CT and MRI are the two most widely used imaging modalities for evaluating head and neck pathology. There is continued controversy in the literature about which modality is superior for imaging different areas of the head and neck. This article summarizes the literature supporting the use of CT, MRI, or both for specific clinical scenarios in otolaryngology. Familiarity with the benefits and potential pitfalls of each modality allows referring physicians and radiologists to tailor imaging regimens to the needs of individual patients.
CT and MRI are the two most widely used imaging modalities for evaluating head and neck pathology. Although certain clinical scenarios are undeniably better imaged with one modality versus the other, there are many situations in which controversy arises regarding the best modality to employ. The advantage of MRI is that it provides superior soft tissue contrast resolution, whereas CT offers excellent bony detail. Although MRI does not require the use of ionizing radiation, it is more expensive and less readily available than CT. Deciding on which modality to employ can be confusing in clinical practice. Several disease entities, such as those affecting the skull base, often require a combination of CT and MRI to fully delineate the type and extent of pathology. Advances in combined modality imaging, such as positron emission tomography (PET)/CT and PET/MR, offer further meaningful information but can also complicate diagnostic decision-making in various head and neck disease states. This article summarizes the literature supporting the use of CT, MRI, or both for specific clinical scenarios in otolaryngology.
Mandibular invasion in oral cancer
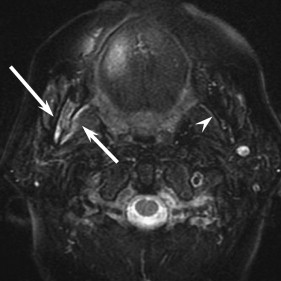
Cross-sectional imaging has a crucial role in the work-up and staging of patients with carcinomas of the oral cavity and oropharynx. Although MRI is generally considered the modality of choice to delineate the extent of the primary tumor, controversy remains regarding which imaging modality is ideal in detecting mandibular invasion . The decision to evaluate for mandibular invasion with CT or MRI is often made on a case-by-case basis. MRI affords higher sensitivity at the expense of lower specificity ( Fig. 1 ) . MRI will overcall tumor invasion when none is present (false positives), whereas CT may overlook subtle invasion (false negatives). The lower specificity of MRI has been attributed to false-positive findings in patients with infectious/inflammatory odontogenic disease, recent dental extractions, or osteoradionecrosis . Assessing the integrity of the normal hypointense cortical line on T1-weighted MR images (which is one of the criteria in determining mandibular invasion on MRI) can also be problematic due to chemical shift artifact by bone marrow fat. This potential pitfall can further decrease the specificity of MRI . Only one study has convincingly reported a high sensitivity and specificity with respect to the diagnostic accuracy of MRI in detecting mandibular invasion (93% and 93%, respectively) .
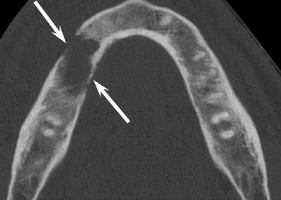
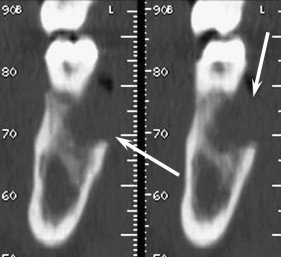
An optimal scanning technique is critical to ensure accuracy with CT ( Fig. 2 ). Early studies that employed 5-mm thick axial sections without bone algorithm reconstructions showed poor sensitivity and specificity. Contemporary CT imaging (3-mm thick axial bone algorithm images) can improve sensitivity and specificity (96% sensitivity, 86% specificity) , and high-resolution scanning with multidetector CT is expected to have even better results. The underused DentaScan (Milwaukee, Wisconsin) has also been shown to improve the sensitivity of CT in assessing mandibular invasion (95% sensitivity) . DentaScan CT software incorporates thin axial sections that can be reformatted into panelliptical and parasagittal views, allowing optimal visualization of the buccal and lingual mandibular cortices. The panelliptical view is a curved reformat along the jaw reminiscent of orthopantomograms. The parasagittal views are aligned perpendicular to the curvature of the mandible ( Fig. 3 ).
Although CT offers lower cost and easy availability, MRI is better at delineating the soft tissue extent of the primary tumor. Often, the decision of whether to image the mandible with CT or MRI is made on a case-by-case basis; however, a rational approach is to begin with MRI to assess the extent of soft tissue involvement in addition to mandibular invasion. Given the high sensitivity and high negative predictive value for assessing mandibular invasion, a negative MR examination might obviate the need for further imaging with CT. Conversely, given the potential false-positive findings on MRI, a positive MRI result that is not definitive or that contradicts the findings on physical examination may warrant a second look with high-quality CT.
Although assessment for bone marrow invasion can be accomplished with MRI or CT, referring physicians should be aware that MRI is prone to false positives and CT to false negatives.
Cartilage invasion in laryngeal cancer
As is true for carcinoma of the oral cavity and oropharynx, cross-sectional imaging has a crucial role in staging laryngeal cancer. Recent advances in CT technology have allowed for optimal evaluation of laryngeal pathology with the use of thin section multidetector computed tomography (MDCT) with coronal and sagittal reconstructions. Multiplanar imaging was once an exclusive strength of MRI, but MDCT now offers similar capabilities, as described in the article by Dr. Glastonbury, elsewhere in this issue. The decision to use CT or MRI in the staging of laryngeal carcinoma often depends on institutional preference. Although the prognostic significance of laryngeal cartilage invasion is well established, how to assess this critical finding is still debated .
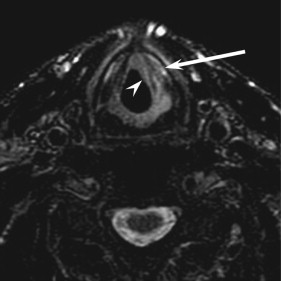
Numerous European researchers have investigated the issue regarding optimal imaging for laryngeal cartilage invasion . These studies support the notion that MRI is more sensitive than CT for the detection of neoplastic infiltration of the laryngeal cartilage; however, the increased sensitivity of MRI comes at the expense of decreased specificity, similar to the evaluation of mandibular invasion discussed previously ( Fig. 4 ). The high negative predictive value of MRI could potentially obviate the need for further imaging with CT. Given the relatively low specificity of MRI, a positive MR scan might provoke a second look with CT, potentially offering the patient a more conservative laryngeal surgery ( Fig. 5 ). Because MRI has been recommended by many investigators as the modality of choice for imaging the primary laryngeal tumor, valuable information can be ascertained regarding laryngeal cartilage invasion while assessing the extent of the primary. A recent study suggested that assessment of T2-weighted signal intensity on MR images may be useful in determining the outcome of primary radiotherapy in glottic carcinoma . This situation is similar to imaging of oral cavity tumors. A recent study in the otolaryngology literature demonstrated considerable interobserver variation in assessing cartilage invasion and sclerosis based purely on CT . CT may also fail to detect early cartilage invasion due to inherent variability in ossification patterns in the laryngeal cartilage, in particular, the thyroid cartilage ( Fig. 6 ) ; however, CT offers a shorter scan time which can limit motion artifact, often the bane of MRI in these patients, who often have co-existent medical conditions. Some researchers believe that MRI can accurately distinguish between true tumor invasion of cartilage and reactive cartilage edema, but these results await confirmation in large trials . In select situations, a combination approach with both CT and MRI will more confidently allow the radiologist to predict cartilage invasion.


Although MRI is usually presumed to be better at staging laryngeal carcinomas, no studies have convincingly shown a benefit of MRI over CT; therefore, institutional preferences dominate this imaging decision. As in the setting of mandibular invasion, MRI has better sensitivity, but CT has better specificity for the assessment of cartilage invasion.
Cartilage invasion in laryngeal cancer
As is true for carcinoma of the oral cavity and oropharynx, cross-sectional imaging has a crucial role in staging laryngeal cancer. Recent advances in CT technology have allowed for optimal evaluation of laryngeal pathology with the use of thin section multidetector computed tomography (MDCT) with coronal and sagittal reconstructions. Multiplanar imaging was once an exclusive strength of MRI, but MDCT now offers similar capabilities, as described in the article by Dr. Glastonbury, elsewhere in this issue. The decision to use CT or MRI in the staging of laryngeal carcinoma often depends on institutional preference. Although the prognostic significance of laryngeal cartilage invasion is well established, how to assess this critical finding is still debated .
Numerous European researchers have investigated the issue regarding optimal imaging for laryngeal cartilage invasion . These studies support the notion that MRI is more sensitive than CT for the detection of neoplastic infiltration of the laryngeal cartilage; however, the increased sensitivity of MRI comes at the expense of decreased specificity, similar to the evaluation of mandibular invasion discussed previously ( Fig. 4 ). The high negative predictive value of MRI could potentially obviate the need for further imaging with CT. Given the relatively low specificity of MRI, a positive MR scan might provoke a second look with CT, potentially offering the patient a more conservative laryngeal surgery ( Fig. 5 ). Because MRI has been recommended by many investigators as the modality of choice for imaging the primary laryngeal tumor, valuable information can be ascertained regarding laryngeal cartilage invasion while assessing the extent of the primary. A recent study suggested that assessment of T2-weighted signal intensity on MR images may be useful in determining the outcome of primary radiotherapy in glottic carcinoma . This situation is similar to imaging of oral cavity tumors. A recent study in the otolaryngology literature demonstrated considerable interobserver variation in assessing cartilage invasion and sclerosis based purely on CT . CT may also fail to detect early cartilage invasion due to inherent variability in ossification patterns in the laryngeal cartilage, in particular, the thyroid cartilage ( Fig. 6 ) ; however, CT offers a shorter scan time which can limit motion artifact, often the bane of MRI in these patients, who often have co-existent medical conditions. Some researchers believe that MRI can accurately distinguish between true tumor invasion of cartilage and reactive cartilage edema, but these results await confirmation in large trials . In select situations, a combination approach with both CT and MRI will more confidently allow the radiologist to predict cartilage invasion.
Although MRI is usually presumed to be better at staging laryngeal carcinomas, no studies have convincingly shown a benefit of MRI over CT; therefore, institutional preferences dominate this imaging decision. As in the setting of mandibular invasion, MRI has better sensitivity, but CT has better specificity for the assessment of cartilage invasion.
Mixed hearing loss
Hearing loss presents in one of three forms: sensorineural (SNHL), conductive (CHL), and mixed (MHL). The best imaging study in the work-up of hearing loss is dictated by a combination of patient age and type of hearing loss . Isolated SNHL is typically imaged with contrast-enhanced MRI of the internal auditory canals, whereas noncontrast CT of the temporal bones is the modality of choice in the work-up of CHL, as described fully in the article by Drs. Martin and Hirsch, elsewhere in this issue. The less common clinical scenario of imaging patients with MHL has not received as much attention in the radiology or otolaryngology literature. MHL is characterized by a loss of hearing sensitivity by bone conduction accompanied by an even greater loss of sensitivity by air conduction . Clinical interpretation of patients presenting with elements of both CHL and SNHL is difficult and requires a combination of audiologic testing, case history, and clinical examination. Children presenting with MHL pose an even greater diagnostic challenge for several reasons, including delayed detection of the sensorineural component and inaccurate information obtained from audiologic testing, and the dynamic nature of MHL can lead to a confusing clinical presentation rendering imaging a crucial component of the work-up.
Although there are no specific guidelines for imaging MHL, the decision to use MRI versus CT in this complex clinical scenario should be based on the etiology of the MHL. Otosclerosis and osteogenesis imperfecta type 1 are among the more common diseases associated with MHL and are readily assessed with CT. In children, numerous syndromes have been described in association with MHL, including Treacher Collins syndrome (mandibulofacial dysostosis) and X-linked stapes gusher. Children may also present with occult SNHL during the work-up of a CHL secondary to otitis media. If the sensorineural component of MHL is not explained by the CT findings, the next step in the imaging work-up would be contrast-enhanced MRI of the internal auditory canals to better assess the membranous labyrinth and inner ear apparatus .
The authors believe that the evaluation of MHL should commence with noncontrast CT of the temporal bones in children and contrast-enhanced CT of the temporal bones in adults. Often, the sensorineural component of the MHL may be explained on the basis of the CT findings. Many diseases, such as perilymphatic fistulas, congenital inner ear anomalies in patients with superimposed causes of CHL, and trauma involving both the ossicular chain and otic capsule, can easily be detected on CT alone. In certain clinical scenarios, a combined approach to analyze the middle ear with CT and the inner ear with MRI might be needed. Interpreting physicians should be aware of rare but reported causes of inner ear CHL presenting as MHL . With respect to otosclerosis, the abnormalities are best characterized on high-resolution CT studies ( Fig. 7 ). MRI findings of otosclerosis are less well described but should be kept in mind when confronted with a clinical scenario that entails both SNHL and MHL ( Fig. 8 ). A ring of intermediate signal intensity in the pericochlear and perilabyrinthine regions on T1-weighted MR images associated with mild-to-moderate enhancement and increased signal on T2-weighted images has been described in association with cochlear otosclerosis .
Contrast-enhanced CT is the initial tool for the evaluation of adults with MHL. MRI should be invoked if the sensorineural component of the hearing loss cannot be explained with the CT findings.
Sinonasal tumors
CT is inarguably the imaging modality of choice for suspected sinonasal inflammatory disease. Sinonasal malignancies often present clinically in a manner similar to chronic benign inflammatory disease . When an aggressive sinonasal process is clinically suspected or incidentally detected on routine cross-sectional imaging of the head and neck, the next step usually involves dedicated sinonasal imaging with CT or MRI. Clinicians who are familiar with the relative strengths and weaknesses of CT and MRI are better able to tailor their diagnostic work-up in these clinical scenarios. CT excels at assessing the bony reaction to sinonasal malignancies, whereas MRI can more precisely outline disease extent into surrounding soft tissue structures . Often, a combined approach with CT and MRI is needed ( Fig. 9 ). MRI is not only superior in defining the soft tissue extent of the primary tumor but also offers more accurate assessment of suspected intracranial complications, skull base invasion, and perineural spread of tumor ( Fig. 10 ) . MRI is excellent at distinguishing dural involvement from parenchymal involvement ( Fig. 11 ) . Perhaps the most important information gained from using MRI in the work-up of sinonasal tumors is differentiating entrapped secretions from neoplasm, because CT is unreliable for this distinction (see Fig. 9 ) . Most sinonasal neoplasms demonstrate low-to-intermediate signal intensity on T2-weighted images, whereas entrapped secretions are often hyperintense. The more homogeneous signal pattern and peripheral enhancement often allow differentiation of tumor from even dense inspissated secretions. Tumor and entrapped secretions cannot reliably be differentiated on CT due to similar attenuation characteristics. Additional strengths of MRI include the ability to distinguish scar tissue from surgical material and recurrent tumors, as well as distinguishing neoplasms from polyps in patients with atypical CT findings .



