As cochlear implant technology has changed, so have implantation criteria. In addition to profoundly deaf individuals, candidacy has expanded to include those with significant remaining acoustic hearing. This article describes the devices that are now in clinical trial, discusses the rationale as to why residual hearing preservation is important, details the surgical techniques for hearing preservation, and shares the clinical results of electric plus acoustic processing. That a video is available online.
Video of Surgical Technique for Hearing Preservation accompanies this article at http://www.oto.theclinics.com/ .

In the past 30 years, cochlear implantation has changed from being an experimental procedure to representing the standard of care. Advances in processing strategies, implant design, and patient selection criteria have improved implant users’ performance significantly. The current frontiers in implantation involve strategies to preserve residual acoustic hearing and the development of algorithms to combine electrical and acoustic hearing. It is also important to consider preserving apical Organ of Corti structures to take advantage of new developments that might lead to regeneration of the inner ear in the future.
Cochlear implantation with a standard-length electrode has become a routine treatment for profound deafness; however, interest is mounting to expand electrical speech-processing capabilities to those individuals with more residual acoustic hearing, as those with implants demonstrate significantly better speech understanding than severely hearing–impaired individuals using hearing aids. Over the past 10 years, individuals with substantial low-frequency acoustic hearing below 1500 Hz have received varying electrode designs, including shortened cochlear implants, in an attempt to preserve this remaining inner ear function. These patients have not been considered candidates for implantation using standard criteria, due to their residual low-frequency hearing. However, patients with severe to profound high-frequency hearing loss above 1500 Hz and relative preservation of low-frequency hearing do poorly, even with bilateral amplification. This loss of fidelity occurs because different qualities of sound are encoded in various frequencies of sound energy. In the low frequencies, information about vocal fold vibration is relayed (ie, the ability to distinguish between “s” and “z”), whereas frequencies above 1000 Hz encode information regarding the vocal formants and spectral patterns (such as the difference between “b” and “g”). The information provided by the low frequencies requires only that the patient be able to distinguish differences in loudness and speech patterns, whereas the information provided in the high frequencies requires the listener to distinguish between various spectral patterns. Patients with high-frequency losses are able to use loudness and speech pattern cues, but they lack the ability to distinguish differences in spectral patterns. This particular hearing-loss pattern results in significant reductions in word discrimination scores as the ability to distinguish between the different consonant sounds erodes. Amplification of these frequencies is insufficient to improve speech recognition scores when thresholds exceed 55 dB.
Electric and acoustic hearing
Shortened Electrodes
In many patients with some residual hearing, cochlear implantation with a standard-length electrode and standard surgical technique results in complete loss of the remaining acoustic hearing. However, in 1997 Hodges and colleagues reported on a series of patients who had preserved residual hearing after implantation. Since that time, multiple studies have demonstrated the ability to retain residual low-frequency hearing following standard-length electrode implantation. However, it is difficult to maintain speech discrimination in addition to pure tones when electrodes are passed beyond the basal turn. Passing a standard-length electrode beyond the basal turn of the cochlea can result in damage to the organ of Corti, due to migration of the electrode through the basilar membrane.
The development of acoustic plus electric hearing has evolved from the work of two independent groups of researchers from the Iowa Cochlear Implant Clinical Research Center in Iowa City, Iowa, USA, and the Johann-Wolfgang-Goethe-University in Frankfurt, Germany.
In 1995, the University of Iowa CI research team began the development of a shortened electrode array, or Hybrid S, in collaboration with the Cochlear Corporation (Lane Cove, Australia). The goals and theories behind development of the short electrode are fundamentally different than merely inserting a standard-length electrode into the cochlea under modified technique. The Hybrid project stemmed from work by Shepherd and colleagues that showed that preservation of the apical regions of the feline cochlea could be spared anatomically and functionally following limited electrode insertion. The Hybrid electrode was thus intentionally designed to only insert into the lower basal turn of the cochlea and stimulate the missing areas of high frequency in subjects with steeply descending audiograms. The design was predicated on the concept that once the electrode was advanced beyond the upper basal turn it could not be controlled, and could migrate through the basilar membrane as it was advanced against the lateral wall. Limiting the length of the electrode prevents this type of damage. The electrode is specifically intended for patients with good to excellent low-frequency thresholds but severe to profound loss in the higher frequencies. The concept of hearing preservation and cochlear implantation was first presented at the National Institutes of Health-National Institute on Deafness and other Communication Disorders Tenth Anniversary celebration meeting in late 1998. The first volunteer was implanted under the initial US Food and Drug Administration (FDA) trial in 1999.
The Hybrid-S electrode is smaller in diameter than the standard electrode, measuring 0.2 mm × 0.4 mm ( Fig. 1 ). Other modifications include a Dacron washer positioned to prevent the electrode from insertion past the 10-mm mark, and a titanium marker to orient the electrodes toward the modiolus. The initial electrode was 6 mm in length and contained 6 electrodes. The most important finding in the original 3 volunteers receiving the 6-mm device was the ability to preserve residual acoustic hearing close to their preoperative levels. Two of the subjects complained that the sound was very high-pitched and not very useful. The initial electrode design was then lengthened to 10 mm, with 6 electrodes within the distal 6 mm. The ideal insertion depth is approximately 195° of the basal turn of the cochlea.

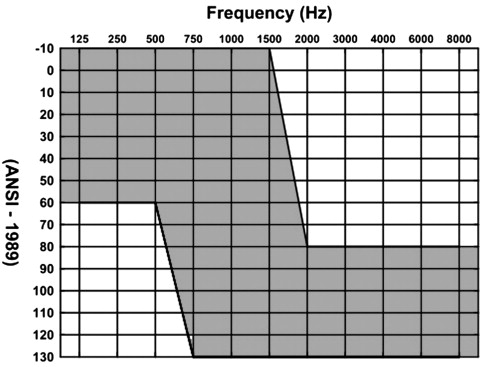
Candidates for implantation with this shorter electrode must have less than 60 dB hearing loss between 125 and 500 Hz and less than 80 dB hearing loss above 2000 Hz. Further, they may have substantial consonant nucleus consonant (CNC) word scores in the best aided situation between 10% and 60% correct in the worse hearing ear and up to 80% correct in the better hearing ear ( Fig. 2 ).
In 2003, Gantz and Turner reported on the first 6 patients implanted with the Hybrid electrode. Three volunteers received the 6-mm electrode and 3 received the 10-mm electrode. All patients had normal to mild hearing loss up to 750 Hz. All patients had preservation of their residual hearing. Patients receiving the 6-mm electrode saw a benefit of 10% in the consonant recognition scores, whereas those who received the 10-mm electrode improved by 40% on average within the first year following implantation. The final results of the initial feasibility study included the original 6 patients plus 3 more who received the 10-mm device. All 9 patients had preserved low-frequency hearing within 15 dB of their preoperative levels. Patients who received the 10-mm electrode did considerably better in the combined mode (cochlear implant + hearing aids in bilateral ears) than those who received the 6-mm electrode. Of the 4 patients implanted with the 10-mm electrode after 12 months or more of follow-up, 3 scored more than 80% on CNC words in the combined mode.
Following the feasibility study, a larger multicenter phase 1 FDA trial was conducted for the Hybrid S 10-mm electrode. Eighty-seven patients were recruited at 13 medical centers. Preliminary data on long-term hearing outcomes was published in 2009. Two patients lost all residual hearing within 1 month of implantation for an initial hearing preservation rate of 98%. Over the course of the study (between 3 and 24 months after activation), 6 more patients lost residual hearing for a long-term hearing preservation rate of 91%. Over time, 30% of patients experienced low-frequency threshold changes of greater than 30 dB (between 3 and 36 months post activation).
In the Hybrid S trial, 16 patients (18% of the subjects) did not improve or worsened on performance measures. A multivariate analysis was performed to determine which factors negatively influenced the outcomes for the poor-performer group. A long duration of deafness (longer than 40 years) and low preoperative CNC word scores were found to negatively impact on functional outcomes ( Table 1 ).
| Cochlear Hybrid S10 | Cochlear Hybrid L24 | Med-El Flex EAS | |
|---|---|---|---|
| Number of patients | 87 | 32 total 24 implanted with L24 | 18 |
| Average length of follow-up, months (range) | 9–12 (3–36) | Not stated 16 patients completed testing at 12 mo 22 patients had reached 6 mo | 15 (range not given) |
| Average change in threshold | 13.5 dB (n = 80) | 10 dB | Not given |
| % within 30 dB of preoperative thresholds | 70% | 94% | 66% |
| Number with complete loss of residual hearing | 2 immediate; 6 delayed | None | 3 delayed |
| Average word scores | 73% on CNC words | 45.1% on FMT | 44% on FMT 71% on open-set sentences |
Another short electrode has been developed in conjunction with the Cochlear Corporation, the Hybrid L24, which is 16 mm in length and contains 22 electrodes (see Fig. 1 ). The optimal insertion is through 250° of the basal turn of the cochlea. This longer electrode would still preserve residual hearing in the apical portions of the cochlea, but if the low-frequency hearing is lost the Hybrid L can be used as a traditional electric-processing only device as it has 22 electrodes, similar to a standard electrode. The FDA trial for the Hybrid L is closed and is now accruing data. Preliminary results from the European clinical trial with this electrode have been published recently, and demonstrate the ability to preserve residual hearing (see Table 1 ). The European trial included 32 patients, 24 of whom were hybrid candidates and 8 long-electrode candidates. Hearing was preserved within 30 dB of preoperative thresholds in 96% of patients, and 68% were within 15 dB. These results were stable over time. Of the 16 patients with 12 months of experience, 94% retained hearing within 30 dB of preoperative thresholds. The ongoing US trial of the L24 electrode is demonstrating similar hearing preservation rates to the S8 US trial. This study also noted a negative impact from prolonged duration of hearing loss. It additionally confirmed the findings from the Hybrid S trial that there is a significant learning period for patients with short electrodes. Those in the European trial showed significant improvement on word scores between the 6-month and 12-month marks.
The Med-El Corporation (Innsbruck, Austria) has also developed a shortened electrode for electric and acoustic hearing. Their standard-length electrode, the Combi40+, has a goal insertion length of 31 mm. The shortened electrode, the M, is 22 mm in length and its goal insertion is 360° through the basal turn of the cochlea. Recent adaptations of the electrode include a significantly reduced diameter of the distal portion of the electrode and a very flexible tip. This Flex EAS electrode can be used for both cochleostomy and round window insertion techniques. Much of the data regarding the Med-El system involves mixed cohorts of patients.
Before the development of the shortened electrode, surgeons in Europe were using a standard-length electrode but limiting the depth of insertion. Therefore, results regarding the shortened electrode from several studies are difficult to interpret. However, results related to the M electrode specifically were reported in 2008 (see Table 1 ). In this series, 18 patients were implanted with the M device. Twelve of the 18 (66%) had low-frequency hearing preservation that could be usefully amplified. Three other patients had some residual low-frequency hearing but did not find amplification useful. Three patients (16%) lost all residual hearing. Of interest, the loss of residual hearing was not immediate, but delayed by 3 to 6 months after hybrid activation. Of the 18 patients implanted, 6 used the hybrid mode on a regular basis.
Standard-Length Electrodes
The ability to preserve residual acoustic function rests in both the type of electrode used and the techniques with which it is inserted. An alternative strategy for hearing preservation has been developed with standard-length electrodes. Kiefer and colleagues reported on 14 patients implanted with the Med-El Combi 40+ electrode. Depth of insertion was intentionally limited to less than 24 mm (full insertion is 31.5 mm) and a “soft insertion” technique was used. Useful low-frequency hearing (less than 20 dB change in thresholds) was maintained in 12 of 14 patients, with 2 patients losing all residual hearing. Fraysse and colleagues reported on a multicenter prospective trial using the Nucleus 24 Contour Advance electrode. The optimal insertion depth was 450° from the cochleostomy. Twenty-seven patients were implanted during the study, but only 12 had no deviations from the reported surgical protocol. Approximately 40% of patients lost the residual hearing completely, and only 19% to 33% (depending on frequency tested) of patients retained hearing thresholds within 20 dB of preoperative scores. Using modified surgical techniques and standard-length electrodes, other investigators have reported preserved hearing within 20 dB of preoperative thresholds in 67% to 89% of patients. However, not all of these patients retain the ability to discriminate. Balkany and colleagues reported that although patients experienced an average of only 15 dB change in the low frequencies, the average acoustic CNC word score postoperatively was 0%. This result was statistically significant ( P <.001). In all of the previously mentioned studies, the electrodes were inserted through the entire basal turn of the cochlea. The optimal depth of insertion for the Nucleus 24, a perinodular 19-mm electrode, is between 450° and 540° (see Fig. 1 ). The Med-El Combi 40+ has a goal insertion of 31 mm. Prentiss and colleagues have reported on their experience with deep electrode insertion with the goal of acoustic hearing preservation. Eighteen patients were implanted with the Med-El Pulsar100 to depths of 24 to 28 mm. All patients retained some acoustic hearing, with 16 of 18 patients within 30 dB of their preoperative thresholds.
Discussion
There is controversy in the literature about which electrode length is preferred. There is a higher rate of reduced thresholds and anacusis with the long electrodes. Some investigators argue that the long electrodes should be used for this reason, so that if residual hearing is lost the patient can have the full-length electrode to use in an electric-only listening mode.
The short electrode, at 10 mm in length, accesses only the 2800- to 4700-Hz range according to the Greenwood frequency-place map of the basilar membrane. Thus, using the electrode in the electric-only listening mode should cause significant tonotopic place mismatch. While this mismatch causes decreased word discrimination in normal-hearing listeners, Hybrid S electrode users in the electric-only mode performed similarly to long-electrode users on consonant recognition tasks. Improved performance with the shorter10-mm Hybrid electrode does require a longer adaptive time. Patients continue to improve even after the first 12 months of use. Long-electrode users frequently require between 6 and 12 months to adapt to electric hearing.
Another argument in favor of implanting patients with a longer electrode is the likelihood of progressive low-frequency hearing loss. Yao and colleagues retrospectively reviewed the audiometric records of 28 patients who met the criteria for implantation with a Hybrid electrode. Linear regression analysis of each patient’s thresholds over time at each frequency from 250, 500, 750, 1000, and 2000 Hz was performed. The average for several groups was then calculated: more than 10 years of data, less than 10 years of data, age greater than 45 years at initial audiogram, and age less than 45 years at initial audiogram.
This study demonstrated no difference in the rate of change between the two groups based on age. Patients with less than 10 years of data had very wide standard deviations as a result of having fewer data to analyze. However, the rate of change was similar between all groups. The average rate of change for all frequencies was 1.05 dB per year. These data suggest that low-frequency hearing is relatively stable over time despite severe/profound loss in the high frequencies. If low-frequency hearing can be preserved at the time of operation, it is likely that the patient will experience minimal further hearing loss in the long term.
Another concern in regard of the Hybrid or electrode acoustic stimulation (EAS) studies is the progression of hearing loss after activation of the electrical processing. At the time of implantation, very few patients lose all of their residual acoustic hearing. Only 2 of 87 (2%) lost all hearing with implantation in the phase 1 Hybrid S10 trial. Between activation and 3 months, 9 of 87 (10%) subjects experienced a 30 dB drop in their pure-tone average at 125, 250, and 500 Hz. The cause of this loss is not known. Originally it was thought that this could be an immune reaction to the electrode; however, that now seems unlikely. Another possibility is loss of afferent spiral ganglion neuron synapse at the hair cell related to the combination of acoustic amplification and electrical stimulation. Puel and colleagues and Wang and colleagues have reported this finding as the initial injury in noise-induced hearing loss. This mechanism of delayed hearing loss is presently under investigation at the authors’ center. The authors are also adapting programming strategies to protect the residual structures by reducing the stimulating current at initial activation and widening pulse rates.
Benefits of acoustic and electric processing
The full benefits of acoustic and electrical stimulation of the ipsilateral cochlea are still being investigated. However, the available literature suggests several discrete advantages to the use of both modalities. There is a significant body of literature that reports on the benefits of “bimodal” hearing. In this situation, the user receives electrical stimulation in the implanted ear and uses a hearing aid in the contralateral ear. A full review of this listening condition is beyond the scope of this article. The reader is referred to a review on the subject by Firszt and colleagues for more detailed information.
The benefits of “combined” hearing are discussed here. In this situation, the user receives electric stimulation in the implanted ear as well as acoustic information through the use of bilateral hearing aids. Improvements in speech discrimination, signal-to-noise ratio (SNR), and music perception are discussed.
Speech Discrimination
As discussed previously, patients with preserved low-frequency hearing have significant improvements in their discrimination scores. Those implanted with shorter electrode arrays, such as the Hybrid S/L or Med-El M/Flex EAS electrodes, are achieving significant improvements in discrimination tasks as well. Patients implanted with the Hybrid S electrode continue to demonstrate improvement in CNC scores beyond 1 to 2 years after activation in the combined mode. At the time of publication of the Hybrid 10 clinical trial, 68 of 87 patients in the multicenter trial had follow-up lengths of greater than 9 months. Improvements in speech reception threshold (SRT) or CNC word score occurred in 74% of patients. Nearly half of patients (48%) had improvement in both SRT and CNC scores. Improvement on CNC testing ranged from 10% to 70% better than preoperative scores for 45 of 61 patients with long-term follow-up. For those implanted with the Hybrid L24, word recognition scores improved by 21% on average; one patient demonstrated improvement from 5% to 95% on the Freiburg Monosyllabic word test (FMT).
Some patients score more than 90% on the CNC monosyllabic word test in the combined mode with all electrodes. Patients implanted with the Flex EAS electrode also scored well. Preoperative open-set sentence recognition was 24% and after 12 months of use, scores averaged 71% ( P <.05). Monosyllable recognition also improved; preoperative scores averaged 16% on the FMT and postoperative scores averaged 44% ( P <.05). One patient in this cohort achieved scores above 90% discrimination postoperatively. As demonstrated in multiple studies, exceptional improvement in speech understanding is possible for patients in the combined mode with all electrodes activated.
Patients receiving long electrodes with preserved low-frequency cochlear function also routinely improved on discrimination tasks. Patients receiving the Med-El Combi40 with 19 to 24 mm of insertion scored 75% on monosyllabic words at 1 year; preoperative scores averaged 9%. Fraysse and colleagues reported on those receiving a Nucleus 24 Contour Advance. Preoperative word scores averaged 15%. At 3 months, patients in the combined condition had improved to 55%. Long-term data for this patient group are not available, but patients may continue to improve in the combined condition as is seen in other studies.
Hearing in Noise
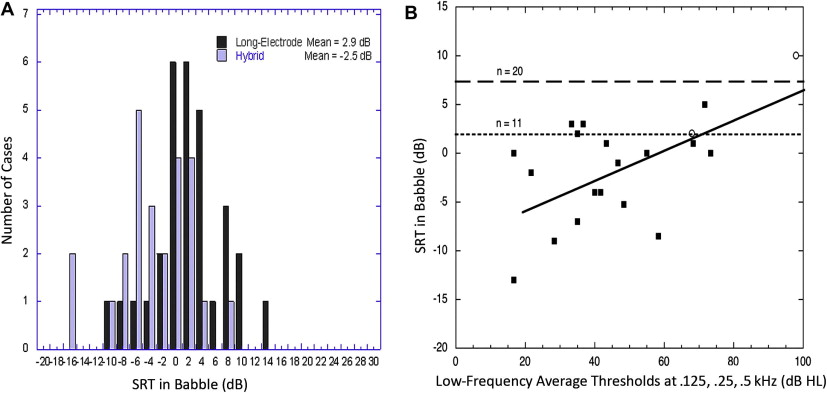
Although cochlear implants significantly improve speech understanding in quiet, traditional cochlear implant users have difficulty in noisy environments. Distinguishing the correct words in a background of competing talkers is an even more difficult task. Normal-hearing listeners are able to understand 50% of the presented words when the background noise is 30 dB louder; thus normal-hearing listeners have an SNR of −30 dB (lower numbers are better). For competing talkers, the average SNR in normal-hearing listeners is −15 dB. The average long-electrode user requires an SNR of +3 dB for unmodulated background noise and +8 for multitalker babble (MTB), meaning that the talker has to be 3 dB louder than competing noise or 8 dB louder than MTB.
Hybrid S recipients do better than traditional cochlear implant patients but not as well as normal-hearing listeners in background noise. SNRs varied from −12 to +17 dB in a subgroup of 27 Hybrid S patients with 12 months or greater experience. The average SNR for the Hybrid S group was −9 dB. Elevated SNRs occurred in those patients who experienced greater than 30 dB changes to their low-frequency hearing. The results for Hybrid S patients in MTB are similar to hearing-impaired patients with SRTs between 81 and 100 dB (severe/profound) ( Fig. 3 ).