dysequilibrium) are less frequent and of shorter duration with cerebellopontine meningiomas. Nevertheless, audiovestibular symptoms predominate. Facial pain, which is rarely seen in VS patients, can present in up to 30% of cerebellopontine meningiomas. Dysesthesias and facial spasms can be presenting signs as well. Cerebellar signs are frequently seen in these meningiomas compared with VSs, in which they are rare.
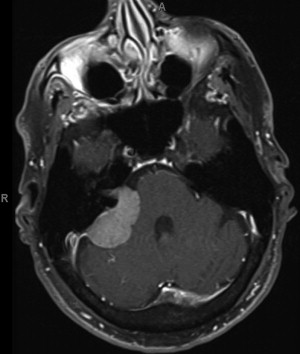
Radiologic diagnosis of cerebellopontine meningioma is made typically with gadolinium-enhanced MRI of the brain. They are uniformly enhancing, hemispheric, semilunar masses with a broad petrous base to which they are attached they are usually asymmetric to the internal auditory canal. Classically, an enhancing dural tail can be appreciated at the tumor’s margin ( Fig. 1 ). On CT, potential calcifications or hyperostosis of the surrounding bone can be appreciated. Sometimes it may be hard to differentiate between meningiomas and schwannomas in the CPA. One study has shown 94% sensitivity and 100% specificity differentiating meningiomas from VSs based on lack of microhemorrhages on T2-weighted gradient echo.
Treatment of meningiomas depends on the symptomatology and goals of treatment. An asymptomatic meningioma can be followed with serial MRI scans to assess for growth. Serial scanning and observation may also be used in patients with advanced age or comorbidities that preclude surgery. In these cases, stereotactic radiosurgery may also be considered. If surgical resection is planned, the goal is maximum safe removal of the tumor, avoiding injury to involved cranial nerves, with wide excision of the dural attachment as well as resection of hyperostotic bone, which can contain infiltrative tumor.
As with VSs, the surgical approaches for these tumors include the retrosigmoid, translabyrinthine, and middle fossa craniotomies. The most common approach used is the retrosigmoid, which offers access to the CPA when hearing preservation is attempted. The translabyrinthine approach is another viable option, with an advantage of less cerebellar retraction during surgery but inevitably sacrifices any residual hearing. This approach may be used in patients with tumors that fill the entire internal acoustic meatus or patients in whom hearing is already poor or not salvageable. The middle fossa approach is generally not useful because it is not appropriate in tumors that extend more than 1 cm out of the internal acoustic meatus. A subtemporal/transpetrosal approach has also been used. It facilitates exposure particularly for meningiomas that extend either anterior or superior to the interior auditory meatus, along the petroclival region. Advantages with this approach include early devascularization of the tumor, small amounts of brain retraction, preservation of the vein of Labbé, and access to both supra- and infratentorial compartments. Combined approaches also may be advantageous depending on tumor location.
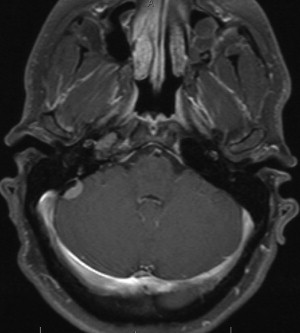
Posterior fossa meningiomas adjacent to the endolymphatic duct may present with a specific symptom complex of vertigo, sensorineural hearing loss, tinnitus, and aural fullness ( Fig. 2 ). Such patients may be misdiagnosed as having Meniere’s disease. The authors have previously described management of these particular lesions. Surgical resection via a retrolabyrinthine or retrosigmoid craniotomy may result in successful preservation of hearing and improvement in vestibular symptoms ( [CR] ).
Outcomes from surgical resection of meningiomas vary depending on tumor location and size. In recent series, gross total resections were achieved in 45% to 86%. Mortality ranged between 0% and 5%. Permanent post operative facial weakness occurred in 6% to 11% with as many as 30% having postoperative facial paresis. Swallowing problems occurred in 2% to 12%. Hearing declined in 17% of patients in hearing preservation surgeries, although 1 large study found 91% of functional hearing preservation in their series.
Stereotactic radiosurgery may be used for cerebellopontine meningiomas, either primary or adjuvant treatment. Good long-term control and a low side-effect profile has been demonstrated. One study examined radiosurgery in CPA meningiomas, specifically. It showed 95% progression-free survival at 5 years, with 31% of patients showing improvement of their symptoms 58% having no change, and 11% with worsening. Of the 74 patients studied, 7 (9%) had symptomatic adverse radiation effects. There was no association between decrease in tumor volume and symptomatic improvement. Trigeminal neuralgia was the most common new symptom after radiosurgery. In another report from the same center, the investigators found that trigeminal neuralgia tended to persist after radiosurgery in petroclival meningiomas despite effective tumor control. In a study by Park and colleagues, measurable hearing was achieved in 99% of patients, and 97% of patients with serviceable hearing preprocedurally had stable or improved hearing after radiosurgery. Unlike in treatment of VSs, no statistical relationship was found between hearing outcomes and radiation dose to the cochlea in stereotactic radiosurgery of meningiomas. A recent multicenter collaboration confirmed this, showing a 93% 5-year progression-free survival and 9% symptomatic neurologic deterioration. This study calculated a 10-year progression-free survival, of 77%.
Epidermoid
Epidermoids are the next most common CPA lesion and represent approximately 6% of such lesions and 1% or all intracranial tumors. In this location they are thought to develop from sequestered epithelial cell rests from the laterally migrating secondary optic and otic capsules or from developing embryonic neurovasculature. They grow slowly through accumulation of keratin and cholesterol from their squamous epithelial lining. Their peak age of occurrence is 40 with no gender predilection. They tend to spread along normal cleavage planes and surround, not displace, cranial nerves and blood vessels. They are benign lesions, although malignant transformation has been reported.
Length of symptoms in cerebellopontine epidermoids tends to be longer than in other tumors of the same area but can present with as wide a variety of posterior fossa dysfunction. Unique to epidermoids, patients can present with recurrent bouts of aseptic meningitis from inflammation induced by keratin debris. On CT scan, these lesions appear almost isodense to spinal fluid with characteristic irregular margins. The signal intensity of these cysts is slightly higher than cerebrospinal fluid (CSF) on T1- and T2-weighted MRI ( Fig. 3 ). Diffusion-weighted image sequences differentiate the epidermoid cyst from spinal fluid based on the restricted diffusion signal in the cyst.
Asymptomatic lesions can be followed, but the only definitive treatment of these lesions is gross total resection of the tumor and its capsule, the part of the tumor responsible for its growth. Safe removal of the capsule may be difficult because it can be firmly adherent to the neurovascular structures in the posterior fossa and consequently recurrence is common. Attempts are made to minimize morbidity from cranial nerve dysfunction and in some cases plan to perform serial resections if residual tumor progresses. Retrosigmoid craniotomy serves as the most common surgical approach, although combined approaches, including a subtemporal and transpetrosal approach, may sometimes be used because these tumors may have supratentorial extension ( [CR] ).
A recent study reports rates of gross total resection of such lesions range from 33% to 88%. In several larger studies in that time period, rates of tumor recurrence have ranged from 7% to 45%. Clinical improvements have been seen in 50% to 100% of the patients. Much as in other surgeries of the CPA, removal of these tumor has risks of facial weakness (0%–23%), worsening of hearing (8%–10%), and swallowing problems (0%–10%). The resection of epidermoids carries a 3% to 8% risk of aseptic meningitis and 0% to 4% of shunted hydrocephalus.
Arachnoid Cyst
Arachnoid cysts compose 1% of all tumors and less than 1% of CPA tumors. Only 7% of all arachnoid cysts are in the CPA and only 15% of which become symptomatic. There is a male predominance overall, but there is a female predominance in cerebellopontine cysts.
These are presumably congenital malformations of the arachnoid and are histologically characterized by a cyst wall made of arachnoid or ependyma and a cystic space filled with CSF or xanthochromic fluid. Their cause is unknown. On CT and MRI they appear almost identical in signal to spinal fluid. They have smooth and rounded edges, displace neurovascular structures, and erode adjacent bony structures. In the CPA they can present with brainstem and cerebellar compression, cranial nerve dysfunction (most commonly CN VIII), mass effect in the posterior fossa resulting in suboccipital headache, tonsillar descent, and syringomyelia. Only 2% of arachnoid cysts have been found to grow. Occasionally, so-called giant arachnoid granulations may be seen as in Fig. 4 . These too do not enhance with contrast and are T1 isointense.



