The unique and specialized structures of the oral cavity and jaws give rise to a myriad of diverse developmental, inflammatory, and benign lesions or conditions. This article reviews the imaging of common lesions and their variants, and reviews several rare but important lesions. Guidelines and algorithms for approaching the differential diagnosis are provided.
It is important to distinguish the oral cavity from surrounding spaces and the oropharynx, as the presence of specialized hard and soft tissue structures gives rise to different disease processes within the oral cavity than in the oropharynx. The oral cavity lies anterior to the oropharynx and is separated from the oropharynx by the soft palate, tonsillar pillars, and at the tongue, the circumvallate papillae. Thus the oral tongue lies within the oral cavity, while the tongue base lies within the oropharynx. The oral cavity contains the hard palate, alveolar processes of the maxilla and mandible, dentition, oral tongue, buccal vestibule, and lips. Within or bounding the oral cavity are three spaces formed by superficial layers of deep cervical fascia, mucosal surfaces, or muscle boundaries. These are the sublingual and submandibular spaces inferiorly and the buccal spaces laterally.
The sublingual space (SLS) is formed by the genioglossus and geniohyoid muscles medially and the mylohyoid muscle laterally and inferiorly ( Fig. 1 A,B). Anteriorly, the SLS is bounded by the lingual cortex of the mandible. On its posterior boundary, the SLS is contiguous with the submandibular space (SMS) and the parapharyngeal space. These anatomical relationships are critical to understanding the spread of infectious or neoplastic processes, in particular, because the SLS is one of the spaces in the head and neck not encapsulated by fascia. The SLS contains fat, the sublingual glands and ducts, the deep or uncinate portion of the submandibular gland and the submandibular duct (Wharton’s duct), the anterior margin of the hyoglossus muscle, the sublingual artery, the lingual nerve and artery, and distal branches of the glossopharyngeal and hypoglossal nerves. It is further important to recognize that the SLS is a continuous space anteriorly, ventral to the frenulum, permitting access across the midline.
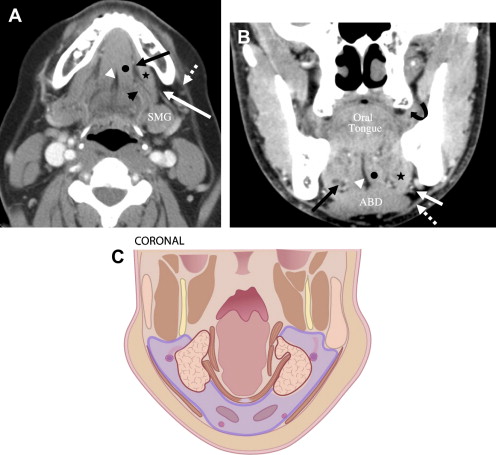
The SMS ( Fig. 1 A–C) is a horseshoe-shaped space that lies laterally, inferiorly, and posteriorly to the SLS, inferior to the mylohyoid and superior to the hyoid bone. It is formed by superficial layers of deep cervical fascia that split to envelope the space with the superficial layer of fascia extending along the medial margin of the platysma muscle and the deep layer extending along the lateral margin of the mylohyoid. The SMS contains fat, the superficial portion of the submandibular gland and proximal portions of Wharton’s duct, submental and submandibular lymph nodes (level 1A and B), the facial artery and vein, the inferior loop of the hypoglossal nerve, and the anterior belly of the digastric muscle. The SMS is continuously inferior to the mylohyoid muscle, thereby permitting midline transgression. The SMS is also contiguous on its posterior boundary with the SLS and with the parapharyngeal space.
The oral tongue volumetrically constitutes the predominant organ of the oral cavity and is composed of the three orthogonally oriented intrinsic tongue muscles (verticalis, longitudinalis, and transversus), and the extrinsic muscles: genioglossus, hyoglossus, styloglossus, and palatoglossus. The root of the tongue (see Fig. 1 A, B) is formed by the genioglossus and geniohyoid muscles and the lingual septum. Inferiorly, the root of the tongue extends to the mylohyoid sling and anteriorly extends to the genial tubercles at the lingual mandibular symphysis.
Anatomical variants
The most common anatomical variants of clinical importance in the oral cavity arise from accessory or ectopic glandular tissue.
Accessory salivary tissue
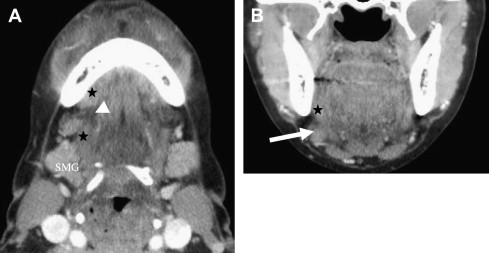
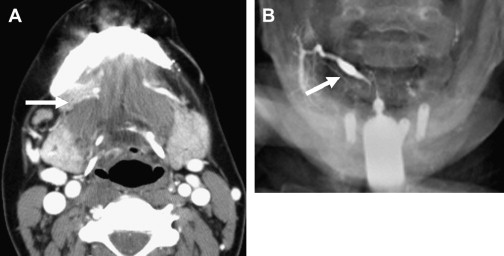
Accessory salivary tissue arises from development of extra submandibular gland tissue. Accessory salivary tissue is composed of normal submandibular salivary gland tissue (mixed mucinous and serous), and it is found in the SMS inferior to the mylohyoid muscle and anterior to the submandibular gland ( Fig. 2 ). On imaging, this soft tissue mass in the SMS will have the same imaging appearance and contrast enhancement as the submandibular glands. On CT imaging it will appear as a homogenous or mildly heterogenous mass with the same density as the submandibular gland. On MRI it will follow the signal intensity of the submandibular glands on all sequences. Accessory salivary tissue is a normally functioning salivary gland, and as such, it may demonstrate ductal supply from branches off of the proximal or distal segments of Wharton’s duct ( Fig. 3 ). Accessory salivary gland tissue ranges in size from several millimeters up to 2 cm, and may, on occasion, attain the size of a normal submandibular gland. In this scenario, it is important to determine whether the submandibular glands are present to distinguish this normal variant from transposed submandibular glands used as a radiation treatment procedure for beam sparing of the glands .
Lingual thyroid
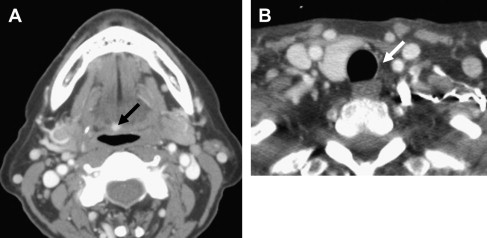
Lingual thyroid is ectopic thyroid found in the tongue or tongue base. This arises because of failure of the thyroid anlage to descend during development from the foramen cecum along the thyroglossal duct tract to its final position in the visceral space of the anterior neck. On CT imaging, lingual thyroid will present as high-density or hyperdense soft tissue mass in the midline intrinsic muscles of the tongue or base of tongue, and which, following contrast, avidly and homogeneously enhances ( Fig. 4 ). On MRI, a lingual thyroid will appear as a hyperintense mass on T1 and T2 weighted images and will demonstrate considerable homogeneous enhancement. An important caveat to recognize is that these ectopic foci may consist of functioning thyroid and as such are susceptible to disease processes of the thyroid, including goiter or neoplasms. Moreover, because approximately 25% to 75% of patients presenting with lingual thyroid will have either only partial thyroid tissue in the cervical neck or a complete absence of thyroid, it is imperative to ascertain the presence of functioning thyroid before surgical extirpation of the tongue mass. This is accomplished through visual search on contrast-enhanced CT or MRI studies and radionuclide iodine-123 to identify uptake in the lingual thyroid and any other cervical thyroid tissue .