This article presents a systematic approach for interpreting a craniofacial CT scan that is clinically useful to the reconstructive surgeon. By categorizing the fracture patterns and highlighting the variables that may affect fracture management, the radiologist can expand his interpretation of the fracture pattern into a clinically useful diagnosis that may affect fracture management.
The management of facial fractures begins with the establishment of an accurate fracture diagnosis. All too often, radiology reports contain a “laundry list” of fractures without clinical context, without an understanding of fracture patterns, or without categorization by fracture severity, fracture criticality, or the need for surgical repair. For example, a radiology report that focuses on nasal septal fractures, but ignores a medial canthal avulsion, can be annoying or even misleading to the surgeon.
Fracture complexes are reproducible, and the terminology of fracture complexes allows for efficient communication between physicians of intricate fracture patterns in the midface. This type of communication requires that the radiologist understand common mechanisms of injury and the fracture complexes that result.
The best-known categorization scheme for fracture fractures is that of Rene Le Fort. However, Le Fort’s work was based on low-speed impact, and does not completely reflect the breadth of trauma that is encountered in modern medicine. The purpose of this issue is to provide a broader classification scheme for midface fracture complexes, which incorporates, and yet goes beyond, Le Fort’s classification. The goal is to encourage more clinically relevant radiology reports, so that surgeons will know what to expect, and radiologists will know what to provide, in the CT evaluation of facial fractures. Variables that affect surgical management will be emphasized. At the end of each section, there is a short list of pearls for creating clinically relevant radiology reports.
This issue is focused on midface fractures; mandibular and skull base fractures are intentionally excluded to retain this focus.
Frontal sinus fractures
Fractures of the frontal sinuses comprise about 5% to 15% of maxillofacial fractures . These fractures are generally classified by involvement of the anterior wall (anterior table) or posterior wall (posterior table). In addition, fractures of either wall may be comminuted or noncomminuted, and displaced or nondisplaced. Finally, involvement of either the nasofrontal duct or the anterior cranial fossa dura has important implications for the clinical management of these fractures.
The importance of the radiologic diagnosis of frontal sinus fractures is underscored by the fact that before the advent of routine CT scanning for head trauma, 50% of frontal sinus fractures were not identified until after the patient had left the emergency room . The frontal bone is the strongest of the facial bones, and a large amount of force (800 to 2200 lb) is required to fracture the frontal sinuses . The presence of frontal sinus fractures may therefore be considered an indicator of a high-force injury, and should alert the physician to search for other injuries. Additional craniofacial injuries are present in 56% to 87% of patients with frontal sinus fractures . An associated cerebrospinal fluid (CSF) leak is present in 13% to 33% of patients with frontal sinus fractures . Mortality secondary to other associated injuries has been reported at rates of approximately 9% of patients with frontal sinus fractures .
Structures involved
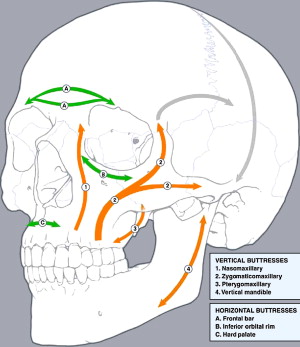
Each wall of the frontal sinus serves a dual function. The anterior wall of the frontal sinus, formed by the frontal bone, is responsible for the aesthetic contours of the forehead and the superior orbital rims. In addition, this structure serves as the frontal bar, one of the key horizontal buttresses of the facial skeleton ( Fig. 1 ). The frontal bar helps to maintain the horizontal dimension of the face and to provide a stable foundation for the vertically oriented facial buttresses (see Fig. 1 ) that support the forces of mastication. Fractures of the anterior table may be clinically important either by disrupting the aesthetic contour of the forehead or by destabilizing the frontal bar from which the other facial bones are suspended . The posterior wall of the frontal sinus forms the anterior wall of the anterior cranial fossa, and serves to separate the sinus contents from the cranial vault. Posterior table fractures are therefore skull fractures, and must be recognized and managed as such. The floor of the frontal sinus forms the medial orbital roof; it also houses the ostium to the nasofrontal duct in its posteromedial aspect . The nasofrontal duct forms the drainage pathway of the frontal sinus into the nose, so obstruction of this pathway can lead to mucocele, mucopyocele, osteomyelitis, and epidural or subdural abscess .
Variables affecting treatment
There are three main variables to consider when assessing the need for surgical intervention for frontal sinus fractures. These are involvement of the anterior table, disruption of the nasofrontal duct, and involvement of the posterior table. When assessing the involvement of the anterior or posterior tables, the degree of fracture displacement and comminution are also important. An additional factor involved when assessing the posterior table is the likelihood of dural penetration or nasofrontal duct disruption.
Anterior table fractures
Nondisplaced anterior table fractures require no surgical intervention. Displaced anterior table fractures may cause cosmetic deformity because of facial stepoffs, asymmetry, or flattening of the normally convex glabella. Repair of these defects is ideally performed within 10 days of the injury, a time during which soft tissue edema resulting from the trauma may mask the cosmetic deformity. Consequently, radiologic estimates of the degree of displacement of the anterior table and the resultant cosmetic deformity are critical in making the determination of whether to proceed with surgery.
Posterior table fractures
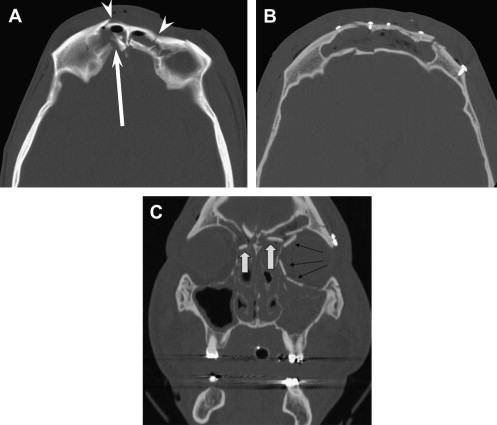
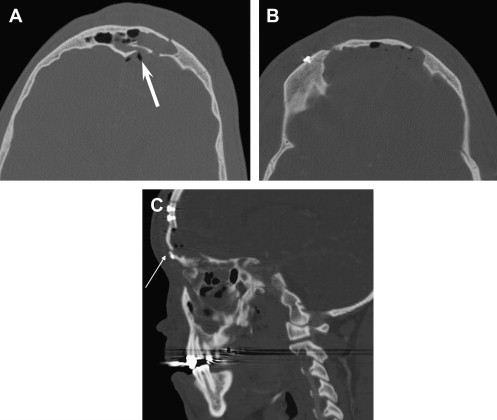
The management of posterior table fractures remains somewhat controversial. Nondisplaced posterior table fractures are frequently treated conservatively with close follow-up . Follow-up should include early and repeated CT scans of the sinuses . In contrast, comminuted or displaced posterior table fractures are generally felt to increase the risk of complications and thus merit exploration . The presence of pneumocephalus, although not specific, may indicate dural violation, and also may be an indication for surgical exploration of the fracture . Posterior table fractures may be managed with sinus obliteration if the floor of the sinus is not comminuted and there is not a large amount of bone missing ( Fig. 2 ). Severely comminuted or displaced posterior wall fractures frequently require cranialization ( Fig. 3 ) .
Involvement of the nasofrontal duct
If the nasofrontal duct is disrupted, operative intervention is necessary. A few recent reports suggest that conservative management with an endoscopic Lothrop procedure when necessary to reestablish the frontal sinus drainage pathway may be an option; however, the most trusted method of management is to obliterate the sinus and nasofrontal duct ostium . Disruption of the nasofrontal duct may be difficult to assess on CT, and intraoperative exploration is often necessary to make the final determination of future nonfunction of the duct. However, the CT report should indicate the likelihood of duct disruption based on the location and degree of displacement of the fracture. Nasofrontal duct disruption is most likely in cases where there is a displaced anterior table fracture medial to the supraorbital notch and involving either the floor of the frontal sinus, the naso-orbital-ethmoidal (NOE) complex (see “Naso-orbital-ethmoidal (NOE) fractures”), or both .
Clinically relevant radiology reports: Frontal sinuses
- 1.
Indicate whether the fracture involves the anterior wall, posterior wall, or both, as well as the degree of displacement and comminution of the fracture.
- 2.
For posterior wall fractures, indicate the presence or absence of pneumocephalus with an estimation of the likelihood of dural violation and the degree of bone loss in the posterior wall and floor of the sinus.
- 3.
Indicate the likelihood of nasofrontal duct obstruction based on the fracture location.
- 4.
Comment on any associated brain injury. This is especially important for posterior table fractures.
Zygomatico-maxillary complex (ZMC) fractures
The malar eminence of the zygoma is the most anterior projection of the lateral face. This prominent position makes the zygoma susceptible to trauma; one study demonstrated zygomatic complex fractures to be the most common type of facial fracture in patients admitted to the hospital following blunt facial trauma . The central portion of the zygomatic bone is sturdy, and contributes to the vertical buttress system of the midface (see Fig. 1 ); however, the projections of the zygoma by which it articulates with the surrounding facial bones, and the articulating bones themselves, are weaker. This often results in fracture of the zygoma at its suture lines, classically labeled as a “tripod” fracture in reference to the three anterior suture lines that are fractured: the zygomaticfrontal (ZF), zygomaticotemporal (ZT), and zygomaticomaxillary (ZM) sutures ( Fig. 4 ). However, the zygoma has a fourth articulation site with the sphenoid bone, which is also fractured, and radiographically, five distinct fractures are demonstrated (lateral orbital wall, orbital floor, anterior maxillary wall, lateral maxillary wall, and zygomatic arch). Thus, the name “tripod fracture” is technically inaccurate. A more compelling reason to avoid the term “tripod fracture” is because it fails to recognize that this fracture complex is intermediate on a spectrum of injuries that range from an isolated, nondisplaced fracture limited to the zygomatic arch to severe displacement and comminution of the zygoma and surrounding bones. This spectrum of fractures all have similar mechanisms of injury, but differ in the amount of force applied and therefore in the degree of bone loss and displacement . For this reason, it is preferable to classify this entire spectrum of fractures together as zygomaticomaxillary complex (ZMC) fractures.
Structures involved
The zygoma is an approximately quadrilateral-shaped bone. The body of the zygoma forms the malar prominence, which is an important aesthetic feature of the face. A prominent malar eminence has been described as “a sign of youth and beauty” . Through its attachments to the surrounding facial bones, the zygoma also helps to determine midfacial height and width . From the laterally oriented malar prominence, the zygoma sends four projections that articulate with the surrounding facial bones. Superiorly, the zygoma articulates with the frontal bone at the narrow frontozygomatic suture; medially, it has a wider articulation with the maxilla, involving both the anterior and lateral walls of the antrum. The curved bony strut of the zygoma lying between these superior and medial projections forms the lateral orbital wall and the lateral aspect of the infraorbital rim and orbital floor. Posteriorly, the zygoma articulates with the sphenoid bone, and laterally it extends as the zygomatic arch to attach to the temporal bone at the zygomaticotemporal suture.
The presence of the thick bone of the zygoma at the lateral corner of the midface allows it to act as a cornerstone to provide support to the other facial bones . The maxilla directly contacts the frontal bone at the frontomaxillary suture line and the sphenoid bone posteriorly above the maxillary tuberosity and anterior to the sphenopalatine foramen. The zygoma then overlies and reinforces this area through its attachments to the underlying frontal, maxillary, sphenoid, and temporal bones.
Variables affecting treatment
The goal of reconstruction in ZMC fractures is to restore the height, width, and projection of the malar eminence. The degree of fracture displacement and comminution determines the extent of the surgical exposure needed for repair. Nondisplaced and minimally displaced fractures frequently do not require surgical intervention . Displaced and comminuted fractures generally require open reduction and fixation. The first and most critical step in management of ZMC fractures is achieving adequate reduction . When fractures are not significantly comminuted, as is the case in a classic tripod fracture, the entire zygoma may be reduced as a single unit. In such cases, ZMC fractures may be managed through the use of limited incisions, in particular an upper gingivobuccal (UGB) incision and a lateral upper blepheroplasty (LUB) incision. Reduction can, in these cases, be accurately assessed by confirming reduction at the ZM suture (through the UGB incision), the ZF suture (through the LUB incision), and the ZS suture (through the LUB incision).
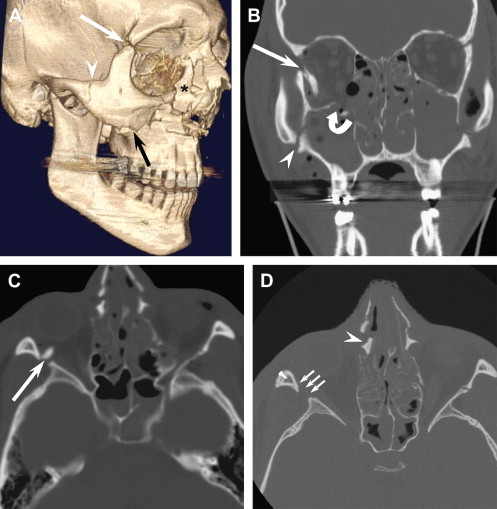
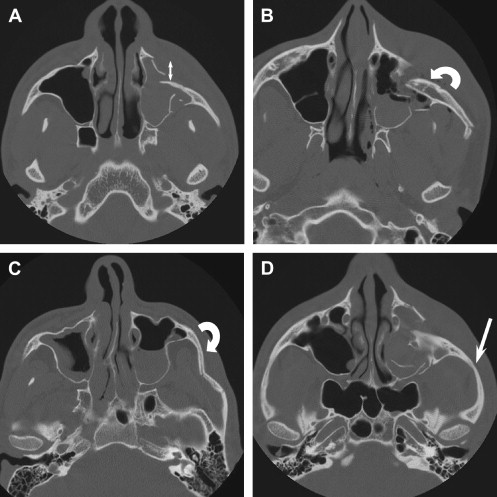
Accurate depiction of ZMC fracture displacement can be accomplished with CT ( Fig. 5 ). The malar eminence is often displaced posteriorly, but the degree of displacement may be masked clinically by soft tissue swelling (see Fig. 5 A). The malar eminence may be rotated internally or externally (see Fig. 5 B, C). Occasionally, the zygomatic arch fracture that accompanies ZMC fractures will not be evident radiographically as a discrete linear hypodensity. Abnormal curvature of the zygomatic arch should be considered equivalent to a discrete fracture in this setting (see Fig. 5 D).
Accurate reduction is more difficult to assess in comminuted fractures. When the zygoma itself is comminuted, it cannot be reduced as a single unit, and accurate reduction at one suture line does not imply adequate reduction at the others. In such cases, additional incisions may be necessary for fracture reduction and fixation. Eyelid incisions (ie, transconjunctival incision with a lateral canthotomy or subciliary incision) provide exposure to the orbital rim. A coronal access incision may be necessary for wider exposure of the zygomatico-sphenoid suture line, lateral orbit, and zygomatic arch. In addition, the high-energy trauma required to create comminuted zygoma fractures frequently also results in comminuted fractures of the surrounding bones. Le Fort, NOE, and panfacial fractures frequently coexist with ZMC fractures . Identification of these coexisting fractures is critical for determining accurate reduction of the ZMC. Failure to recognize coexisting fractures may mislead the surgeon into aligning the ZMC with another segment of the buttress system that is itself displaced; this in turn may result in postoperative cosmetic deformity .
Another major variable affecting the surgical management of ZMC fractures is the status of the orbital floor. The zygoma contributes to both the lateral and the inferior orbital walls. Displacement of these walls frequently occurs in ZMC fractures, and may result in an increased volume of the bony orbit. This increase in orbital volume is the most common cause of posttraumatic enophthalmos . Restoration of the pretrauma orbital volume is therefore a primary goal of ZMC fracture management. Before the advent of routine CT scanning for these injuries, the decision of whether or not to explore the orbit was made on a clinical basis. CT scan has been shown to be a reliable method of making the decision of which orbits require exploration . The ability to make this determination based on the CT scan allows those patients without significant orbital volume expansion to be spared the morbidity of a subcilliary or transconjunctival incision. Some degree of ectropion and scleral show may complicate as many as 20% of these incisions . Radiologic criteria suggesting the need for orbital exploration include severe comminution or displacement of the orbital rim, displacement of greater than 50% of the orbital floor with prolapse of the orbital contents into the maxillary sinus, an orbital floor fracture greater than 2 cm 2 , and the combination of an inferior and medial wall fracture . Based on these or similar criteria, approximately 30% to 44% of patients with ZMC fractures require an orbital incision .
A final variable to consider in ZMC fractures is the status of the orbital apex. The orbital apex is the posterior portion of the orbit that contains the optic nerve and lies in close apposition to the internal carotid arteries and cavernous sinuses. Injury to this area may result in a number of serious injuries resulting from injury to the carotid arteries and to cranial nerves II, III, IV, V1, and VI . The lateral wall of the orbital apex is formed by the greater wing of the sphenoid. This bone also contributes to the lateral orbital wall and articulates anteriorly with the zygoma. ZMC fractures may result in displacement of the greater wing of the sphenoid . It is important to note whether this displacement occurs laterally or medially (into the orbital apex). The medial wall of the orbital apex is formed by contributions from the ethmoid and palatine bones and the body of the sphenoid bone. Fractures in these areas should also alert the radiologist to possible orbital apex involvement.
Clinically relevant radiology reports: ZMC fractures
- 1.
Recognize that a range of injuries from an isolated zygomatic arch fracture, to a classic tripod fracture, to a displaced, comminuted zygoma all represent fractures of the zygomaticomaxillary complex (ZMC).
- 2.
Comment on the degree of displacement and comminution of the ZMC fracture. The more displaced and the more comminuted the involved bones are, the more complex the surgical repair with a need for wider surgical exposure and more points of fixation.
- 3.
Comment on the extent of orbital involvement. Fractures involving more than 50% of the orbital floor will likely require open reconstruction.
- 4.
Identify whether the medial orbital wall (lamina papyracea) is involved. An isolated medial orbital wall fracture is generally not a cause of clinically significant orbital volume loss; however, when found in combination with a floor fracture, it may require repair.
- 5.
Comment on the involvement of the orbital apex and the direction of displacement of the lateral orbital wall.
Zygomatico-maxillary complex (ZMC) fractures
The malar eminence of the zygoma is the most anterior projection of the lateral face. This prominent position makes the zygoma susceptible to trauma; one study demonstrated zygomatic complex fractures to be the most common type of facial fracture in patients admitted to the hospital following blunt facial trauma . The central portion of the zygomatic bone is sturdy, and contributes to the vertical buttress system of the midface (see Fig. 1 ); however, the projections of the zygoma by which it articulates with the surrounding facial bones, and the articulating bones themselves, are weaker. This often results in fracture of the zygoma at its suture lines, classically labeled as a “tripod” fracture in reference to the three anterior suture lines that are fractured: the zygomaticfrontal (ZF), zygomaticotemporal (ZT), and zygomaticomaxillary (ZM) sutures ( Fig. 4 ). However, the zygoma has a fourth articulation site with the sphenoid bone, which is also fractured, and radiographically, five distinct fractures are demonstrated (lateral orbital wall, orbital floor, anterior maxillary wall, lateral maxillary wall, and zygomatic arch). Thus, the name “tripod fracture” is technically inaccurate. A more compelling reason to avoid the term “tripod fracture” is because it fails to recognize that this fracture complex is intermediate on a spectrum of injuries that range from an isolated, nondisplaced fracture limited to the zygomatic arch to severe displacement and comminution of the zygoma and surrounding bones. This spectrum of fractures all have similar mechanisms of injury, but differ in the amount of force applied and therefore in the degree of bone loss and displacement . For this reason, it is preferable to classify this entire spectrum of fractures together as zygomaticomaxillary complex (ZMC) fractures.



